
Abstract
Mental health court diversionary programs are a key strategy to address over-representation of individuals with a mental illness in the criminal justice system. The study examined 2,476 individuals identified as eligible for mental health court diversion by the Statewide Community and Court Liaison Service (SCCLS) in New South Wales (NSW), Australia and compared reoffending of those granted and not granted court diversion. Individuals not diverted had 43% higher reoffending rate than those granted diversion. Predictors of non-diversion and reoffending included younger age, being male, Aboriginal and/or Torres Strait Islander background, primary personality and/or substance use diagnosis and non-violent offence charges.
Introduction
In Australia and internationally, individuals with mental illness are over-represented amongst those in contact with the criminal justice system (Butler & Allnutt, 2003; Fazel & Seewald, 2012); they are more likely to experience repeated interactions with courts, contact with the custodial system (Chesser & Smith, 2016; Denckla & Berman, 2001), and are at greater risk of repeated incarcerations compared to those without a mental illness (Baillargeon et al., 2009). In response, many jurisdictions have adopted court-based mental health diversionary programs (Chesser & Smith, 2016), such as mental health courts and/or court liaison and diversionary services (Davidson et al., 2019) designed to assist courts with applying the principles of therapeutic jurisprudence (Wexler, 2000), and to link individuals to hospital or community psychiatric care (Bradford & Smith, 2009). By doing so, court diversion aims to address the underlying causes of criminal behavior associated with mental illness rather than apply a punitive approach (Chesser & Smith, 2016; Lim & Day, 2014; Wexler, 2000).
Court diversion and liaison approaches vary across jurisdictions. Internationally, specialized mental health courts are commonly used in the United States (US) (Lange et al., 2011), while court-based diversion and liaison services are the predominant model in the United Kingdom (UK) (James, 2010). Within Australia there are also diverse approaches to court diversion (Davidson et al., 2019). In New South Wales (NSW), local court magistrates have legislative diversionary powers to direct people with mental illness charged with less serious criminal offenses into psychiatric care. It is a pre-adjudication model which only deals with minor criminal charges and allows criminal matters to be diverted or dismissed by magistrates. To facilitate the application of this legislation, local court magistrates have assistance from mental health court liaison services such as the NSW State-wide Community and Court Liaison Service (SCCLS), to help identify those with mental illness likely to meet diversion criteria and to coordinate access to psychiatric care (Bradford & Smith, 2009).
Despite the broad adoption of a range of diversion services and programs in Australia and internationally, the majority of studies have been primarily focused on mental health courts (MHC) in the USA and there is limited evidence of the impact of other diversion models, including in relation to reoffending, in other western countries, including Australia (Davidson et al., 2016; Lim & Day, 2014). Studies in the United States (US) have found evidence of a reduction in recidivism for individuals completing MHC diversion programs, at least compared to those failing to complete such programs (Hiday et al., 2013; Ray, 2014). For example, one study showed the 12 month recidivism rates of MHC program participants (27.5% rearrested) was significantly lower compared to non-MHC program participants (37.3% rearrested) (Hiday et al., 2013), while another found the relative reduction to persist even after 5 years of follow-up (Ray, 2014).
Similarly in the UK, where court diversion/liaison models predominate, individuals with a mental illness who were diverted to hospital were half as likely (28%) to reoffend within two years compared to similar individuals given other disposals such as prison (56% reconviction) or community penalties (58% reconviction) (James, 2010).
In Australia, states with mental health court diversion programs have also reported a reduction in reoffending amongst those completing court supervised diversion programs (Chesser & Smith, 2016; Lim & Day, 2014; Skrzypiec et al., 2004). In 2014, a study of the South Australian Magistrates Court Diversion Program, showed that participants with a mental impairment who completed the court-supervised mental health service intervention had a lower mean number of charges in the 24 months after program completion (1.37 charges, SD = 2.57; p < 0.05) compared to 24 months prior to the program (4.78 charges, SD = 5.98), with program completion identified as the strongest predictor of desistance (Lim & Day, 2014). In Victoria, those who completed a court supervised program also had a lower rate of reoffending when compared to those who did not complete the program (i.e. 49.3% completers versus 18.2% non-completers) (Chesser & Smith, 2016). In NSW, individuals seen by a clinical court liaison service have been found to have lower reoffending rates (Bradford & Smith, 2009). Another recent NSW study, found that individuals with psychosis who were diverted to mental health care were less likely to reoffend (38%) compared to individuals granted a punitive disposal (50%) (Albalawi et al., 2019). This reduction in reoffending was also evident when the cohort was matched with individuals given punitive disposals (Weatherburn et al., 2021), although it was not known whether the comparison group with psychosis who were not diverted were eligible for diversion at the relevant time.
