
Abstract
This case report presents a 51 year old female patient who had a train accident in 1999. She suffered bilateral trans-tibial and bilateral trans-radial amputations. In this paper, the evolution of the right transradial amputation where eventually a Krukenberg procedure was performed, is described as is its good functional outcome after rehabilitation treatment. After this first procedure the patient also asked for the Krukenberg procedure for her left arm.
Introduction
In 1917 Hermann Krukenberg, a German army surgeon developed a procedure for phalangising the forearm. In this operation, the radius and ulna are separated, thus creating a pincer-like grasp that gives the patient good pinch and grip with useful sensibility (Krukenberg 1917, 1931). With this concept he conceived a grip function with preserved sensitivity, which no prosthetic device could provide. The main drawback is the poor cosmesis of the stump because of the crab-like pincers. This procedure is frequently rejected in the Latin American continent where culture gives priority to cosmesis above function; however, in other countries an additional prosthesis can contribute to cosmesis (Matussek and Neff 2003).
The standard indication for the Krukenberg procedure is on blind bilateral trans-radial amputees (Irmay et al. 2000). In this case report, however, the patient is not blind, as was already also indicated and described in several patients by Garst (1991), Marquardt and Martini (1985) and Irmay et al. (2000).
Case report
A 51-year-old female suffered a train accident four years ago, resulting in amputation of the four limbs, bilateral trans-tibial short amputations and bilateral trans-radial amputations. The right trans-radial amputation was at the distal third of the forearm, and the left one at the union of the proximal third with the middle third. She has a supportive husband and daughter and she used to do all the domestic work in the household.
She was fitted with PTB prostheses for her both legs. However, this report will only deal with the upper limbs. The residual upper limbs were fitted with functional-mechanical prostheses with active opening and passive closure mechanical hands, cosmetic gloves and Hosmer 5Xa hooks, with a suspension to the opposite shoulder. She was trained in the use of these prostheses with a good functional result. Nevertheless, she abandoned their use and preferred to use the bare stumps, with both forearms acting as pincers, and according to the patient she feels more comfortable because she “can touch and feel”. For this reason the advantages and disadvantages of the Krukenberg amputation were shown and explained, in order to transform her right stump into an active pincer. The patient was shown other documented cases and eventually accepted the procedure. The right stump was chosen to be operated on in the first instance because it was considered to have an adequate length, while the left one was too short and the distal part barely exceeded the distal insertion of the pronator teres. She was operated on in 2002.
Surgery
The stump was hypertrophic because of the time elapsed since the amputation, with significant atrophy of the muscles and with a reduction of the cutaneous cover. The palmar and dorsal flaps were fashioned without separating the skin from the aponeurotic layer so that no compromise of irrigation and innervation occurred. The brachio radialis, the flexor carpis radialis and the extensor carpis radialis longus were reinserted on the external palmar and dorsal face of the radius respectively. The other tendons were used to cover and pad the ulnar and radial ends, which were severed at the same length. The interosseous membrane was released, achieving an unforced separation of approximately 8cm. The medial, radial and ulnar nerves were cut short in order to protect their ends from the pressure zones. Radial and ulnar arteries were ligated distally. Skin closure on the ulnar portion left an uncovered muscular area, which was not covered with skin grafts, as many authors describe (Irmay et al. 2000; Gu et al. 1996), because it was considered that they attach to the surface of the area. The use of tissue expanders to gain sensitive skin is already described in literature (Stober and Traub 1998). Spontaneous closure allows its progressive reduction due to the normal scarring retraction. General anaesthesia was preferred and an haemostatic tourniquet was used. The tourniquet was released after the muscular momentum was finished and homeostasis was secured. It is crucial to avoid haematomas that can jeopardize the vitality of the flaps. Resorbable sutures were used in deep layers, while nylon was used on superficial layers. Soft dressing was placed, to keep it in position, for 3 weeks. The non-covered surface was taken care of on an everyday basis, and total closure occurred 40 days after the surgery. The scar did not interfere at all in the posterior rehabilitation.
