
Abstract

INTRODUCTION
The concept of hormesis, the stimulatory or adaptive responses to low doses, and nonlinear dose effects are becoming a more prominent and accepted concepts in toxicology and risk assessment (Calabrese, 2003). While many have contributed to the concepts in hormesis, its recent prominence is largely attributable to the detailed and extensive assessment of low-dose effects compiled by Ed Calabrese and Linda Baldwin.
The road to the acceptance of hormesis has been a long and hard one. Most toxicologists have rejected the concept outright as irrelevant or simply ignored it or have simply been ignorant of the literature. The discovery that hormetic effects are evident in over 40% of all studies that meet the criteria for its existence, and that the effects are seen across toxins and phyla have indicated that low-dose stimulatory effects need to be seriously considered in toxicology and biology (Calabrese and Baldwin, 2001).
However, what about clinical medicine? Hormesis is not as prominent a concept in pharmacology and medicine as the title of this journal would indicate. Why is this? Is the concept of hormesis something only of value in toxicology and risk assessment or are there wider implications? To answer this question I suggest that those interested in hormesis examine two areas of potential value — one area is new and largely unexamined, and the second is old and controversial. In examining these areas we should use research and data as the discerning factors and not make the mistake of a priori rejection like others have applied to hormesis and that set it back for so long.
The first area is to examine if low-dose toxins can stimulate reparative processes such that they can used in the treatment of disease. The second is to examine the effects of very low and ultralow dose stimulatory effects. Two articles in this issue of Non-linearity in Biology, Toxicology and Medicine allow us to comment on these areas.
CLINICAL RELEVANCE OF NONLINEAR EFFECTS
Do nonlinear effects have important clinical implications? Toxins are not always poisons and drugs are sometimes toxic. For example, there are several hierarchical dose effects of aspirin, each with clinical implications. These include the differential effects of aspirin on serum thromboxane B2, gastric PGE2 output, and gastric mucosal injury with doses as low as 3 mg/day (Lee, 1994). High-dose aspirin increases bleeding time, but very low-dose aspirin (0.01 mg/day) shows a decrease in bleeding time (De Gaetano, 1988; Doutremepuich, 1990). This effect is modulated by vascular wall endothelium factors, probably prostacyclin (PGI2) (Lalanne, 1990). Some of these effects have gender differences. For example, bleeding time and platelet aggregation react differently in males and females at the same dose (Buchanan, 1983). High-dose and medium dose aspirin are used clinically to inhibit platelet aggregation, but also can cause bleeding in the stomach and intestines. But do the hormetic effects of low-dose aspirin matter clinically? Could low-dose aspirin increase thrombotic events in men, say after surgery, and be used to prevent gastric bleeding from higher doses in both genders? More studies on the effects and mechanisms of low and very low doses of aspirin are needed before we can answer these questions, but their answers could be breakthroughs in clinical medicine.
Another example of the clinical utility of hormesis is the development of tolerance. Cellular and tissue tolerance is a commonly reported phenomenon in allergy desensitization. Could a similar effect be used in developing cellular tolerance to environmental toxins? In this issue, we report on the effects of low and ultralow-dose exposure of normal prostate cells to low and ultralow doses of cadmium for up to 20 weeks (Jonas, 2003). Expression of metallothionein (MT), the primary Cd detoxification protein, was induced by exposure to 10−6 M Cd for over 20 weeks. Cd pretreated cells had delayed transformation compared to controls. In addition, the number of transformed cell mounds was lower in pretreated cells indicating that low and ultra-low dose exposure had protective effects to high-dose Cd induced carcinogenesis. An exaggerated MT response remained even 4 weeks after growth in Cd free media. Thus, it appears that a prolonged protective window of resistance to cellular transformation was induced by exposure to low levels of Cd. The potential clinical utility of this is clear. If the induction of cellular tolerance is a general phenomenon (like hormesis) it may be a simple and safe mechanism for protection from a variety of environmental and perhaps even terrorist toxin exposures. This idea is certainly not any more unlikely than hormesis seemed a decade ago.
HOW LOW DOES BIOLOGY GO?
Do biological systems react to doses even lower than previously thought? One of the major obstacles to the acceptance of hormesis has been a disbelief that very low doses can and do have effects. Thankfully, this concept is gradually eroding as good data accumulates showing otherwise. A second major obstacle to the examination of the clinical utility of hormesis is the association of low-dose treatment with the controversial medical system called homeopathy. The contaminating use of the concept of hormesis by homeopathy in an attempt to legitimize itself has caused a backlash by those interested in the science of hormesis against examining ultralow doses effects (Calabrese, 2002).
