
Abstract
The treatment effectiveness of the CAD/CAM method and the manual method in managing adolescent idiopathic scoliosis (AIS) was compared. Forty subjects were recruited with twenty subjects for each method. The clinical parameters namely Cobb's angle and apical vertebral rotation were evaluated at the pre-brace and the immediate in-brace visits. The results demonstrated that orthotic treatments rendered by the CAD/CAM method and the conventional manual method were effective in providing initial control of Cobb's angle. Significant decreases (p < 0.05) were found between the pre-brace and immediate in-brace visits for both methods. The mean reductions of Cobb's angle were 12.8° (41.9%) for the CAD/CAM method and 9.8° (32.1%) for the manual method. An initial control of the apical vertebral rotation was not shown in this study. In the comparison between the CAD/CAM method and the manual method, no significant difference was found in the control of Cobb's angle and apical vertebral rotation. The current study demonstrated that the CAD/CAM method can provide similar result in the initial stage of treatment as compared with the manual method.
Introduction
The conventional manual method of making a spinal orthosis is that a negative body cast is taken from the patient with AIS (Wong et al. 2003). A positive cast is then prepared by filling the negative cast with plaster. Rectification of the positive cast is done by removing and adding plaster to certain specific areas of the cast. A spinal orthosis is formed by moulding a plastic sheet onto the rectified positive cast. The required trim line will then be cut and straps will be secured to the orthosis. Adjustments to the orthosis would be done during the final fitting.
Computer-aided design and computer-aided manufacturing (CAD/CAM) systems have been widely used in the industry since the 1970s (Zeid 1991). In 1979, the first CAD/CAM system for P&O was developed by James Foort and his colleagues at the Medical Engineering Resource Unit of the University of British Columbia. The system was for below-knee socket design. Afterwards, other researchers began to develop different parts of the CAD/CAM system with him. The system was demonstrated at the International Society for Prosthetics and Orthotics World Congress in London in 1983. The impact of that demonstration led to a race to develop commercial CAD/CAM systems. There are now close to 10 different CAD/CAM systems in the market such as BioSculptor (Finnieston 1997), CAPOD system (Janols 1997), Clynch Technologies Inc. (Reed 1997), IPOS (Kaphingst 1997), Orten (Genevois 1997), Seattle Limb Systems (Dowell and Poggi 1997), TracerCAD system (Pratt 1997), CANFIT-PLUS™ (Mason 1997) and Prosthetics Design Inc. Most of them can serve not only upper and lower limb prostheses and orthoses but also spinal orthoses. However, research studies about the application of CAD/CAM system to spinal orthotics are very few.
A CAD/CAM system generally consists of 3 units. The first unit is a digitizer which converts the 3-dimensional information of the body or limbs (positive or negative cast) into the data file in digital format. The second unit is the computer station which is used to receive a file, manipulate the image on the screen and allow prosthetists and orthotists to design by inputting data. The third unit is the mill (carver) which receives a rectified file from the computer station and reproduces a 3-dimensional foam/plaster model in which the contour is according to the directives of the rectified file.
The clinical practice of the orthotic treatment for AIS was reviewed by the current research team and some drawbacks were identified in the conventional manufacture of the spinal orthoses such as time consuming cast rectification, high plaster consumption, relatively low accuracy and no data storage for future reference. Apparently, an introduction of a CAD/CAM system in spinal orthotics could benefit not only in time saving but also in standardizing the fabrication process, improving accuracy and allowing prosthetics and orthotics professionals to spend more time on the patient interface such as education, training and counselling. Apart from those technical considerations, the clinical effectiveness of the CAD/CAM method is the major concern. This study aimed to compare the immediate in-brace effectiveness of the spinal orthoses manufactured by the BioSculptor CAD/CAM System and the conventional manual method in the management of adolescent idiopathic scoliosis.
