
Abstract
This study investigates the effects of early fitting in trans-tibial amputees. The assumption is that compared to elastic bandaging, the use of a rigid dressing in early fitting will result in quicker wound healing and earlier ambulation. A retrospective file search was carried out in three different hospitals, analysing the time to first prosthesis, the incidence of local and general complications and the functional outcome after discharge from hospital. Each of the hospitals used a different method of postoperative care: elastic bandaging, immediate postoperative application of the plaster cast or delayed application of the plaster cast within one week post amputation. In comparison to the elastic bandaging method (N=52), the use of a rigid dressing in the early fitting method (immediate and delayed, N=97) resulted in a statistically significant shorter period from amputation to the delivery of a first regular prosthesis (110 days vs 50 days) and a decreased risk of knee flexion contracture. Although, differences in local complications were not observed, the risk of pressure sores in other places than the stump was increased in early fitting. Instead of further reducing the time to first prosthesis by immediate fitting, the use of delayed fitting resulted in a statistically significant shorter period from amputation to the delivery of a first regular prosthesis (56 vs 40 days). However, delayed fitting was associated with an increased risk for reamputation. In conclusion, this study indicates that early fitting by use of a rigid dressing after trans-tibial amputation is the treatment of choice. If it is possible to apply a plaster cast in the operating room, the authors would prefer the immediate fitting method.
Introduction
Despite continued advances in preventive foot care and increased possibilities in reconstructive surgery, trans-tibial amputation is still a sequela of irreversible ischaemia. The challenge in postoperative care for both the patient and the physician is to regain walking ability with a prosthesis. Prior to the delivery of the prosthesis, the stump has to meet certain criteria; the wound must have healed, the oedema must have been resolved, the stump should be conically shaped and stump maturation should be achieved. The two most frequently used postoperative strategies that are carried out to meet these criteria are the elastic bandaging method and the rigid dressing method with plaster of Paris. In the “elastic bandaging method” the stump is wrapped with an elastic pressure bandage to reduce the oedema and to shape the stump. Only when stump volume is constant, is a regular prosthesis fitted. This method influences the reduction of stump oedema, the stump formation and to some extent the stump maturation. In “the early fitting method” the stump is covered with a rigid dressing (plaster cast socket in this study), and a temporary prosthesis is provided. Early fitting can be divided into two sub-groups according to the time of starting with the rigid dressing. In the first method, called “immediate fitting”, the fresh stump is covered with a cast socket immediately after surgery, whereas in the second method, called “delayed fitting”, postoperatively the stump is covered with an elastic wound dressing while the cast socket is only applied at a later time (within a maximum of 1 week). This delay is because in some hospitals there are practical problems of casting in the operating theatre. The plaster cast is assumed to improve the wound healing (Baker et al. 1977; Kraeger 1970; Mooney et al. 1971; Moore et al. 1972; Vigier et al. 1999). Furthermore compared to elastic bandaging, the assumed advantage is that it prevents oedema instead of reducing it (Baker et al. 1977; Burgess et al. 1965; Condon and Joro 1969). Finally patients regain walking ability sooner (Folsom et al. 1992; Harrington et al. 1991; Kraeger 1970; Moore et al. 1972; Wong and Edelstein 2000), knee flexion contracture can be prevented more efficiently (Harrington et al. 1991) and they suffer less general complications, because of a quicker mobilization (Moore et al. 1972). Some authors report disadvantages of an early cast socket, such as increased risk for pressure ulcers because of tightness of the plaster and a delay in detecting wound problems (Cohen et al. 1974).
Most literature about early fitting dates from the 1960s, 70s and 80s. In these studies positive as well as negative effects have been reported, but the methodological quality of the studies is insufficient to draw a firm conclusion about the effectiveness of early fitting. The studies are often non-controlled (Burgess and Romano 1968; Condon and Jordan 1969; Kraeger 1970) or only descriptive (Burgess et al. 1965). Moreover, the level of amputation or surgical technique varies in several trials, (Burgess and Romano 1968; Cohen et al. 1974; Folsom et al. 1992; Kraeger et al. 1970) making it more difficult to understand the effect of early fitting.
