
Abstract
In order to achieve stump healing after trans-tibial amputation, various methods are applied, such as soft dressings followed by elastic wrapping of the stump, rigid dressings, semi-rigid dressings, and more recently the application of silicon or gel-liners. A systematic literature search was performed to identify the optimal post-amputation management. The methodological quality of the studies was systematically evaluated by using a predefined list of criteria. Only 11 controlled studies were identified and evaluated for their methodological quality. From these studies, no studies were classified as A-level studies, whereas three were classified as B-level, and 8 were classified as C-level studies. Relevant literature appears heterogeneous with respect to patient selection, intervention and outcome measures. Despite the large variability of included studies, this review reveals a trend in favour of rigid and semi-rigid dressings for achieving stump healing and reduction of stump volume. No conclusions can be drawn with regard to the effect on functional outcome. The literature is not conclusive on the effects of early weight bearing on stump healing, volume reduction, and functional outcome. More research is needed for the development of evidence-based clinical practice guidelines concerning management after trans-tibial amputation.
Introduction
In post-amputation management, achieving optimal stump healing is one of the primary objectives. Although this objective appears obvious, there is no consensus on how to use wound dressings to optimise healing after trans-tibial amputation.
Various methods have been applied to achieve stump healing. Since the 1960s, there has been an increasing interest in improving post-operative management, precipitated by the post-surgical care based on the immediate fitting principle (Tooms 1998). Burgess and colleagues improved the technique of the immediate post-surgical plaster fitting (Berlemont 1969), and their technique was adopted by many contemporary surgeons (Condon and Paul 1969; Golbranson et al. 1968; Moore et al. 1968; Vitali and Redhead 1967; Warren and Moseley 1968). Today, soft dressings with subsequent elastic wrapping of the amputation stump remains the post-surgical technique of choice (Choudhury et al. 2001). In addition to elastic wrapping of the stump and the immediate plaster-fitting technique, various methods and modifications of post-surgical management have been developed. These methods include semi-rigid dressings (SRD) such as unna paste and polyethylene (Ghiulamila 1972; Sterescu 1974; Swanson 1993), and pneumatic aids that can be recycled (Kernstein 1974; Little 1971; Redhead et al. 1978; Scott et al. 2000; Sher 1974; Sher and Liebman 1982).
The application of a plaster cast immediately after trans-tibial amputation was considered to serve two main functions: oedema reduction on the one hand and early weight bearing and ambulation using a simple pylon prosthesis on the other hand (Kay, 1975). Burgess and Romano (1965) consider oedema to be a pathological accumulation and retention of intracellular and extracellular fluid in response to trauma and a main factor in prolonged amputee rehabilitation (Golbranson et al. 1968). It is believed that in the absence of oedema, a maximum of capillary blood supply is available for the healing process of tissues, therefore improving wound healing. In addition to this, Moore et al. (1968) stated that subjecting a stump to gravity increases perfusion within the healing tissues. The additional effect of ambulation on the reduction of oedema is described by Gerhardt et al. (1970). They believe that this mechanism is partly based on an increased counter-pressure within the socket during weight bearing but also, more importantly, the result of the pumping action of the stump muscles, which directs venous blood centrally. With this in mind, the immediate plaster-fitting technique and other techniques of local stump management were combined with early mobilization in order to improve wound healing (Ghiulamila, 1972; Little, 1971; Redhead et al. 1978; Sher and Liebman 1982; Sterescu 1974). Bipedal standing with graded (minimal to full) weight bearing and walking were permitted at different stages after surgery. Condon and Paul (1969) encouraged full weight bearing immediately after surgery, while Warren and Moseley (1968) only allowed full weight bearing after inspection at about 7–10 days after surgery.
The diversity of treatment procedures after trans-tibial amputation and the lack of consensus constituted the impetus for conducting this systematic literature review. The purpose of this review was to establish the optimal post-amputation management taking into consideration wound healing, oedema reduction and functional outcome.