Overall, there is research accumulating across jurisdictions that demonstrates a positive relationship between mental health court diversion and a reduction in reoffending, however, there remain inherent difficulties in rigorously evaluating and comparing the impact of court diversion in different settings due to the diverse nature of services and programs, differences in legislation, and a lack of appropriate comparison groups in many cases (Lim & Day, 2014). While impact on post-diversion reoffending should not be the only measure of success, it remains an important indicator of effectiveness and studies that are able to rigorously evaluate the impact of mental health court diversion on reoffending and identify areas for improvement, in the absence of controlled trial methodology, are much needed.
The aim of the current study is to directly examine the impact of mental health court diversion on reoffending by comparing reoffending rates amongst those granted and not granted diversion, within a cohort of individuals assessed by mental health clinicians as being eligible for court diversion. Court diversion in NSW is defined by the NSW Mental Health (Forensic Provision) Act 1990 and individuals are eligible for diversion if they have ‘mental illness, mental condition, or cognitive impairment’. In the absence of an ability to randomize diversion in such populations, this approach represents the most robust examination of the true impact of mental health court diversion on risk of reoffending, overcoming many of the limitations of previous studies which have relied on either ‘before and after’ comparisons or comparisons to undiverted groups with unknown diversion-eligibility status. In this cohort of individuals assessed by NSW SCCLS mental health clinicians as being eligible for court diversion (n = 8,317) focused on the impact of diversion to either psychiatric hospital or community-based care on subsequent rates of reoffending, we have also considered a range of other potentially moderating and/or confounding factors, including sociodemographic, clinical, and forensic variables.
The variables have been selected on the basis that they have been found in previous studies to be associated with outcomes of mental health diversion, including in previous Australian and international studies that have included the following covariates of age, gender, racial (such as Aboriginal and/or Torres Strait Islander) background, mental health diagnosis, level of socio-economic disadvantage and location (Gaskin et al., 2024; Schlesinger, 2013).
Method
Study cohort
The study cohort was derived from the dataset compiled by the NSW SCCLS and completed by team clinicians (i.e., mental health clinical nurse consultants) based at each of the 22 NSW local courts covered by the service. The SCCLS clinicians prepare reports for the court following assessment of people referred to the service. The reports provide detail on whether an individual is eligible for court diversion based on the presence of symptoms such as delusions, hallucinations and/or severe mood disturbance, and make recommendations to the court on the appropriate mental health services and treatment ordinarily available in the community (Bradford & Smith, 2009). The diversion program does not itself provide mental health treatment or intervention but rather mental health assessments that would not otherwise be routinely available. If a magistrate makes an order for diversion, then the SCCLS clinician will liaise with relevant community or hospital-based mental health services to facilitate diversion. The mental health diversion clinicians do not provide treatment or ongoing care. People assessed by the service are those charged with a non-indictable offense/s, carrying a maximum penalty of 2 years jail, and are not subject to fitness to stand trial assessments or a mental health defense (these are available for indictable offenses dealt with in higher courts).
The cohort includes all individuals aged 18 years and over seen by the SCCLS between 1 July 2008 and 30 June 2015 and assessed by SCCLS clinicians as eligible for any type of mental health court diversion. Court diversion is supported primarily by the NSW Mental Health (Forensic Provision) Act 1990 (“MHFPA”). Under section 32 MHFPA (s32), diversion to community psychiatric care requires the ‘presence of a mental illness, mental condition, or cognitive impairment’, and under section 33 MHFPA (s33) diversion to hospital psychiatric care requires the presence of a condition that seriously impairs the mental functioning of a person and is characterized by the ‘presence of delusions, hallucinations, thought disorder, severe mood disturbance or irrational behavior’. While not the focus of the current study, there are additional pathways for court diversion in NSW supported by other legislation. These pathways include conditional bail, dismissal of charges under good behavior bonds, and transfer to hospital under civil mental health legislation, as well as informal diversion involving referral to mental health services without legislative support.