Rehabilitation
The main objectives for the patient were to gain self-sufficiency and a strong and functional grip. The patient received active assisted mobilization in order to train in opening and closure movements of the Krukenberg pincers. Oedema and scar tissue were treated according to conventional techniques. The most important feature was to stimulate a wide and strong grip between the ulna and the radius. In order to enhance the opening and closure the best position to train the patient was in: abduction, supine forearm, elbow in flexion and/or adduction, prone forearm, elbow in flexion. Once the patient has learned these movements, objects were incorporated to train grasping and releasing. These elements were graduated in size and shape, utilizing always at the beginning small, compact, rigid and light objects. The difficulty is in gaining the ability to hold the object without releasing it because the patient tends to open the stump ends naturally by moving the bones as if they were normal fingers. The patient was very anxious to obtain immediate results so the occupational therapist had to control the time for activity to avoid tiredness and lack of attention. This anxiety to achieve quickly activities of daily life (ADL) can sometimes play a negative role. Opening range and muscle strength gradually improve with the treatment. It is important to try to avoid scar adherences. Sensitivity is simultaneously stimulated, bearing in mind that sensitive innervation is less on the forearm than on the hand. The patient is trained to recognize the grasping and releasing of objects, as well as their size, texture, temperature, pressure, weight, and consistency. Stereognosis is hard to achieve in the first years, and as this patient can see, she uses eyesight to compensate.
During the first year of training muscle strength increased, until she was able to lift 10kg with the elbow flexed in a prone position. After the first year grip could be achieved in a pronated, supined and neutral position, with an extended elbow and assisted by gravity (arm at the side of the body). Training was provided in activities of daily living (ADL) and independence was achieved with functional assistance, substitute grasping and some adaptations.
At different stages of the training measurements were done with Jamar, pinch and picking-up tests, as well as with ADL scales for feeding, personal hygiene, dressing, hand and computer writing, and all activities concerning the house tasks. Donning and doffing her PTBs were better than with her conventional prostheses (Figure 1).
These assessments were done every month to measure improvements in independence.
Discussion
This is an adult female patient, who requires maximum function to manage all the activities of housekeeping while her husband works. Initially after traumatic bilateral forearm amputation she was provided with mechanical prostheses. Eventually she stopped using them because she chose to use her bare stumps as pincers. She explained that being able to feel helped her a lot in her tasks. Due to her desire of preserving sensitivity, a Krukenberg procedure was performed on her right stump. There has been a lot of controversy regarding this procedure for cosmetic reasons (Krukenberg pincher; Figure 2) when proposed to other patients and many surgeons have refused to perform it (Loosli-Guinard et al. 1983). She accepted the proposal, in spite of the cosmetic appearance. Yet, an excellent functional result was obtained, from both the surgical and the rehabilitation point of view. The patient lives with her family, takes care of the household, and does art and crafts, which she is currently selling, and is very happy with the procedure. A year and a half has gone by and she is still gaining dexterity and strength.
Conclusion
The Krukenberg procedure is an option to achieve manual dexterity in double forearm/hand amputees where resources for sophisticated prostheses are lacking and where the Krukenberg improves function beyond every existing prosthetic system.

Donning the prosthesis.

Krukenberg pincher.