The current study is designed as a retrospective case-control study (with selection of control subjects from other hospitals), comparing the effects of early fitting with a rigid dressing and elastic bandaging. The authors hypothesise that trans-tibial amputees treated with “early fitting” have a quicker stump healing time, have less local and general complications and can function more independently than patients treated with “elastic bandaging”. Furthermore it is hypothesized that compared to “delayed fitting”, the “immediate fitting” method is associated with faster stump healing and with less local and general complications, because in immediate fitting the oedema is prevented instead of reduced and because ambulation using a temporary prosthesis starts earlier.
Methods
Study design
This is a retrospective case control study. The authors did not match the individual patients but restriction was used in order to allow comparison of three hospital based cohorts. All consecutive trans-tibial amputees between January 1997 and December 1999 in three large teaching hospitals in the east of the Netherlands where enrolled into the study. The follow-up period of patients was one year. The diagnosis was verified according to the code for national illness registration SIG. Clinical data were collected from medical files of the medical and rehabilitation wards and from general clinical or nursery files. Data for prosthetic fitting were provided by the local orthopaedic technicians.
Subjects
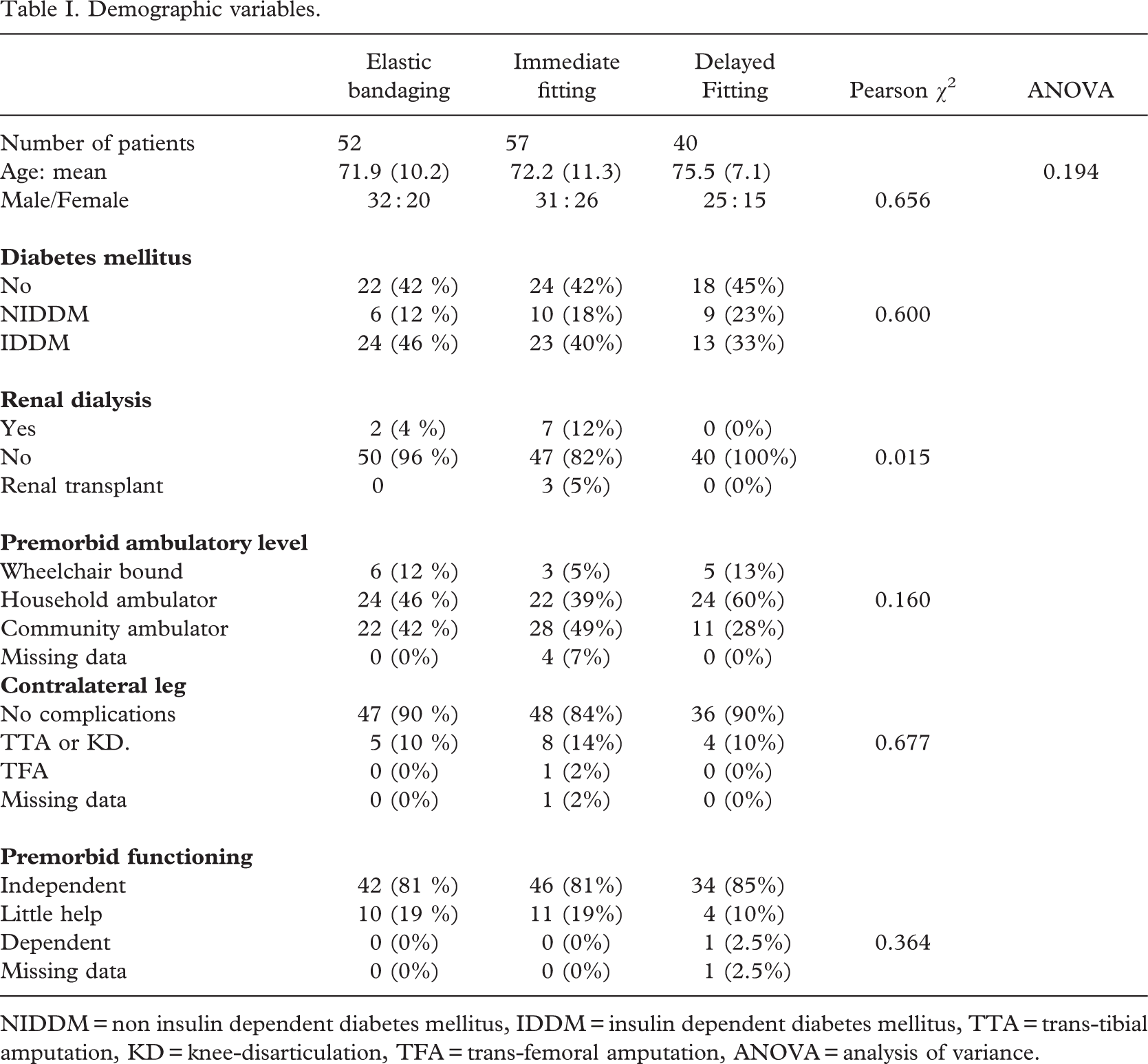
The study population consisted of patients with a trans-tibial amputation due to vascular insufficiency. Patients suffering from dementia, a paresis MRC grade 3 or less in one or more limbs and patients with an amputation of the contralateral leg within one year after the amputation were excluded. Demographic and clinical baseline characteristics are depicted in Table I.
Treatment procedures
In all hospitals the long posterior flap technique, as described by Burgess, was used as part of the standardized operation. Three different postoperative strategies were used.
In the “traditional elastic bandaging” group, subsequent to surgery the amputation stump is covered with a dressing bandage. After a few days the wound is examined by the surgeon. When the wound has healed and the stitches are removed, elastic bandaging is started by the physiotherapist. The elastic bandage is changed every day to be sure of a good pressure gradient from distal to proximal. After stump oedema has been minimised, fitting of a regular prosthesis starts. The procedure from amputation to the delivery of the regular prosthesis usually takes a few months. During this procedure patients start gait training using air splints. Furthermore they are trained to walk without prosthesis with walking devices or bars.