Materials and methods
This prospective study was conducted in the Rehabilitation Engineering Centre of The Hong Kong Polytechnic University (PolyU) and the Department of Prosthetics and Orthotics, Prince of Wales Hospital (PWH). Forty subjects were recruited from the scoliosis clinic of PWH. All were female patients aged 10 to 14 and Risser's sign ≤ 2. Their spines were diagnosed with progressive scoliotic deformity with Cobb's angle between 25°–45° and curve pattern of right thoracic and left lumbar curves, and orthotic treatment was newly prescribed.
The subjects' body shapes were obtained by taking a plaster cast. The spinal orthoses were designed and rectified by the two methods, namely the conventional manual method and the CAD/CAM method. The same orthotist was involved in the whole fabrication process. He had 5 years of clinical experience in treating AIS with spinal orthoses and 3 months' experience of using the CAD/CAM method for making spinal orthoses. The CAD/CAM system used in this research study was the BioSculptor CAD/CAM system located in the CAD/CAM laboratory of the Rehabilitation Engineering Centre, PolyU (Figure 1). This system consisted of an imager (non-contact laser digitizer), computer station with rectification software and 4.5-axis mill.
The subjects' information including name, age, sex, menarche, height, mass, family history and date of clinical visits were recorded. Radiographic measurements on AP and lateral views were taken where the Cobb's angle, curve type, pattern and range, Risser's sign and apical vertebral rotation were obtained. All radiographic measurements were taken by the same prosthetist-orthotist.