Figure 1 illustrates the sample selection process for the current study. During the study period, NSW SCCLS clinicians identified people presenting to local court as eligible for any type of mental health court diversion on 8,532 occasions of service contact involving 8317 individuals. For those with more than one contact during the study period, the most recent was selected. Individual linkage to the NSW Bureau of Crime Statistics and Research (BOCSAR) Reoffending Database (ROD) was conducted using probabilistic record linkage methods applied to key identifiers for each individual in the SCCLS dataset (e.g., name, date of birth, and the criminal justice record number known as the Master Index Number (MIN)). The BOCSAR ROD dataset contains information on all finalized court appearances in NSW for all individuals with at least one proven offense, and for the current study we obtained such data for the period 1 July 2008 to 31 August 2019. A total of 6,950 individuals with a documented ‘index offense’ (i.e., the principal offense or most serious charge that led to the ‘index’ court appearance) and a relevant SCCLS contact at which they were deemed eligible for court diversion were identified. Those deemed eligible for court diversion specifically under section 32 and 33 MHFPA (n = 2,476, including hospital transfers recommended under the civil mental health act) were then selected as the final sample for analysis in the current study.
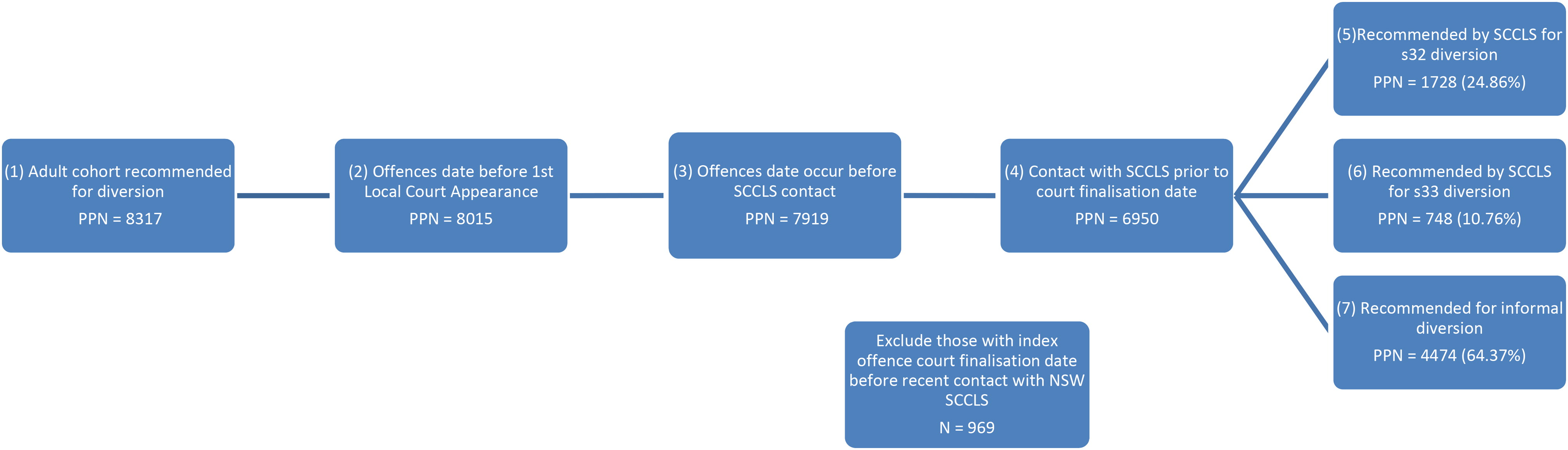
Selection of Study Cohort.
Diversion status and outcome variables
The primary source of diversion status variable and outcome data was the dataset compiled by the NSW SCCLS, including sociodemographic and clinical information recorded by mental health clinical nurse consultants (CNC). The main diversion status variable and outcome, confirmed court diversion under section 32 or 33 MHFPA, was obtained from the NSW Bureau of Crime Statistics and Research’s (BOCSAR) Reoffending Database (ROD), recorded as the finalized court outcome linked to the most serious charge.
The cohort were categorized into 3 age groups (18 to 29 years, 30 to 39 years, and 40 years and over) based on their age when they were assessed by a SCCLS clinician. In addition, key socio-demographic variables such as gender and Aboriginal and/or Torres Strait Islander Status were obtained from the most common categorization recorded for each individual across both the BOCSAR ROD and the NSW SCCLS datasets. The primary diagnoses were taken from those listed by the CNC for each person based on the ICD-10 Classification System and were grouped into serious mental illness (e.g., schizophrenia), personality or substance use disorders and common mental disorder (e.g., ICD-10 categories of depressive disorders, stress-related somatoform disorders and affective disorders). The primary diagnosis was made by the CNCs based on their clinical training and expertise rather than on a standardized assessment process.