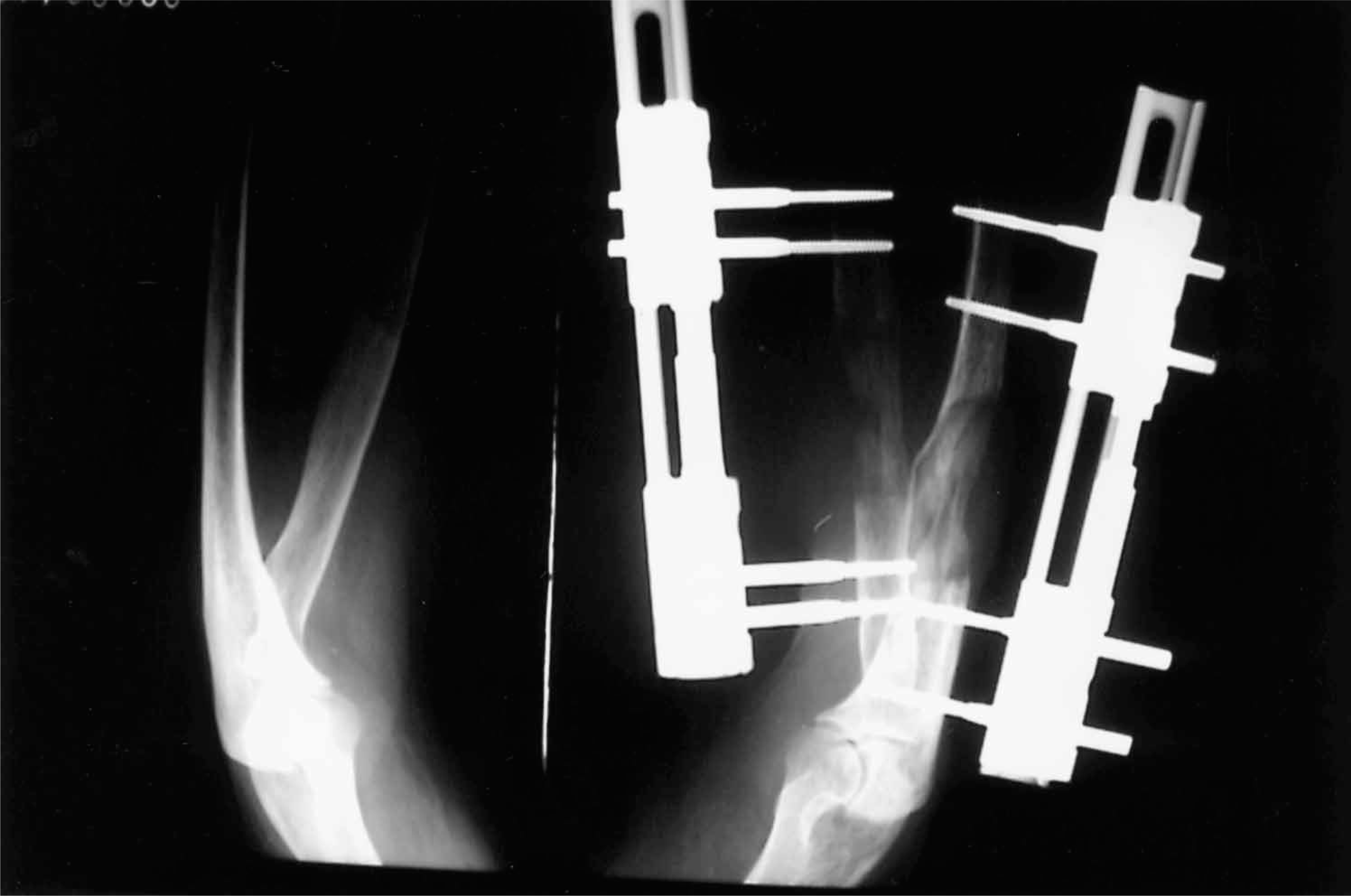
Elongation technique.
Postscript
The patient was so well adapted with her right limb Krukenberg, that months later she asked for the same procedure on her left limb, where she was using a prosthesis. She said that sensitivity made all the difference and she did not want to go on using the prosthesis. The left stump was very short for such a procedure. The first option considered was to reinsert the teres pronator proximally but the conclusion was that the opening of the pincer would be poor. The favoured option was the lengthening of the forearm bones. Two uniplanar external fixators were placed one at the ulna and one at the radius, to avoid blocking pro- and supination movement during the elongation period (Figure 3). Ninety days have gone by since the surgery, and though the whole process has not ended, the bones have elongated 5cm (26%). As soon as the callous is consolidated the fixators will be removed and the training will begin again.
In literature the precise indication for this procedure is in blind trans-radial bilateral patients, but the authors believe that it should have a wider indication. It has the advantages of keeping sensitivity and the precision that can be obtained in the pincer, both allowing for an excellent function without the need of a prosthesis; especially in those cases where it is difficult or expensive to obtain one, for social or economical reasons.