The data were analysed using the Statistical Package for Social Sciences (SPSS) Version 10.0. Paired samples t-tests were used to compare the Cobb's angle and apical vertebral rotation at the pre-brace and immediate in-brace visits, and independent t-tests were used to compare the two clinical parameters handled under the two methods. The level of significance was set at 95% (p ≤ 0.05).
Results
Forty female subjects fitted for the set criteria were randomly selected to either the CAD/CAM method or manual method (20 subjects for each method). The mean, standard deviation and range of the subjects' maturity (menarche, age and Risser's sign), body height and mass at the pre-brace visit are shown in Table I.
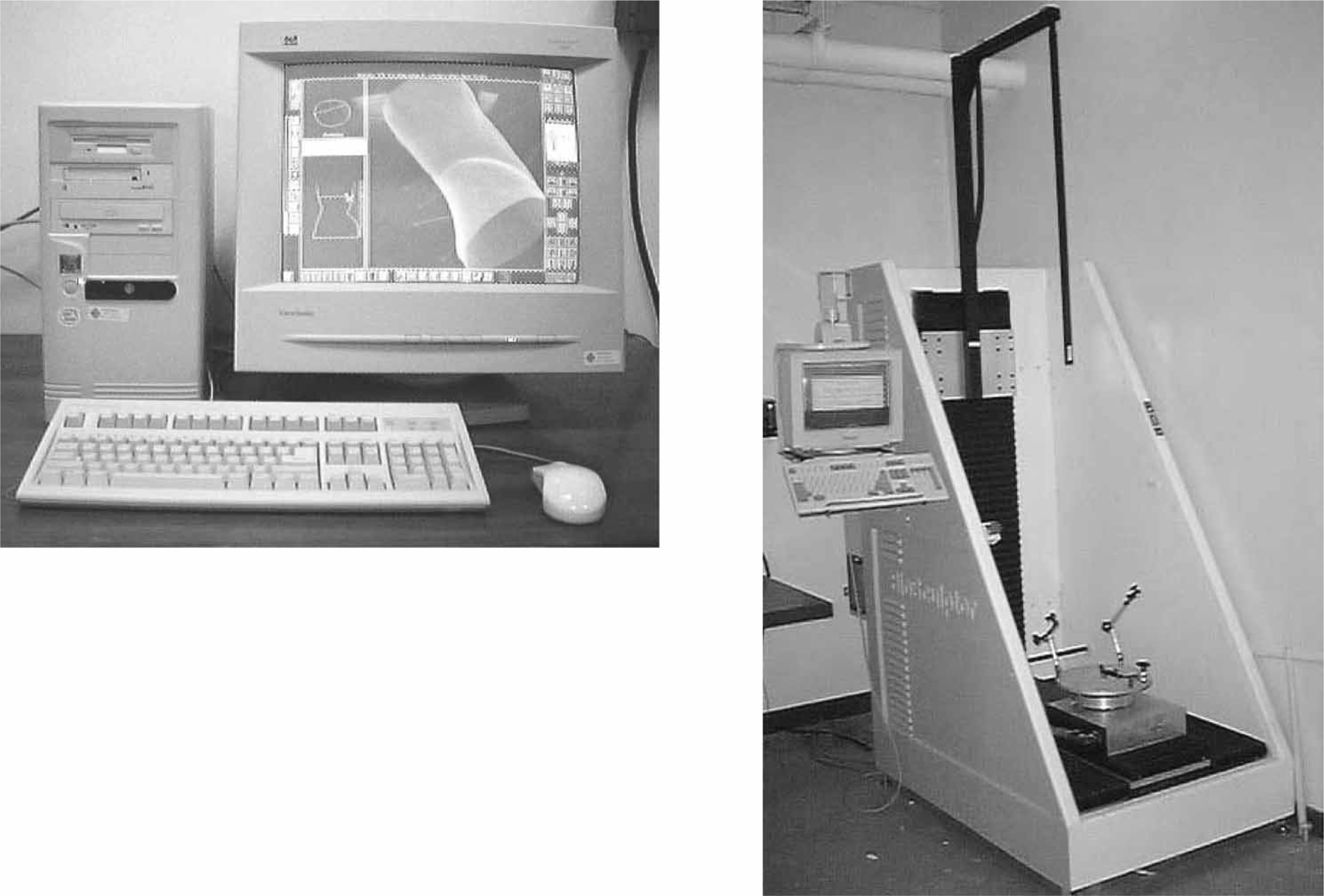
BioSculptor CAD/CAM System: Workstation (left) and Imager (right).
Assessments of the subject's maturity, height and mass.
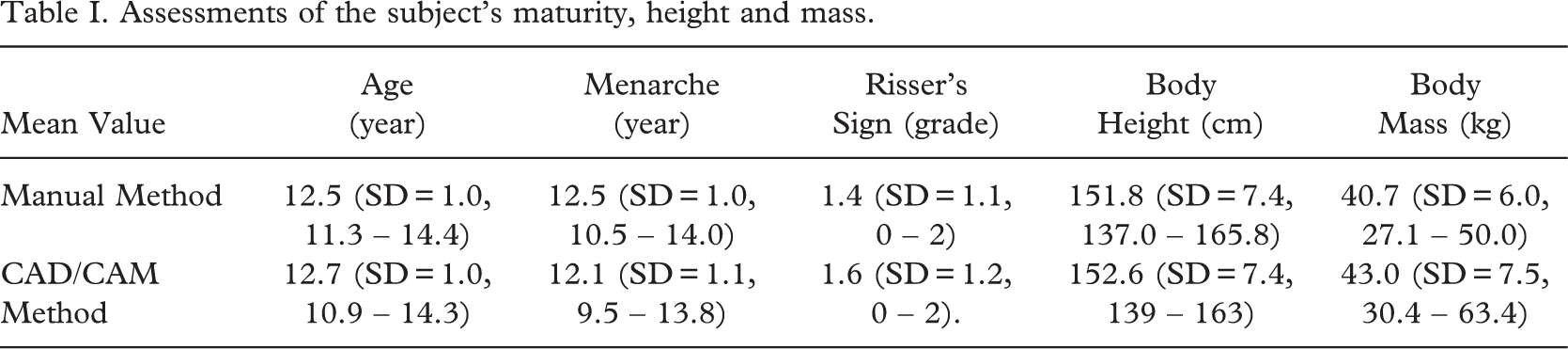
In the manual method, the mean age of the subjects at diagnosis was 12.5 years (SD=1.0, 11.3–14.4) and their mean age of menarche was 12.5 years (SD=1.0, 10.5–14.0). Their mean Risser's sign was 1.4 (SD=1.1, 0–2). The mean body height was 151.8 cm (SD=7.4, 137.0–165.8) and mean body mass was 40.7 kg (SD =6.0, 27.1–50.0). In the CAD/CAM method, the mean age of the subjects at diagnosis was 12.7 years (SD=1.0, 10.9–14.3) and their mean age of menarche was 12.1 years (SD=1.1, 9.5–13.8). Their mean Risser's sign was 1.6 (SD=1.2, 0–2). The mean body height was 152.6 cm (SD=7.4, 139–163) and mean body mass was 43 kg (SD=7.5, 30.4–63.4).