The linked BOCSAR ROD dataset provided information on individual criminal charges which were classified according to the Australian and New Zealand Standard Offense Classification system (ANZSOC) (Pink, 2011) and grouped into violent (acts intended to cause injury and sexual assaults), nonviolent (theft, fraud, property damage and related offenses), and minor (e.g., traffic and vehicle offenses) offenses. The BOCSAR ROD also provided information on whether individuals had legal representation at court and the individual’s level of residential remoteness based on the recorded postcode (ABS, 2011). The definition of remoteness was based on the remoteness structure of the Australian Standard Geographical Classification, which uses the Accessibility/Remoteness Index of Australia Plus (ARIA+) score to determine the number of services available to a population (ABS, 2021). For example, “inner regional areas” are generally rural/regional centers in or within a 15 km drive from a town with a population between 15,000 to 50,000 residents. The socio-economic status of individuals was obtained from the BOCSAR ROD in the form of the Socio-Economic Index for Area (SEIFA) variable, based on the socio-economic classification of the area of residence recorded for the individual at the time of their court appearance. The SEIFA index is determined by the employment status and average income of individuals living in specific geographical locations defined by postcode (Pink, 2011).
Individuals were followed from their court finalization date (when all charges are fully determined by the court) for the index offense until their first reoffense recorded in the ROD or until the end of the follow-up period (August 2019), whichever came first. The first reoffense was defined as any finalized charges recorded in relation to an offense (or offenses) occurring on an offense date after the index court finalization date. Furthermore, the study separately examined finalized charges that were categorized as violent reoffenses based on Australian and New Zealand Standard Offense Classification system (ANZSOC) (Pink, 2011a), and analyses were repeated for the first violent reoffense.
Statistical analysis
Statistical analysis was performed using SAS version 9.4. Characteristics of the study cohort were established, and the court diverted group compared to the undiverted group using univariable and multivariable binary logistic regression models, with measures of association reported as odds ratios (ORs) with 95% confidence intervals. The primary outcome variable of reoffense after index offense court finalization date was established using survival analysis. The patterns of reoffending were presented using Kaplan–Meier survival curves, including separately by gender and type of diversion (s32 or s33). Predictors of reoffending, including the primary predictor of interest—diversion—were examined using Cox proportional hazard regression models, with both univariable and multivariable approaches undertaken. Also, a survival analysis specifically for violent reoffending was undertaken. In addition, the prevalence and type of reoffense within discrete time periods (30 days, 12, 24, and 36 months) were examined and chi-square tests used to assess any association between reoffending at different time periods and diversion status. It was assumed that for any periods of time in hospital or custody during the study period, individuals remained at risk of reoffending given that recorded offending, while restricted, was still possible in both circumstances.
Results
Cohort description
Of the 2,476 individuals eligible for court diversion under sections 32 and 33 MHFPA, 1,161 (67.1%) were granted court diversion by the local court magistrate and 815 (32.9%) were not diverted. Most of the study cohort were male (n = 1,827, 73.8%), under 40 years (n = 1,628, 65.8%), major city residents (n = 1434, 60.9%) and did not identify as Aboriginal and/or Torres Strait islander descent (n = 2,060, 83.2%). In addition, the most frequent primary diagnosis category recorded by clinicians was ‘serious mental illness’ (n = 1,409, 57.9%) which included schizophrenia and bipolar disorder most commonly, followed by common mental health disorder (n = 737, 30.3%) and personality or substance use disorder (n = 286, 11.8%). The most common principal offenses were nonviolent (n = 1,496, 60.4%) and most commonly they were theft, public order, and drug-related offenses. Most individuals had legal representation (n = 2,131, 86.1%). Most of the cohort was in the 2nd most disadvantaged of the SEIFA quintiles (n = 937, 39.8%) and lived mainly in major cities (n = 1,434, 60.9%).
Factors associated with being granted diversion
Amongst those deemed eligible for s32 or s33 court diversion, there were a number of factors on logistic regression univariately associated with being granted court diversion (Table 1), including being female (OR 1.52, 95% CI [1.25, 1.86]), having a non-Aboriginal and/or Torres Strait Islander background (OR 1.60, 95% CI [1.29, 1.98]) and having a primary diagnosis of a common mental disorder (OR 2.25, 95% CI [1.69, 2.98]) or serious mental illness (OR 1.93, 95% CI [1.49,2.49]), rather than personality or substance use disorder. Only the primary diagnosis recorded by court mental health clinicians was considered and thus the presence of co-occurring conditions was unknown. Individuals with violent, compared to nonviolent, index offenses were also more likely to be court diverted (OR 2.35, 95% CI [1.61, 3.42]), as were those with legal representation (OR 1.56, 95% CI [1.24, 1.97]). In addition, those who lived in inner regional areas (OR 1.55, 95% CI [1.28, 1.89]) and the 2nd most disadvantaged areas according to the SEIFA Quartile categories (OR 1.96, 95% CI [1.45, 2.65]) were also more likely to be diverted compared to those who resided in major cities and were in the least disadvantaged areas, respectively. In Table 1 the significant relationships between Aboriginal and/or Torres Strait Islander status, gender, diagnosis, principal offense, the 2nd SEIFA Quartile and odds of diversion were largely unaltered on multivariable logistic regression analysis. However, on multivariable logistic regression analysis legal representation was not a significant correlate of diversion.