Demographic variables.
In the “immediate fitting method”, the fresh stump is covered immediately after surgery with a minimal wound dressing and wrapped by a rigid plaster cast socket that fixes the knee joint in extension. Once a week the amputation wound is examined by the physician in physical medicine and rehabilitation, the surgeon, the bandagist and the orthopaedic technician. As soon as wound healing starts, a temporary prosthesis with a foot that allows ankle movement in the saggital plane is fixed beneath the cast socket. Commonly, approximately one week after trans-tibial amputation the patient can start reloading his replaced leg under guidance of a physiotherapist. During the weekly wound inspection, the cast socket (and temporary prosthesis) is changed. As soon as the stump oedema has resolved, a regular prosthesis is fitted.
In the “delayed fitting method”, the procedure is similar to the immediate fitting method. However, after surgery the fresh stump is covered with a wound dressing, and the rigid cast socket is supplied only a few days after surgery.
Outcome measures
Stump healing. The duration of stump healing was determined by the number of days between amputation and fitting the regular prosthesis (measurements for the prosthesis can only be taken when oedema has resolved and the wound has healed). The lifetime of the patient's first tube was also registered to control too early fitting.
Local complications. Local complications were categorized into flexion deformity of the knee, superficial wound problems (local infection, superficial bleeding, abrasions), deep wound problems (wound dehiscention, deep infection, deep pressure ulcer) and reamputation (knee disarticulation, trans-femoral amputation or several re-amputations). Only clinically relevant knee flexion deformity from 108 or more were required to have been recorded in the medical files.
General complications. General complications were categorized into four large groups: (1) cardiovascular and/or pulmonary problems, (2) infectious disease, (3) pressure sores, (4) death within 1 year post-amputation. The authors only scored the complications in hospital from amputation to discharge.
Level of independent living. Functional outcome was investigated by scoring the maximum level of independent living reached within 1 year post-surgery. The highest level of independent living is characterized by living alone with or without adaptations. The medium level of functioning is characterised by living with little support, e.g. staying with family or friends or living in a home for elderly people. The lowest level of functioning is characterized by dependent living in a nursing home for a longer period.