The distribution of the curve pattern is shown in Table II. The curve pattern for those two subject groups is homogeneous.
Cobb's angle
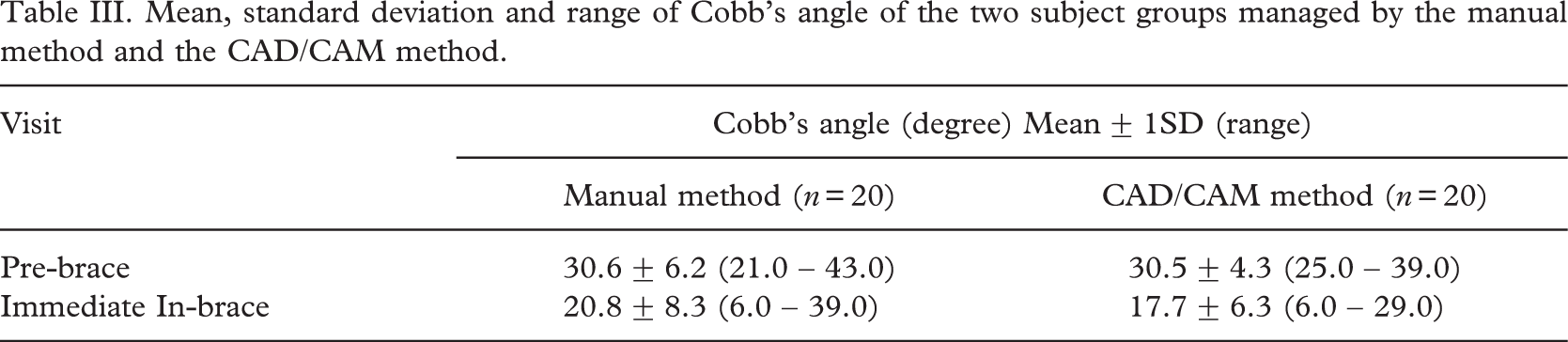
The mean, standard deviation and range of Cobb's angle of the two subject groups managed by the manual method and the CAD/CAM method respectively are shown in Table III and Figure 2.
Both methods showed significant decrease (p < 0.05) in the Cobb's angle after the orthotic treatment was applied. In the manual method, the mean Cobb's angle reduced from 30.6° (SD = 6.2, 21.0–43.0) at pre-brace visit to 20.88 (SD =8.3, 6.0–39.0) at immediate in-brace visit while in the CAD/CAM method, the Cobb's angle changed from 30.5° (SD=4.3, 25.0–39.0) to 17.7° (SD = 6.3, 6.0–29.0).