Associations between sociodemographic and clinical characteristics and the granting of s32/33 diversion amongst those determined to be eligible for diversion, unadjusted and adjusted).
Note. Total Number Eligible for Diversion = 2476.
Adjusted for all other variables (as all factors univariately significant) in the table in logistic regression analysis.
p < .001 ** p < .05 ***.
Prevalence of reoffending
Over the total follow-up period, the prevalence of any type reoffending (minor, nonviolent or violent), amongst all those eligible for court diversion was 57.9% (n = 1,434). The average follow-up period for those eligible for diversion was 2,567 days. There was no significant difference between the average follow up time in days between those diverted (M = 2,582, SD = 765) and not diverted (M = 2,560, SD = 789), t(1432) = 0.61, p = .54. Overall, the most common type of reoffense for both diverted and undiverted individuals was a nonviolent offense.
Table 2 presents the proportion charged with at least one reoffense over discrete follow-up periods, stratified by diversion outcome status (i.e., granted s32/33 diversion versus undiverted). Over the entire follow-up period, the proportion who had a finalized charge with at least one reoffense was significantly lower (χ2 = 34.09, p < .001) for the group granted diversion (n = 755, 53%) compared to those not granted diversion (n = 679. 64.7%). Amongst those reoffending at least once, the diverted group appeared more likely to have a first reoffense that was violent (23.3% vs 20.5%, p < .001). The difference in time to recidivism between the two groups was apparent within 30 days of the finalized court appearance for the index offense, (n = 61, 4.3% for those diverted and n = 63, 6% for those not granted diversion). At 12 months, any reoffending for any offense also remained significantly lower (χ2 = 46.19, p < .001) for those not granted court diversion (n = 