Methods
Literature search
Material for the review was collected from a systematic search in Medline (from 1970), Current Contents (from 1996), and the Cochrane Database (2003 Issue) until May 2003. A combination of the following keywords and their synonyms was used: ‘amputation', ‘trans-tibial', ‘amputation stump', ‘immediate/early/delayed/prosthetic fitting', ‘soft/plaster/semi rigid dressing', ‘airsplint', ‘PPAM', ‘post-amputation-management', ‘early ambulation', ‘amputation rehabilitation', ‘stump healing', ‘oedema reduction', ‘randomized-controlled trial', ‘comparative', ‘case-control', and ‘experiment'. The studies were selected by assessing the information provided within the abstracts if available. If this information was inadequate, the full article was perused for relevant data. In addition, references from the retrieved articles were reviewed.
Selection criteria
Based on the information derived from the abstracts, studies were selected if they met the following four criteria:
Studies that pertained to post-surgical stump dressings or the use of temporary prostheses in trans-tibial amputees.
Studies in which wound healing after amputation, oedema control or mobilization were the outcome measures.
Studies with either a Randomized Controlled Trial (RCT) design or a case-control design.
Publication in the English, German, French, or Dutch language.
Assessment of methodological quality
The methodological quality of the selected studies was assessed independently by two reviewers (SEN, HvdL). In case of disagreement, consensus was reached by discussion. Thirteen modified criteria (Figure 1 and Appendix A) were used for the evaluation of the included studies in terms of selection of patients, intervention, outcome measurement and statistics (Tulder et al. 1997). Each criterion was scored dichotomously: ‘1' for yes, ‘0' for no or unsure. The criterion ‘blinding of the patient' was excluded of the original criteria list because this was found to be irrelevant in relation to the outcome measure of interest.
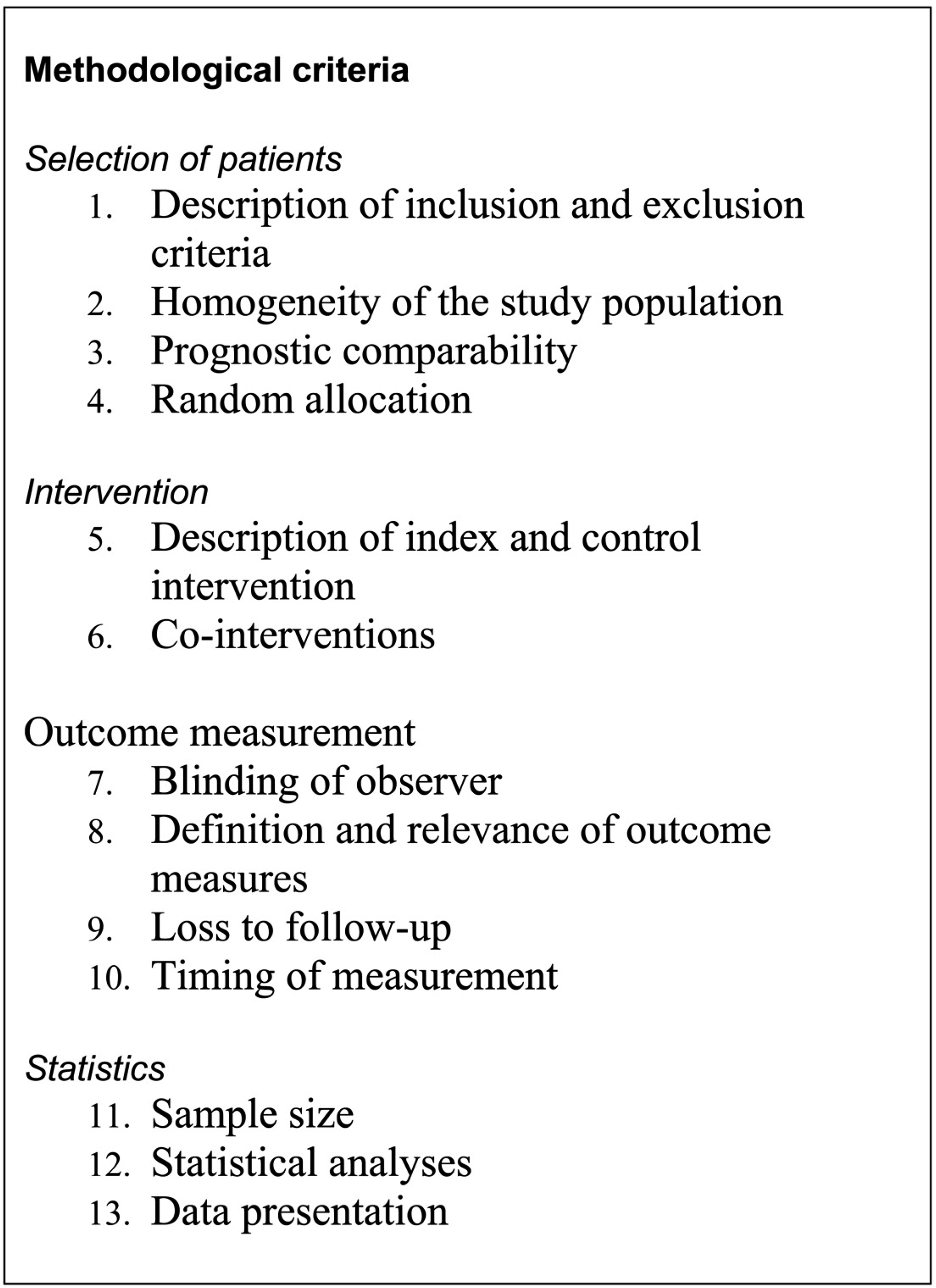
Modified criteria to assess the studies.