Apical vertebral rotation
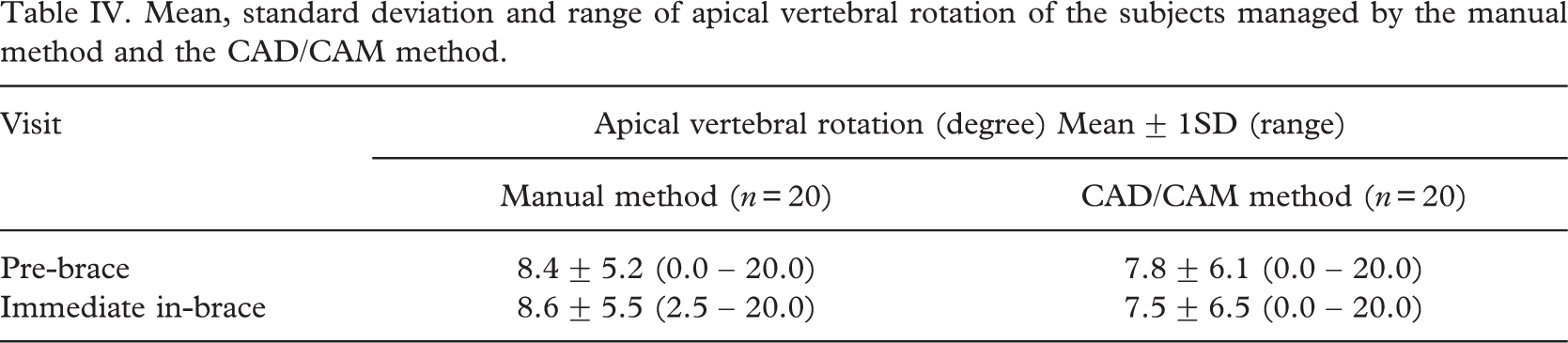
The mean, standard deviation and range of apical vertebral rotation of the two subject groups managed by the manual method and the CAD/CAM method respectively are shown in Table IV and Figure 3.
Regarding the apical vertebral rotation, there was no significant change (p > 0.05) between methods. In the CAD/CAM method, the apical vertebral rotation decreased from 7.8° (SD=6.1, 0.0–20.0) at pre-brace to 7.5° (SD=6.5, 0.0–20.0) at immediate in-brace but there was an increase from 8.4° (SD =5.2, 0.0–20.0) at pre-brace to 8.6° (SD=5.5, 2.5–20.0) at immediate in-brace for the manual method.
Comparison of the manual method and the CAD/CAM method
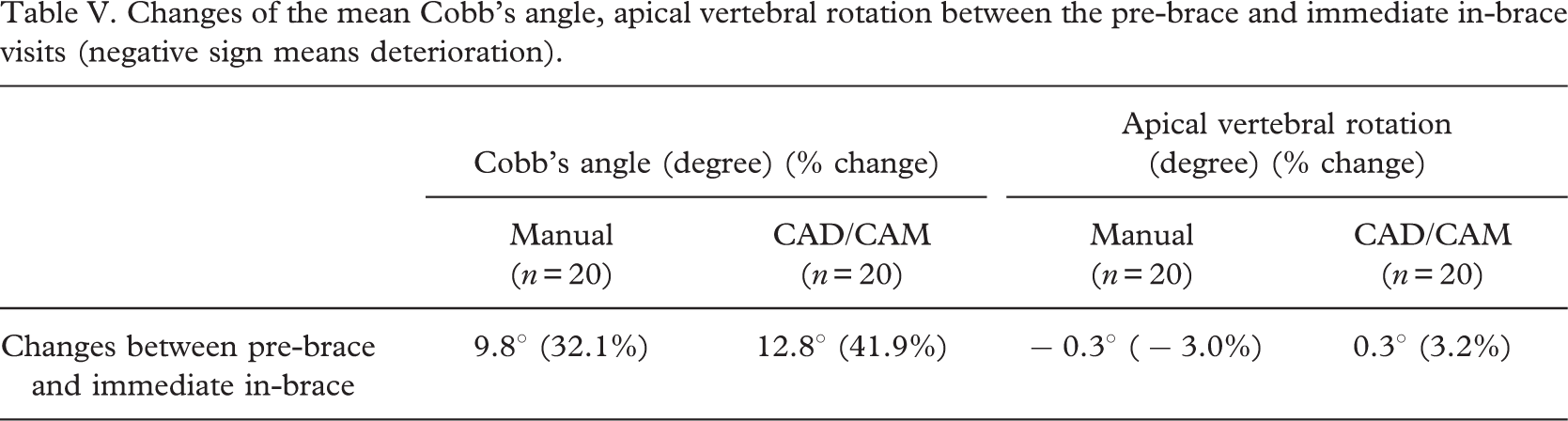
The changes of the mean value of the Cobb's angle and apical vertebral rotation between the pre-brace visit and the immediate in-brace visit are shown in Table V.