366, 34.9%) compared to those who were diverted (n = 321, 22.5%) and the difference persisted up to the 24-month follow-up point (n = 472, 33.1% for those diverted; n = 494, 47.1% for those undiverted). Amongst those with at least 36 months of follow-up time available, a lower proportion reoffended at least once in the diverted groups (n = 687, 48.2%) compared with the diverted group (n = 642, 61.3%) difference again being statistically significant (χ2 = 41.89, p < .001). Table 2 also details the proportion reoffending at least once with nonviolent, violent, and minor offenses across the four time periods, with the patterns seen for any reoffense replicated for the specific offense-type analyses. The exceptions were violent reoffense within 36 months (χ2 = 8.2, p < .06) and minor offenses within 30 days (χ2 = 1.86, p < .17) of court finalization date which were not significant between those court diverted and not court diverted.
Reoffending patterns by diversion (s32/33) outcome.
Note. Total Number Eligible for Diversion N = 2476.
The impact of diversion on incidence of reoffending, along with other predictors
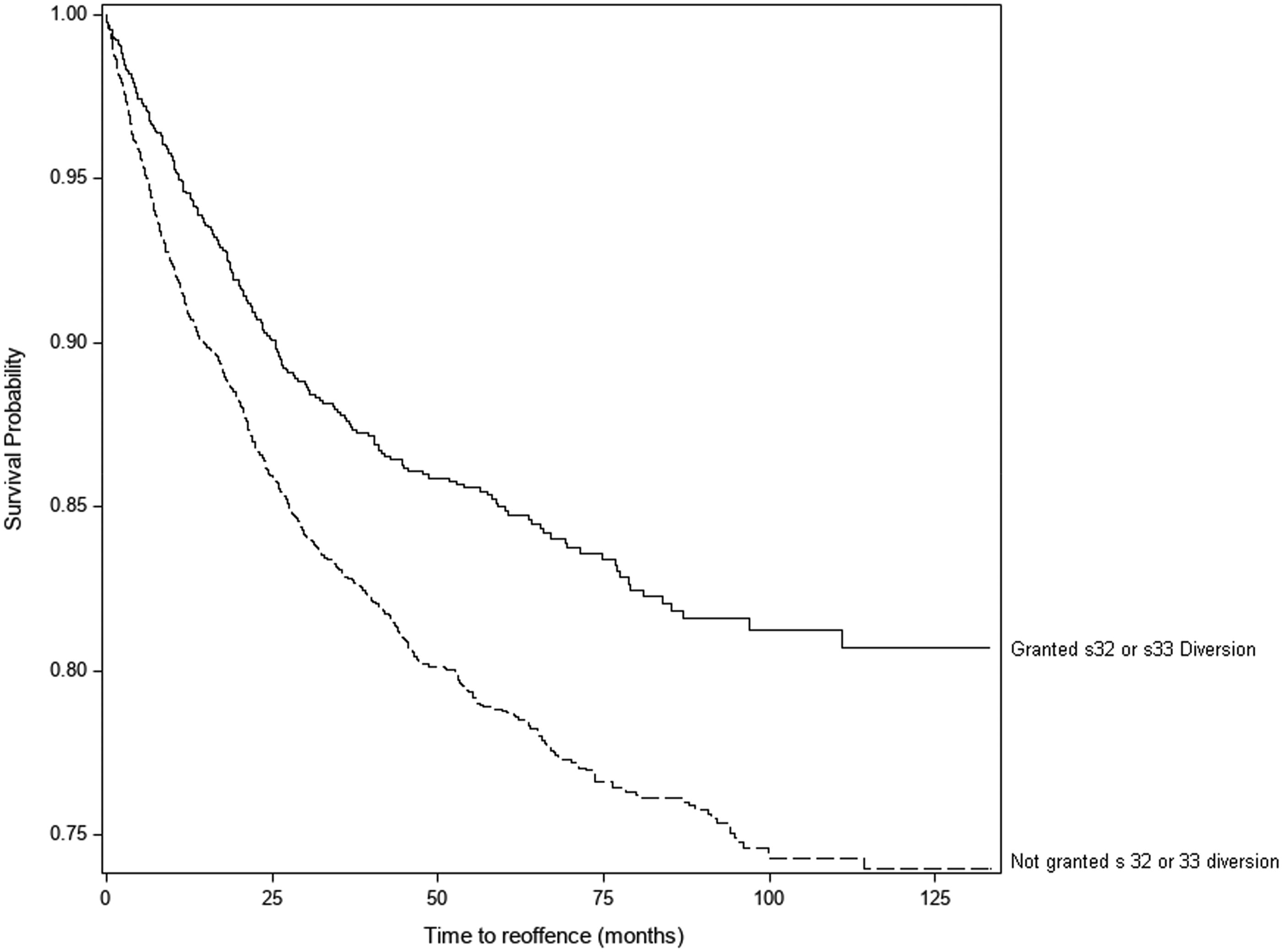
As detailed in Table 3, individuals not granted court diversion had a higher incidence of any type of reoffending (18.52 reoffenses per 100 person years) compared with the group granted court diversion (12.36 reoffenses per 100 person years), with the Hazard Ratio (HR) being 1.43 (95% CI [1.29, 1.59], p < .001) and a significant difference found in time to reoffense (χ2 = 253.98 with 1 df, p < .001). Figure 2 summarizes the pattern of survival to first reoffense for the two groups (diverted and undiverted).
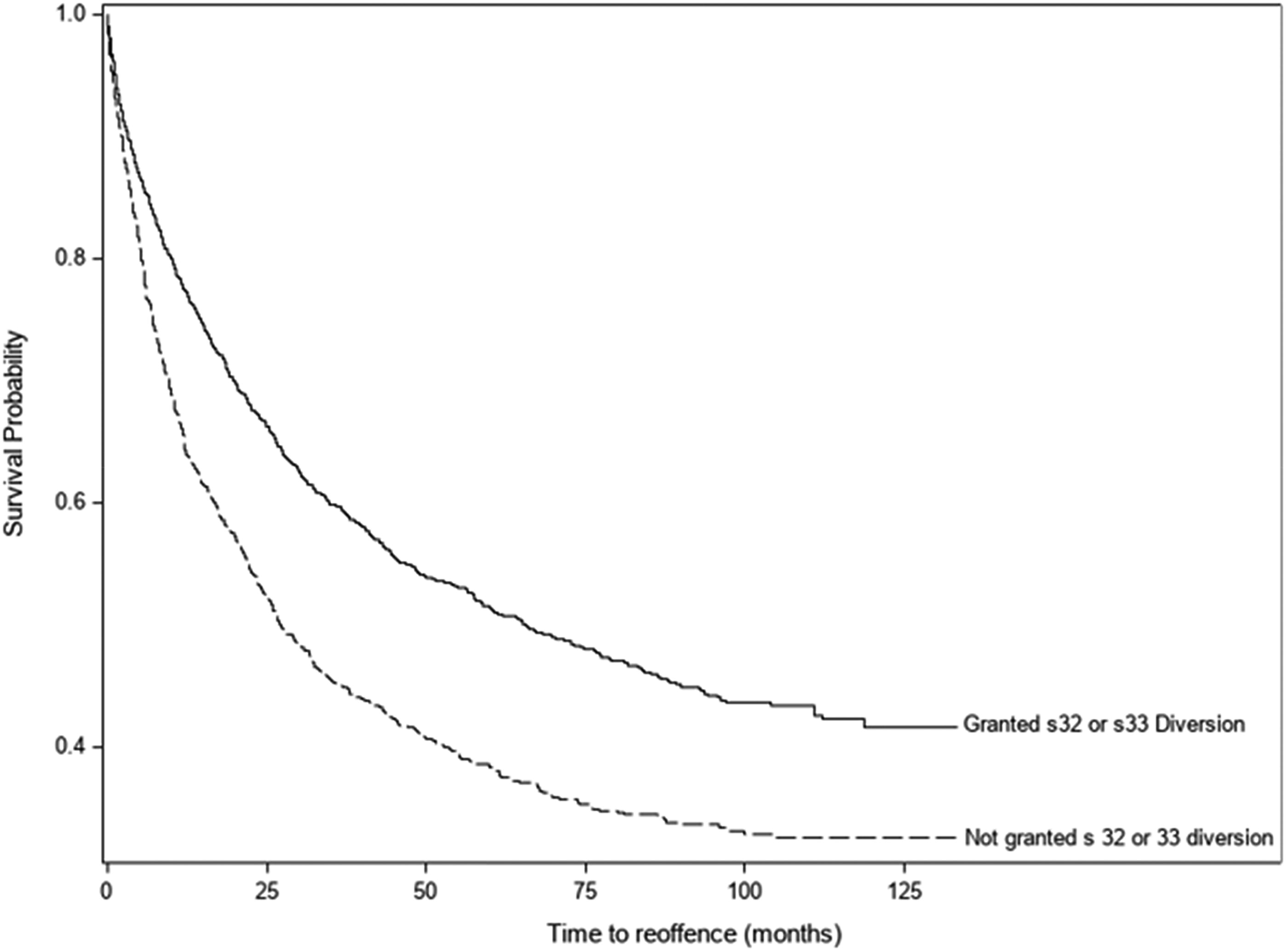
Survival curve – 1st Reoffense after finalized index court appearance amongst those recommended for s32/22 court diversion, by diversion status.
Incidence of reoffending amongst those diverted and undiverted, and in relation to sociodemographic, clinical, and forensic characteristics.