Methodological evaluation and grading of included studies.
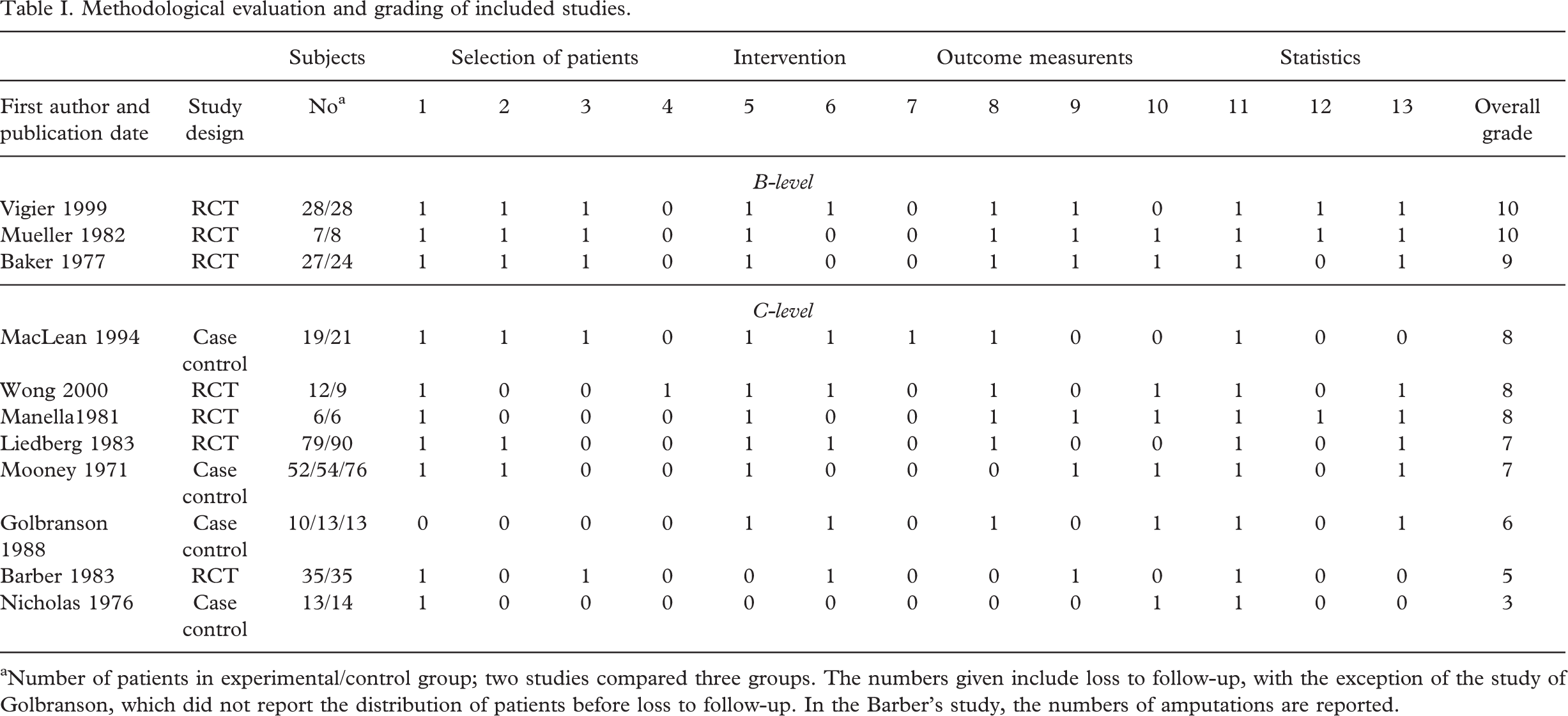
Number of patients in experimental/control group; two studies compared three groups. The numbers given include loss to follow-up, with the exception of the study of Golbranson, which did not report the distribution of patients before loss to follow-up. In the Barber's study, the numbers of amputations are reported.