In the comparison of changes of Cobb's angle between the pre-brace and immediate in-brace value for the manual method and the CAD/CAM method, there was no significant difference (p = 0.117). Similarly, in the comparison of changes of apical vertebral rotation between the pre-brace and immediate in-brace value for the manual method and the CAD/CAM method, there was no significant difference (p = 0.643).
Curve pattern distribution.

Mean, standard deviation and range of Cobb's angle of the two subject groups managed by the manual method and the CAD/CAM method.
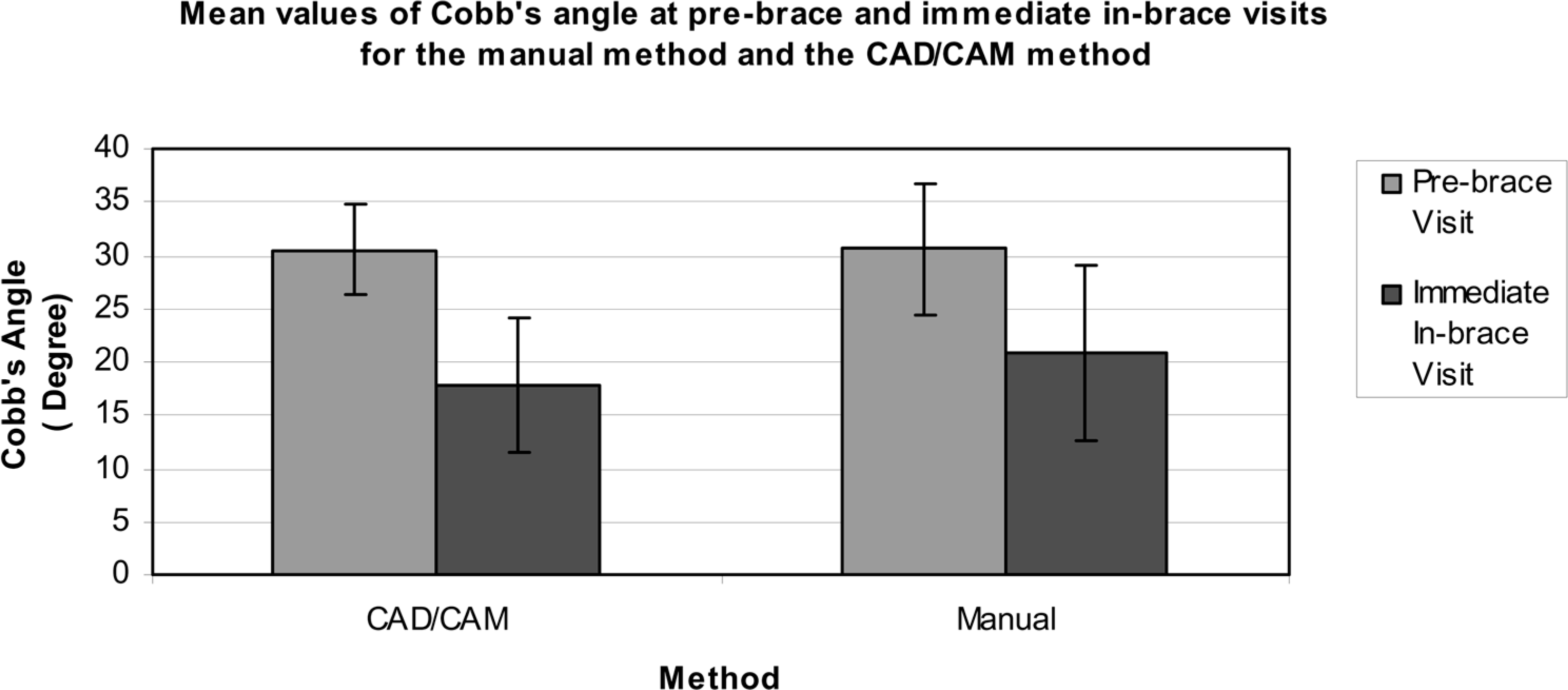
Mean values of Cobb's angle at pre-brace and immediate in-brace visits for the manual method and the CAD/CAM method.