Note. Total Number Eligible for Diversion = 2476.
Adjusted for all other variables in the table using Cox’s proportional hazards regression.
p < .001.
p < .05.
The likelihood of reoffending for any offense was higher for men than women (HR = 1.44, 95% CI [1.27, 1.63], p < .001) and for those of Aboriginal and/or Torres Strait Islander background (HR = 1.60, 95% CI [1.41, 1.82], p < .001). For primary psychiatric diagnosis, individuals with a personality or substance use disorder (HR = 1.67, 95% CI [1.41, 1.98], p < .001) were more likely to reoffend compared to individuals diagnosed with a serious mental illness (HR = 1.19, 95% CI [1.06, 1.34], p = .005). While those charged with a nonviolent principal offense were more likely to reoffend (HR = 1.24 95% CI [1.09, 1.41], p < 0.001) compared to those charged with minor or violent offenses. Major cities residents were significantly more likely to reoffend (HR = 1.29, 95% CI [1.15, 1.46], p < 0.001) than inner or outer regional/remote area residents. However, there was no significant difference in reoffending by SEIFA (area-level socioeconomic status).
In Table 3, after adjusting for the univariately significant covariates (i.e., age, gender, Aboriginal and/or Torres Strait Islander status, primary diagnosis (personality or substance use disorder), type of principal offense (nonviolent), and urban residence), individuals not granted court diversion continued to have a significantly higher proportion of reoffending (adjusted HR = 1.24, 95% CI [1.11, 1.39], p < .001). In addition to diversion status, the following factors were also independently associated with reoffending on multivariable Cox regression analysis: age, gender, Aboriginal and/or Torres Strait Islander status, primary personality or substance use disorder, nonviolent principal offense, and residential location in a major city.