Data extraction and data analysis
The authors chose to perform a qualitative review, since the existing literature on post-surgical management is too heterogeneous with respect to the performed methods, statistics as well as the lack of highly qualified studies. Therefore, in addition to RCTs, case control studies also were selected. In order to perform a best evidence synthesis, the methodological strength of each study was assessed. Studies were classified at A-level when the total score of all criteria amounted to 11 points or more, in addition to a positive score for functional homogeneity (criterion 2) and prognostic comparability (criterion 3). Studies were classified at B-level if the score totaled 9 or 10 points also in addition to a positive score for criterion 2 and 3. Studies were classified at C-level in the event the total score was less than 9 points or when these studies presented with a negative score for criterion 2 or criterion 3.
Results
Selection of literature
The systematic search yielded in the identification of 439 studies. Sixteen controlled studies were identified, from which five studies (Kane and Pollak 1980; Pinzur et al. 1988; Moore et al. 1972; Schon et al. 2002; Wu et al. 1979) with historical control groups were excluded. Only 11 studies were found to meet our criteria for selection.
Methodological quality
Table I shows the evaluation of the selected studies based on the sum scores of methodological criteria. According to the applied methodological criteria, only three studies could be classified as B-level studies, whereas eight studies received a C-level classification. In one study, a valid randomization of treatment allocation (criterion 4) was applied and documented, and in another study, the observer was blinded to the intervention (criterion 7). In three studies, statistical analysis was carried out and reported adequately (criterion 12).
Study results
Descriptive data, reported study results, and outcome measures of the selected studies are presented in Table II. Four relevant outcome measures were identified within the selected studies and will be discussed below.
Stump healing
Healing of the stump constituted a main outcome measure in two B-level studies (Baker et al. 1977; Vigier et al. 1999) and four C-level studies (Barber et al. 1983; Liedberg et al. 1983; Mooney et al. 1971; Nicholas and Demuth 1976). Vigier et al. (1999) found a shortening of healing time using a plaster cast interposed with a silicon liner up to 5 h a day when compared to elastic compression bandages (71.2 ± 31.7 versus 96.8 ± 54.9 days, P = 0.04). The B-level study of Baker et al. (1977), however, did not show a difference in wound healing rates when comparing a soft dressing with a rigid dressing. Two C-level studies (Mooney et al. 1971; Nicholas and Demuth 1976) support the result of the study of Vigier et al. (1999) who reported higher healing rates (primary-/secondary-/non-healing) when using rigid dressings. One C-level study (Barber et al. 1983) showed similar results to those of the study of Baker et al. (1977). No studies found any negative wound healing effects as a result of the application of rigid dressings. The study of Liedberg et al. (1983) assessed possible deleterious effects from the use of a temporary prosthesis, called the Tulip prosthesis. They found no differences in wound healing; primary healing occurred in 25 out of 47 patients in the Tulip group and in 21 out of 48 patients in the control group.
Characteristics of included B and C studies.