Mean, standard deviation and range of apical vertebral rotation of the subjects managed by the manual method and the CAD/CAM method.
Discussion
The results of the current study showed that orthotic treatment rendered by the manual method and CAD/CAM method can provide significant initial control in the Cobb's angle of patients with adolescent idiopathic scoliosis. For the CAD/CAM method, the mean reduction value of Cobb's angle at immediate in-brace visit was 12.88 while the manual method had a decrease of 9.8°. These values were less than the results of some previous studies. In Eman et al.'s (1986) study of 295 patients, an initial reduction of 14.5° was found. Wiley et al. (2000) reported a decrease of 19°. Different orthosis designs may have different responses to the initial control and even the final result of treatment. In addition, different casting methods used may also affect the control of Cobb's angle (Wong et al. 2003).
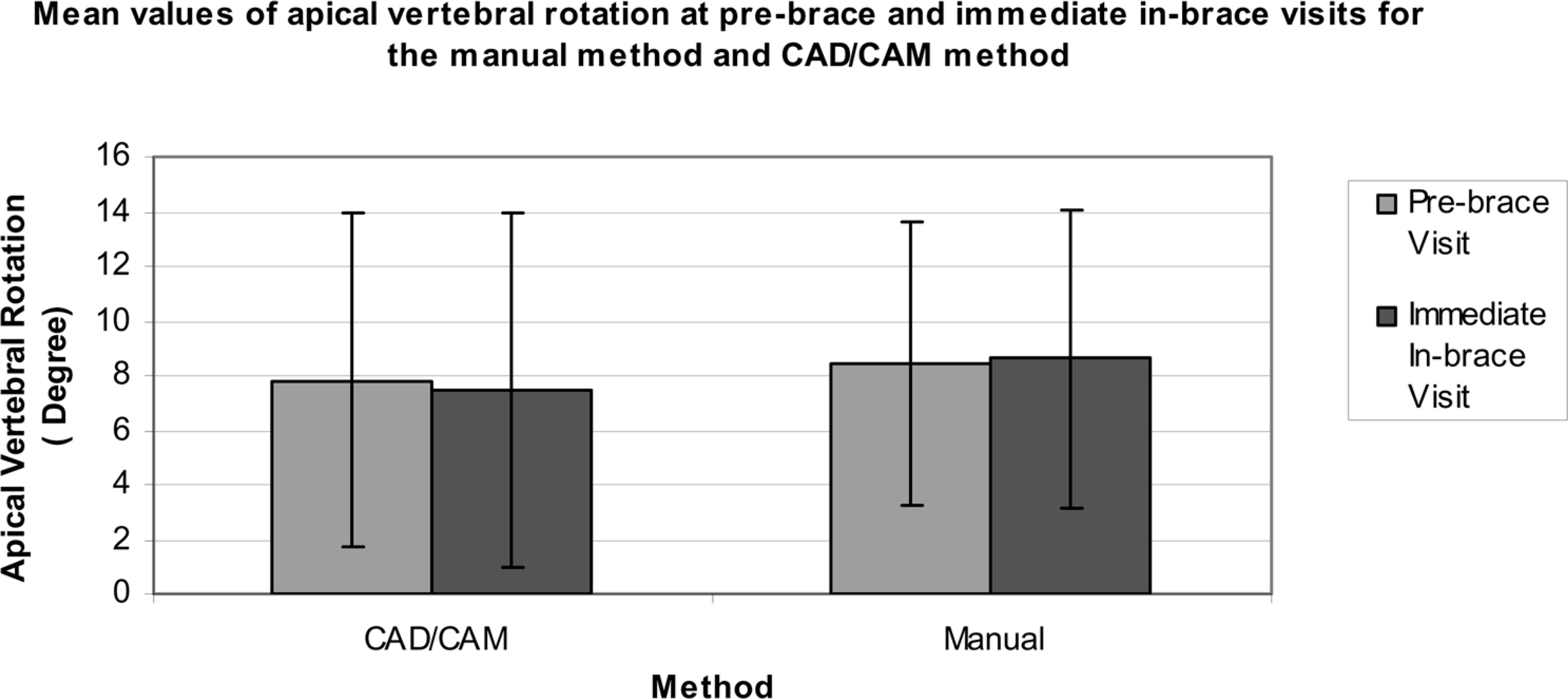
Mean values of apical vertebral rotation at pre-brace and immediate in-brace visits for the manual method and the CAD/CAM method.
Changes of the mean Cobb's angle, apical vertebral rotation between the pre-brace and immediate in-brace visits (negative sign means deterioration).
In the current study, neither the CAD/CAM method nor the manual method could provide an initial control of the apical vertebral rotation. For the CAD/CAM method, the mean reduction of apical vertebral rotation at the immediate in-brace visit was 0.3° (3.2%) while for the manual method, the mean value was even increased/deteriorated by 0.38 (3.0%) at immediate in-brace stage. This result was less than the findings of some previous studies. The mean reduction value of apical vertebral rotation recorded in Wong et al.'s (2003) study was 3.9° (21.4%) for frame casting and 3.8° (25.3%) for supine with traction. Aaro et al. (1981) found