Data analysis
The baseline characteristics were compared and also primary outcome measures between early fitting and elastic bandaging and between immediate and delayed fitting. For comparing the immediate and delayed fitting method the authors only investigated differences in velocity of stump healing and the number and kind of local and general complications, because differences in level of functioning were not expected. The data were compared by computing the relative risks and the 95% confidence intervals. Nominal data were tested with student t-test or analysis of variance (ANOVA), ordinal data with Pearson chi-square test. Data were analysed using SPSS Statistical Package for windows 10.0 (SPSS Inc. Headquarters, Chicago, Illinois). A p-value < 0.05 was considered statistically significant.
Results
In the elastic bandaging group 52 patients were included in the study. In the early fitting group 97 patients were included, of whom 57 patients were treated with immediate fitting and 40 patients with delayed fitting. The matching by restriction appeared to be partly successful as the three groups appeared to be rather similar. The only difference was determined by the higher percentage of renal dialysis and renal transplant in the group of immediate fitting as compared to the other two groups (Pearson χ2, p = 0.015). This is explained by the fact that in the hospital using the delayed fitting there are no facilities for renal dialysis. These patients are referred to the hospital with the immediate fitting. There were no other statistically significant differences in either demographic or clinical variables nor differences in premorbid level of functional level (Table I). There were very few missing data (0 to 4 %, see Table I).