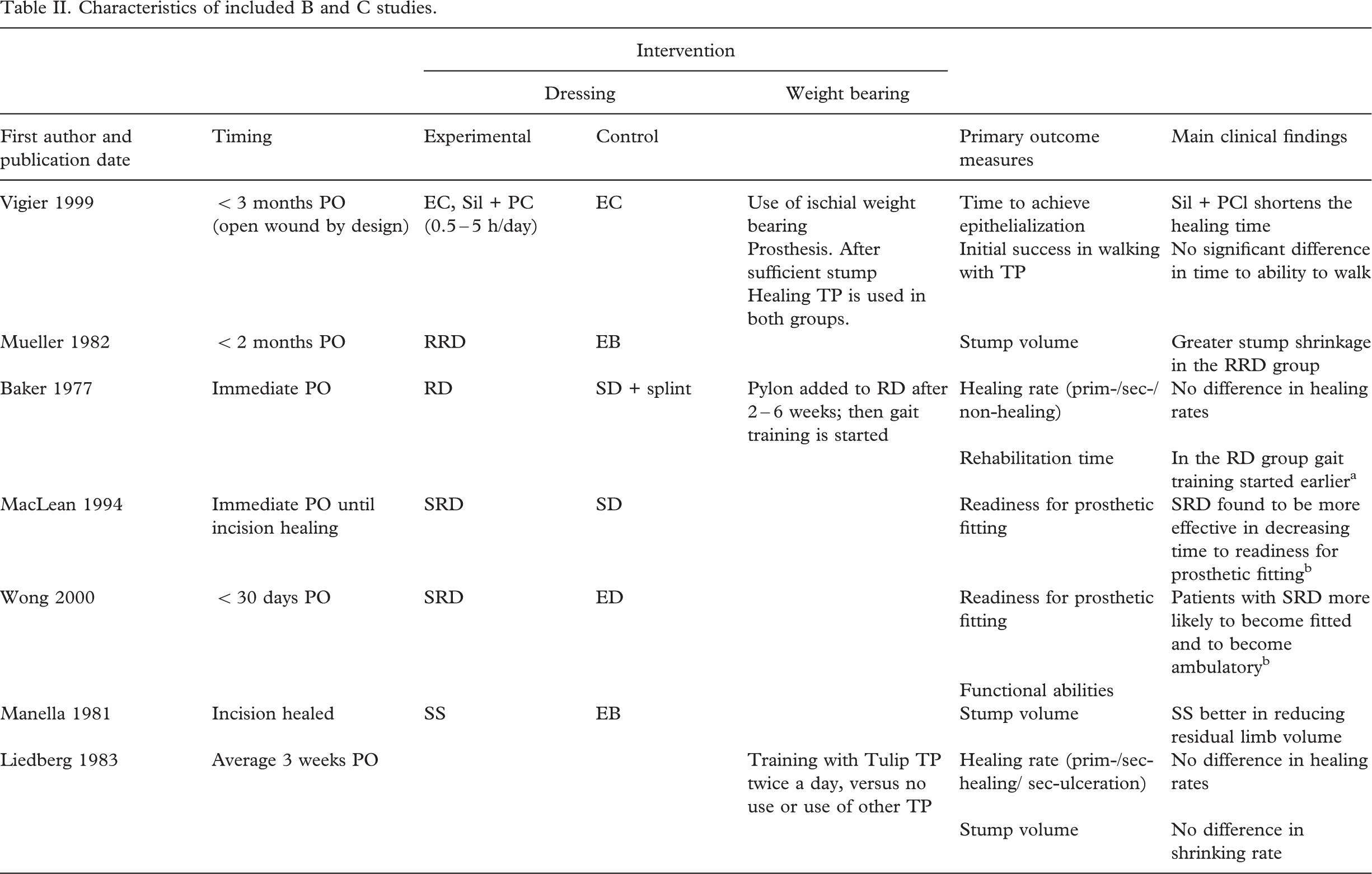
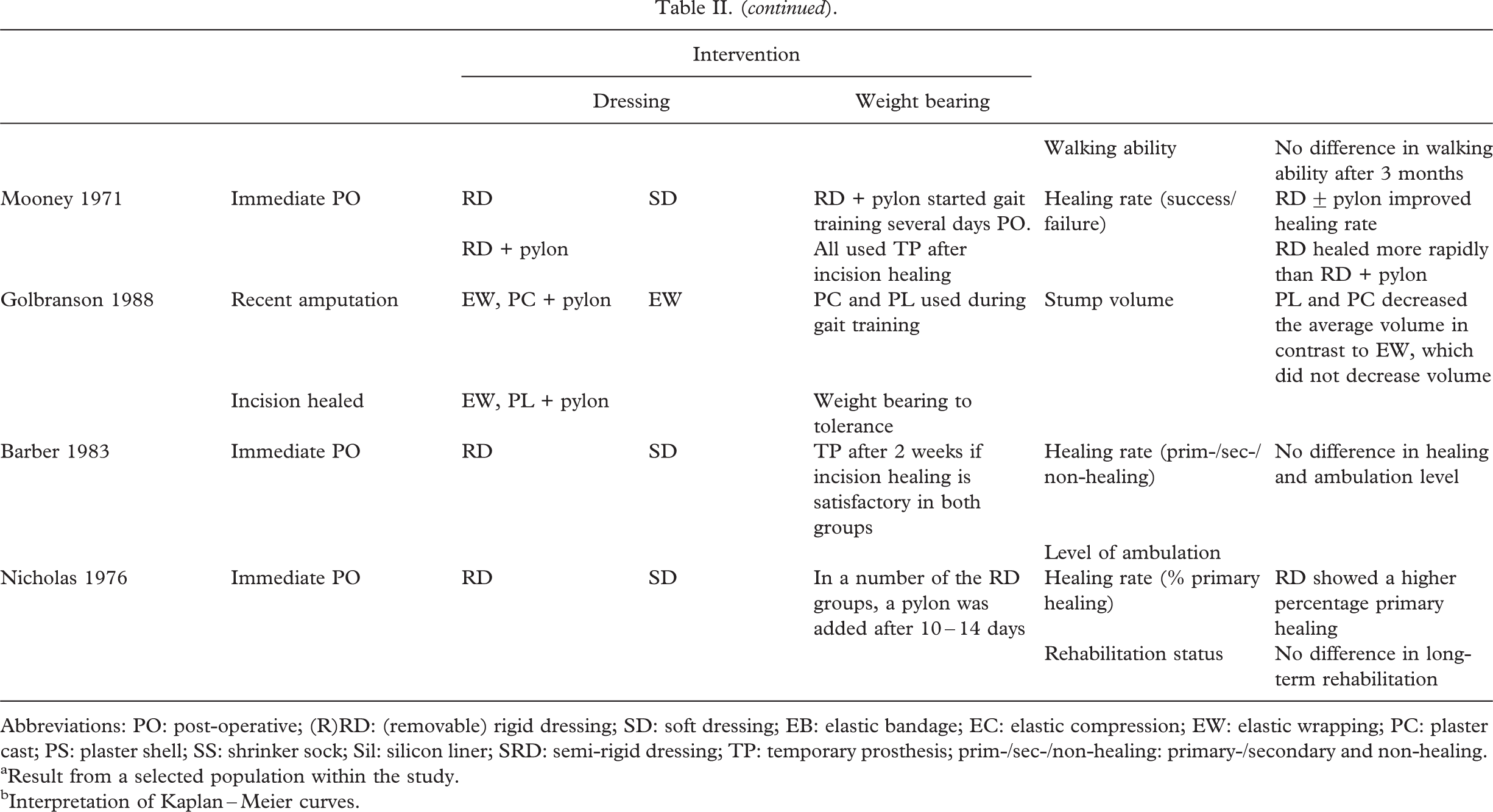
Abbreviations: PO: post-operative; (R)RD: (removable) rigid dressing; SD: soft dressing; EB: elastic bandage; EC: elastic compression; EW: elastic wrapping; PC: plaster cast; PS: plaster shell; SS: shrinker sock; Sil: silicon liner; SRD: semi-rigid dressing; TP: temporary prosthesis; prim-/sec-/non-healing: primary-/secondary and non-healing.
Result from a selected population within the study.
Interpretation of Kaplan–Meier curves.
Stump volume
Residual stump volume was a main outcome measure in one B-level and three C-level studies. Mueller (1982) found a significantly greater degree of stump shrinkage with the Removable Rigid Dressing (RRD) when compared to the use of elastic compression bandages (70.7 ± 21.3 cm3 versus 31.2 ± 49.0 cm3, P < 5.05). The use of elastic bandages did not decrease stump volume significantly in this study, similar to the results reported in the C-level studies of Golbranson et al. (1988) and Manella (1981). Liedberg et al. (1983) found no difference in shrinking rates when using the Tulip limb, i.e. using a temporary prosthesis, compared to no use or use of another temporary prosthesis.