a decrease of 35% at immediate in-brace visit. One of the possible reasons for this obvious control being not shown in the current study may be the relatively low pre-brace value–the mean pre-brace apical vertebral rotation was 8.4° for the manual method and 7.8° for the CAD/CAM method. Those values were relatively mild compared to 18.28 for the frame casting method and 15.08 for the supine with traction method in Wong et al.'s (2003) study.
In the comparison of changes of Cobb's angle and apical vertebral rotation between the pre-brace and immediate in-brace value for the manual method and the CAD/CAM method, there was no significant difference. In addition, from the result of the mean reduction value of Cobb's angle and apical vertebral rotation in the current study, it was noted that the orthotic treatment based on the CAD/CAM method could have a slightly better initial in-brace control than that of the manual method. Apparently, the CAD/CAM method can be considered as a competitive choice of manufacturing method for handling adolescent idiopathic scoliosis.
Conclusion
In the current study, the spinal orthoses manufactured using the CAD/CAM method and the manual method could both demonstrate an effective initial control of the Cobb's angle of the patient with adolescent idiopathic scoliosis. However, no significant reduction of the apical vertebral rotation was shown in either method. By comparing the mean reduction value of the Cobb's angle and apical vertebral rotation between the two methods, no significant difference was found. Thus, the CAD/CAM system could provide similar treatment results to the manual method. This would be one of the references for the professionals who want to choose the CAD/CAM system to manage adolescent idiopathic scoliosis. To understand the efficacy of the CAD/CAM system comprehensively, a prospective and long-term evaluation is advocated.