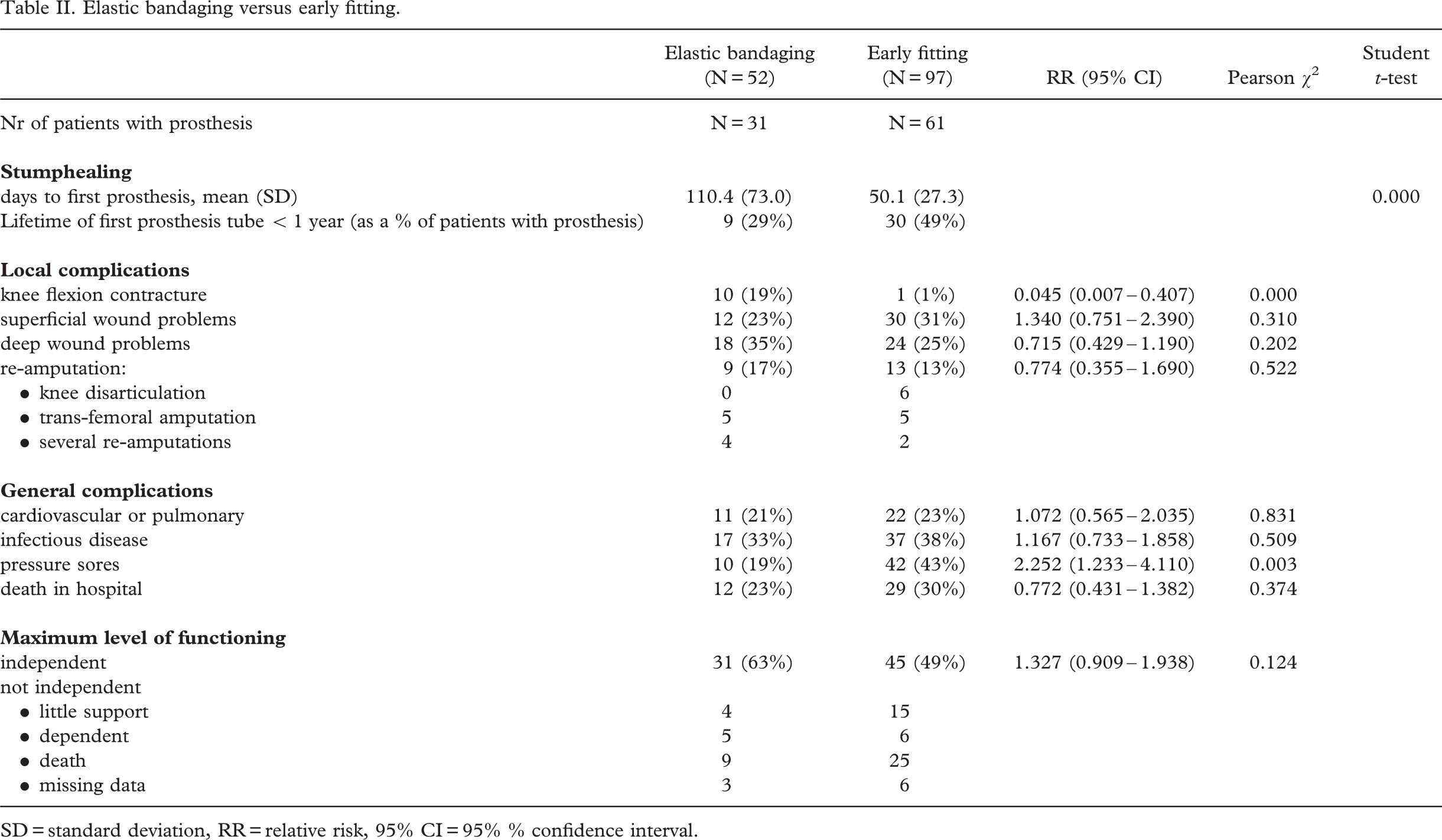
Results of early fitting and elastic bandaging (Table II)
Stump healing. The early fitting group showed a statistically significant (t-test, p < 0.001) shorter mean duration (50.1, days sd 27.3 days) of the time to first prosthesis than the elastic bandaging group (110.4 days, sd 73.0 days). The lifetime of the first prosthesis tube was less than one year for 49% of the early fitting group, against 29% for the elastic bandaging group.
Local complications. The elastic bandaging group (N = 10, 19%) showed statistically significantly (χ2, p < 0.01) more postoperative knee flexion contractures than the early fitting group (N=1, 1%). Moreover the only patient in the early fitting group had a knee flexion deformity prior to surgery. There are no statistically significant differences in the number of wound problems between early fitting and elastic bandaging or differences in rate of reamputations.
General complications. The risk for pressure sores outside the area of the stump (e.g. sacral, trochanters) is increased statistically significantly (χ2, p < 0.02) in the early fitting group (43%) compared to the elastic bandaging group (19%). There were no statistically significant differences in prevalence of cardiovascular, pulmonary problems, infectious problems and hospital death for the two groups. From a post hoc analysis it appeared that the prevalence of pressure sores was not associated with any of the general complications which are assumed to be associated with prolonged immobilization in bed.