Prosthetic fitting
In the scope of the outcome measures stump healing and stump volume, ‘readiness for prosthetic fitting' constitutes an outcome measure in which both these measures are incorporated. In two C-level studies (MacLean and Fick 1994; Wong and Edelstein 2000), ‘readiness for prosthetic fitting' was a main outcome measure. In the study of MacLean and Fick (1994), time to readiness for prosthetic fitting in the group treated with semi-rigid dressings was found to be half as long as with the treatment of elastic bandages (p = 0.026). In the Wong and Edelstein study (2000), 30% of the patients in the SRD group were found to be ready for prosthetic fitting in 34 days compared to 64 days in the group using elastic bandages (P = 0.025).
Functional outcome
Non-uniform functional outcome was one of the main outcome measures used in two B-level studies and four C-level studies. Vigier et al. (1999) found no significant difference in time to initial success in walking more than 20 m. However, Baker et al. (1977) found a reduced rehabilitation time, i.e. time from amputation to gait training, when using plaster dressing compared to elastic bandages (29.6 days post-amputation versus 35.5 days; standard deviations were not reported). Wong and Edelstein (2000) found that more patients that use a SRD become ambulatory when compared to those who use elastic bandages. Other C-level studies found no differences in functional outcome (Barber et al. 1983; Liedberg et al. 1983; Nicholas and Demuth 1976) as a result of the interventions applied.
Discussion
Methodological quality
This systematic review was performed to establish the optimal stump management after trans-tibial amputation based on the outcome measures wound healing, oedema reduction, and functional outcome measures.
Despite the great number of studies identified by the literature search, no A-level studies were identified. Due to methodological flaws, the results of the B- and C-level studies should be interpreted with caution.
From the methodological assessment of the selected studies, patient selection criteria were found to be the most important in distinguishing between A- and B-level studies. In the authors' opinion, homogeneity of the study population with regard to possible prognostic factors, particularly in relation to wound healing, is a prerequisite for intervention studies on stump healing. Therefore, criteria 2 and 3 were strictly adhered to. However, in the absence of a gold standard for the prediction of stump healing, establishing the optimal cut-off point is difficult when assessing criteria 2 and 3. Vascularization is a major factor in wound healing (Martinez-Hernandez 1988); tissue blood flow at the level of amputation is therefore an important prognostic factor in stump healing. None of the tests used to assess patent peripheral circulation gained general acceptance, while clinical judgement by itself is insufficient to predict the success or failure of an amputation (Sarin et al. 1991). In reviewing the studies on oedema reduction in particular (Golbranson et al. 1988; Liedberg et al. 1983; Manella 1981; Mueller 1982), the assessment of prognostic comparability was similarly carried out. This was done because it was hypothesized that the same factors that affect wound healing would play a role in resolving oedema in the amputation stump. Besides tissue blood flow, other specific factors suggested to affect wound healing after major amputation were reviewed by Eneroth (1999) such as smoking, haemoglobin and/or haematocrit values, malnutrition, diabetes mellitus, previous vascular surgery, and use of prophylactic antibiotics. From these factors, co-morbidity, i.e. diabetes mellitus, was often suggested to be a factor in the studies reviewed.
Stump healing
This review reveals a trend in favour of rigid dressings as compared to the application of soft dressings (including elastic bandages) in order to achieve stump healing. There may be several explanations for the differences in outcomes found in the evaluated studies. For example, measures of stump healing quite often varied between studies. Vigier et al. (1999) studied patients with stumps open by design. Therefore, epitheliazation of the wound was recorded as opposed to incision healing, resulting in a longer healing time. In other studies, primary and secondary wound healing and failure to heal were often not well defined. Homogeneity of the study population, i.e. on prognostic factors was absent in the four C-studies investigating stump healing. Comparison of results between studies is therefore difficult. Furthermore, the age of the study population was not always reported, although in the two B-studies (Baker et al. 1977; Vigier et al. 1999), age groups were found to match. The intervention and timing of the intervention also varied between studies. While, in the study of Vigier et al. (1999), the intervention was initiated less than 3 months postoperatively, Baker et al. (1977) provided direct postoperative. In Baker et al.'s (1977) study rigid dressings were changed first after 14 days as opposed to application of a plaster cast interposed with a silicon liner for up to 5 h a day in the study of Vigier et al. (1999). A relevant shortening of healing time was found in this latter study. The technique of open stump amputation is, however, not considered a routine procedure in vascular amputation surgery. Therefore, these findings limit possible clinical relevance.