Misuse of the concept of hormesis by unscientific groups should not be the driving factor in looking at nonlinear dose effects. Those interested in the science of low-dose responses should not treat ultralow doses such as traditional pharmacology has treated hormesis. Recent reviews of the clinical research on homeopathy have come to unclear conclusions (Jonas, 2003). Before throwing out the bathwater, let's find the baby first. While hormesis does not prove homeopathy, neither should a fear of homeopathy bias scientists
In our prostate cell model of low and ultralow-dose Cd we found that MT was not enhanced in doses below 10−6 M. However, mRNA subtype MT-1G was up-regulated at much lower exposures, and this subtype correlated more closely with delayed transformation from high-dose Cd than any other factor. In a second article in this issue, Elżbieta Malarczyk (2003) and colleagues report on the nonlinear effect of low-dose guaiacol and ethanol on the laccase and peroxidase activities of two strains of Basidiomycetes, Pleurotus sajor-caju and Trametes versicolor. Unlike in most studies, they continued to find nonlinear responses in dose ranges as low as 100−20 mol/L. One of the three reviewers of this article called for outright rejection. The editors of this journal, however, decided to work closely with the authors to assure that their methodology was sound. After going through a meticulous checklist for quality (Table) that was ultimately answered adequately by the authors, it was decided to accept the article for publication. No doubt some readers will object to the publication of any research that claims to show effects below some predetermined level. However, if science is to prevail and if the potential clinical utility of hormesis is to be explored, we must guard against both poor methods and a priori conclusions. In all cases, however, research quality should be the primary judge of value if the clinical utility of hormesis is to be determined.
Quality Evaluation Criteria for Studies on Low-Dose Effects
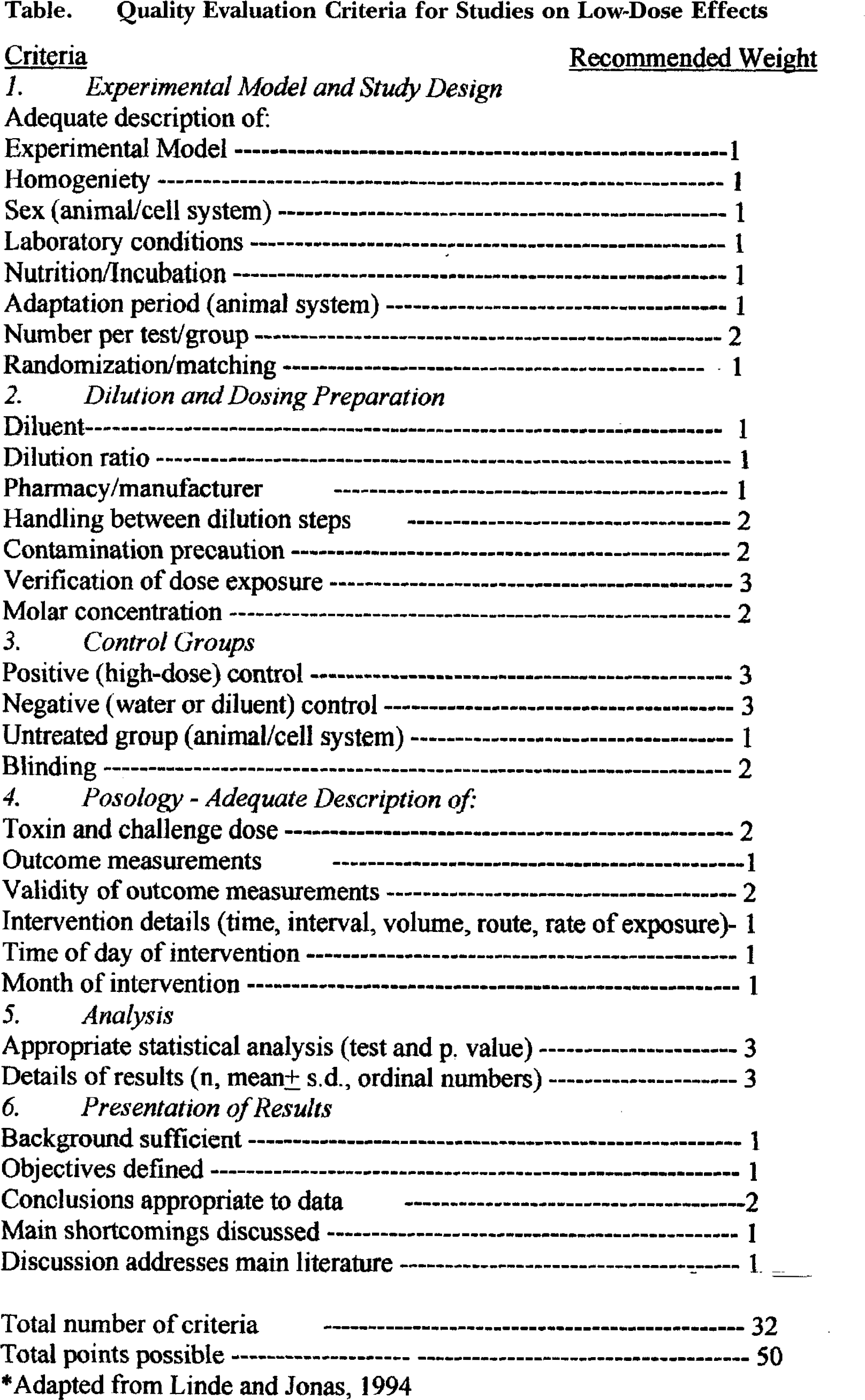
* Adapted from Linde and Jonas, 1994
We recommend that those doing research on hormesis, nonlinear effects in biological systems, and the protective or therapeutic effect of low-dose treatments begin with the quality criteria checklist in the Table of this editorial. We recognize that these criteria will evolve and change as the field matures. Indeed, other guidelines for quality research have also been published (Linde and Jonas, 1994; Jonas, 2001; Calabrese and Baldwin, 2001). We recommend these criteria as a starting point for investigators and reviewers when investigating the topic of protective or therapeutic hormesis.