Level of independent living. There were no statistically significant differences in maximal functional outcome between the two groups. In both groups approximately 50 to 60% was able to live independently within 1 year and approximately 20 to 25% of the patients died within 1 year after discharge from hospital. The remaining patients were more or less dependent on other caregivers.
Elastic bandaging versus early fitting.
SD = standard deviation, RR = relative risk, 95% C I= 95% % confidence interval.
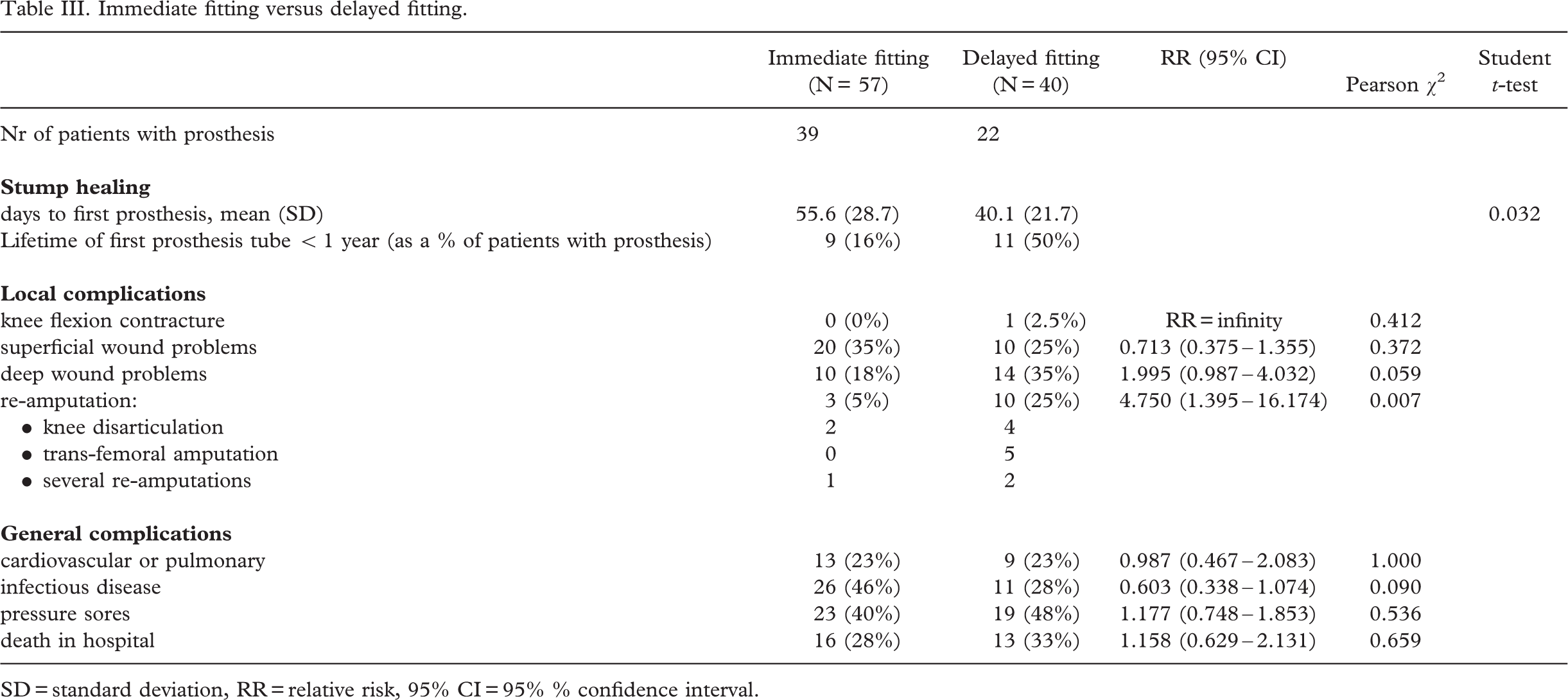
Results of immediate fitting and delayed fitting (Table III)
Stump healing. The delayed fitting group (40.1 days, SD = 21.7) showed a statistically significantly (student t-test, p < 0.05) shorter mean duration of the time to first prosthesis than the immediate fitting group (55.6 days, SD 28.7). In the delayed fitting group a larger part of the patients used their first tube during a longer period of time.
Local complications. In neither immediate nor delayed fitting were there any newly developed knee flexion contractures. The only patient in the delayed fitting group with a knee flexion contracture was already known to have this problem before amputation. Furthermore, there is a statistically significant (χ2, p < 0.026) increased risk for re-amputation in the delayed fitting group, with 25% of the patients (N= 10) needing an amputation at a higher level. From a post hoc analysis it appeared that all 10 patients needing a re-amputation had deep wound problems.
General complications. There are no significant differences in the number of general complications between the immediate and delayed fitted patients.