Stump volume
The results of the studies investigating stump volume revealed a trend in favour of rigid and semi-rigid dressings when compared to application of soft dressings to achieve reduction of stump volume. In the studies assessing stump volume (Golbranson et al. 1988; Manella 1981), incision healing was already completed at the time of inclusion. Mueller (1982) did not report whether incision healing already occurred, though one could expect incision healing to have occurred by the time of inclusion of patients in the study within 2 months after amputation. Patient numbers in these last three studies were limited. In a larger study, the chance of finding significant differences between the study groups is expected to increase. Volume measurements of the stump were calculated based on circumference and height measurements of the stump. Water displacement was the method of volume measurement in only one (Golbranson et al. 1988).
Prosthetic fitting
Both C-level studies on prosthetic fitting revealed a shortening of time to readiness for prosthetic fitting (MacLean and Fick 1994; Wong and Edelstein 2000) with the use of semirigid dressings when compared to using soft dressings. In the study of Wong and Edelstein (2000), patients with SRD were more likely to be fitted with a prosthesis. However, in the author's opinion, the interpretation of the Kaplan Meier survival curves applied in both studies suggests that inadequate numbers of patients were involved at the time of measurement. These results should therefore be interpreted with caution. It is worth mentioning that in the study of MacLean and Fick (1994), the use of semi-rigid dressings in the experimental group was discontinued at the time of incision healing, after which elastic compression was applied in both control and experimental group and girth measurements began. Continuation of the use of SRD over a longer period could have resulted in more contrast between the study groups.
Functional outcome
No trend can be seen in the effect on functional outcome. This is probably due to the lack of the availability of a uniform standard of measurements, timing, and correction of the effects of confounding factors on the outcome. The authors expect post-operative management to have more effect on early time-related functional outcome measures than on late functional outcome measures as in follow-up. This would explain the results in two C-level studies that found no difference in rehabilitation status and ambulation level in late follow up. Furthermore, the definition of the outcome measure and the timing of follow-up are not well defined. This omission makes it more difficult to interpret the results. Baker et al. (1977) define rehabilitation time as the time between amputation and the initial gait training with a prosthesis. However, in their study, they failed to operationalize this period adequately. Initial success in walking as described in the study of Vigier et al. (1999) was better defined and therefore more valid when investigating functionality. No differences could be found between study groups in this latter study.
The effect of early ambulation or weight bearing is another issue to address. There is only one study (Mooney et al. 1971), in which the design enables the reader to distinguish between the effect of the stump dressing and the effect of early mobilization. In this study, early weight bearing (within days) appeared to lengthen the time until wound healing occurs. Being a C-level study, the evidence presented in this study is of limited value. It is therefore concluded that literature assessed in this review is not conclusive on this issue.
Implications for further research
How can the favourable effects of rigid and semi-rigid dressings on wound healing and oedema reduction be explained? The mechanism described in the introduction of this paper certainly represents an important factor. Oedema reduction will have a favourable effect on the micro-circulation needed to achieve wound healing. Even when the rigid dressing was applied for only 5 h a day, a positive effect was found on wound healing (Vigier et al. 1999).
The authors stress the need for further research on stump management after trans-tibial amputation. In their opinion, emphasis should be on elucidating the mechanisms responsible for the acceleration of wound healing and reduction of oedema, which enables earlier weight bearing. When investigating stump healing, the intervention, i.e. stump dressing should be applied early, preferably on the operating room. This may avoid the development of excessive oedema. When studying these interventions, a randomized controlled trial is the preferable design. In such a study, homogeneity of the patients in particular on possible prognostic factors should be pursued by assessing the peripheral circulation, co-morbidity, and other general factors expected to affect wound healing. These factors involve nutrition status, infection parameters, and others, as reviewed by Eneroth (1999). The effect of early weight bearing should be studied separately from the effect of stump dressings. Time-related outcome measures concerning wound healing, oedema reduction and functional outcome are important, since reduction of time to complete stump healing, stump volume stabilization, and independent prosthetic ambulation is of clinical importance and may generate cost containment.
Conclusion
The results from the reviewed studies show a trend in favour of the application of rigid and semi-rigid dressings compared to the application of soft dressings to achieve stump healing and reduction of stump volume following trans-tibial amputation in vascular patients. More research is needed to confirm these results. An RCT is considered to be the preferable study design.