Discussion
The goal of this study is to investigate the advantages and disadvantages of early fitting with a rigid dressing as a method to improve postoperative care in trans-tibial amputees. Most importantly, in comparison to the traditional elastic bandaging method, the period from amputation to the delivery of a first regular prosthesis can be shortened by half. This indicates that the shaping of the stump is faster and ambulation with a definitive prosthesis can start earlier. In addition, the risk of developing a knee flexion deformity is decreased by the use of early fitting. Moreover, in contrast to the reported disadvantages of early fitting (Cohen et al. 1974), this study did not support the increased risks for local pressure ulcers or other wound problems. In both elastic bandaging and the early fitting method with a delayed application of the plaster cast (the delayed fitting method), risks were comparable (approximately 35%). Using the immediate fitting method this risk was even smaller (18%). One of the assumptions for a faster stump healing time by use of a rigid dressing is the inhibition of development of oedema, promoting an earlier ambulation with prosthesis, whereas the elastic bandaging method allows the oedema to develop. Extending from this assumption, the authors expected a further advantage of early prevention of oedema in the immediate fitting method as compared to the delayed fitting method. However, in contrast to these expectations, the period from amputation to the first definitive prosthesis was shorter in the delayed fitting method. In order to understand this difference a post hoc analysis was carried out in those patients who were actually fitted with a first prosthesis and baseline data and local and general complications during postoperative care compared. The only difference was found in incidence of infections, with the immediate fitting group showing more infections (N=20, of which 13 were due to urinary tract infections) than the delayed fitting group (N = 4). However, this difference was not associated with a difference in time to first prosthesis between patients with (57.1 days, SD 26.8) or without infections (54.1 days, SD 31.3). Although 6 of the 39 patients with immediate fitting were treated by renal dialysis (N = 4), or had already a renal transplant (N = 2) these patients did not show a statistically significant difference in the time to first prosthesis (57.5 days, SD 27.8) as compared to the patients without renal complications (55.3 days, SD 29.3). So it remains unclear which factors are responsible for earlier stump formation and ambulation in the group of patients treated with the delayed fitting method.
Immediate fitting versus delayed fitting.
SD = standard deviation, RR= relative risk, 95% CI=95% % confidence interval.
Unexpectedly, the risk for pressure sores in parts of the body other than the stump is higher in the use of early fitting. Since the findings could not explain this difference by the prevalence of co-morbidity of serious general diseases resulting in immobility, an alternative explanation might be that the mobility during lying in bed is decreased because the heavy plaster cast socket is not removed during bed rest or sleeping.
Another important finding was that the delayed fitting group (who were treated with rigid plaster cast socket within one week postoperatively), showed a higher percentage of reamputations and deep wound problems, This may indicate that when some stump oedema is allowed to develop in the first days following the amputation, the application of the rigid plaster cast creates an increased risk for pressure sores.
The reported advantages of the early fitting method did not result in a better functional outcome within one year after amputation. The authors' impression is that the outcome measure used is a crude measure, not sensitive enough to show differences in functional level.
In comparison to earlier (uncontrolled and descriptive) studies from the 1970s and 80, the quicker healing time of the stump for early fitting with a rigid dressing can be affirmed (Baker et al. 1977; Kraeger 1970; Mooney et al. 1971; Moore et al. 1972) but it could not be confirmed that the risk of wound problems is increased, as reported by Cohen et al. (1974). Two controlled studies used postoperative strategies which were not completely comparable to early fitting, but were also based on the same principles of preventing oedema. Vigier et al. (1999), using a combination of silicon sleeve covered by a plaster cast, demonstrated a quicker wound healing. Wong and Edelstein (2000) using a semi-rigid unna dressing, found a reduction of 50% for the time to the first prosthesis in favour of the semi-rigid dressing when compared with elastic bandaging. In contrast to the results in the present study regarding the functional outcome Wong and Edelstein (2000). found a better functional outcome. This might be explained by the much more sensitive and specific outcome measure they used for functional outcome.
The limitations of this study consist of the retrospective character of the study and the multicentre setting. Although the matching by restriction appeared to be successful there was a possible effect of selection bias because in the hospital employing the delayed fitting method there were no facilities for renal dialysis. However, additional post hoc analyses showed that this difference did not influence the main outcomes of interest.
In conclusion, this study seems to indicate that early fitting after trans-tibial amputation is the treatment of choice in comparison to elastic bandaging. The authors think that the application of a rigid dressing is the key factor to prevent oedema and promote stump maturation and early walking with a temporary prosthesis may have reinforced these results. Although a delay of the application of the plaster cast does not increase, but rather decrease, the time to first prosthesis, the increased risk for deep wound problems and consequently reamputation indicates that this method is not without complications. Therefore, if it is possible to apply a plaster cast immediately in the operating room, the immediate fitting method is preferred. But, the importance of an experienced bandagist and a good collaboration between surgeon, physician in rehabilitation and physical medicine, bandagist, technician and physical therapist must be emphasized.