Figure 3 presents a survival curve for reoffending for any offense comparing the diverted and undiverted groups but separating the two types of court diversion (i.e., s32 and s33). Both diversion types were associated with a reduction in reoffending compared to the undiverted group, but the lowest time to recidivism were for section 32 diversion (χ2 = 61.21 with 2 df, p < .001). When stratified by gender (Figure 4), the incidence of reoffending in men (17.78 reoffenses per 100 person years) was higher than for women (11.03 reoffenses per 100 person years). Undiverted men had the highest proportion of reoffending, followed by men granted diversion, undiverted women and lastly, women granted court diversion were least likely to reoffend. The groups differences were significant (χ2 = 73.61 with 1 df, p < .001).
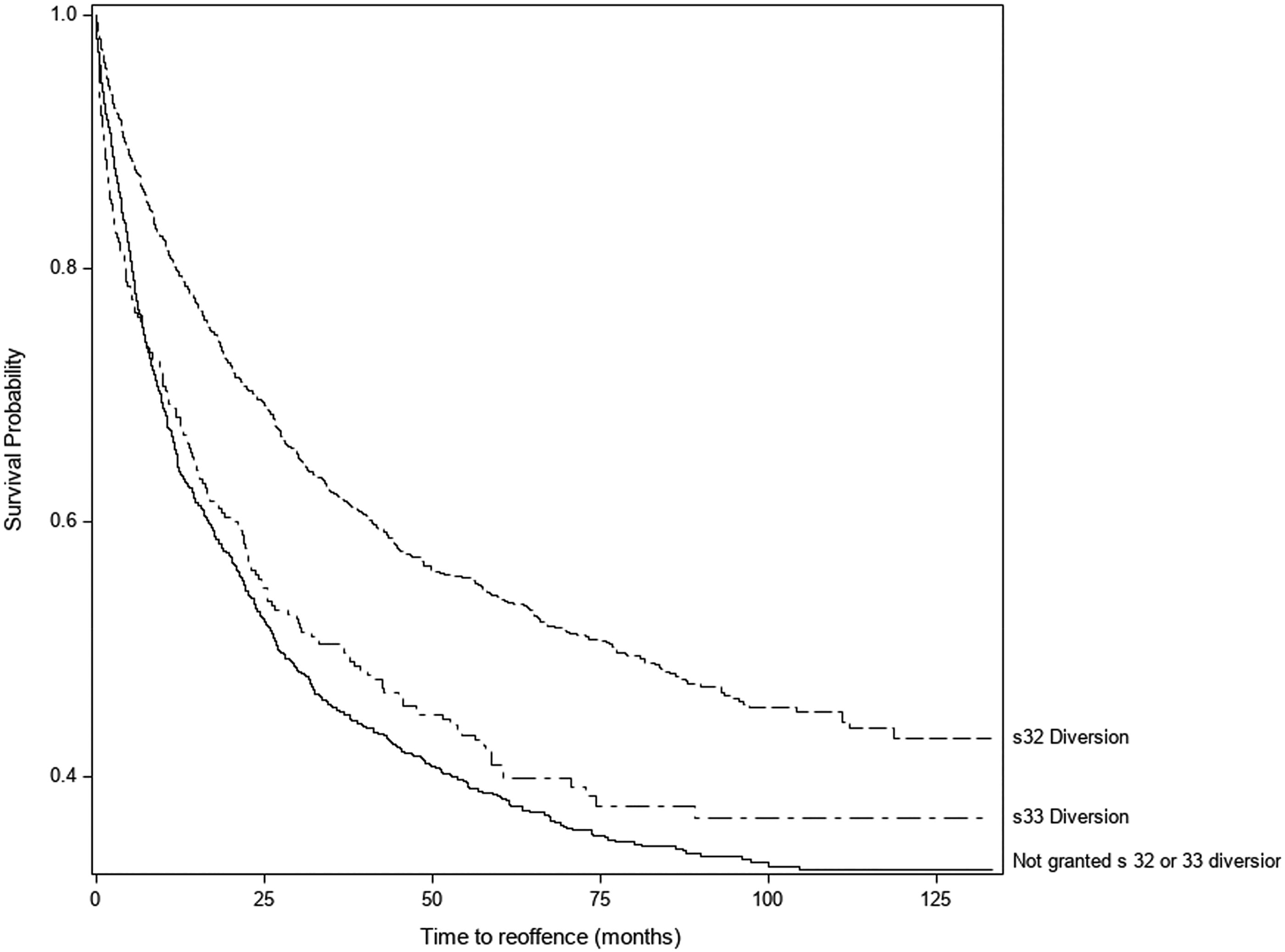
Survival curve – 1st Reoffense after finalized index court appearance amongst those recommended court diversion (s32/33) comparing those granted section 32, section 33 or no diversion.
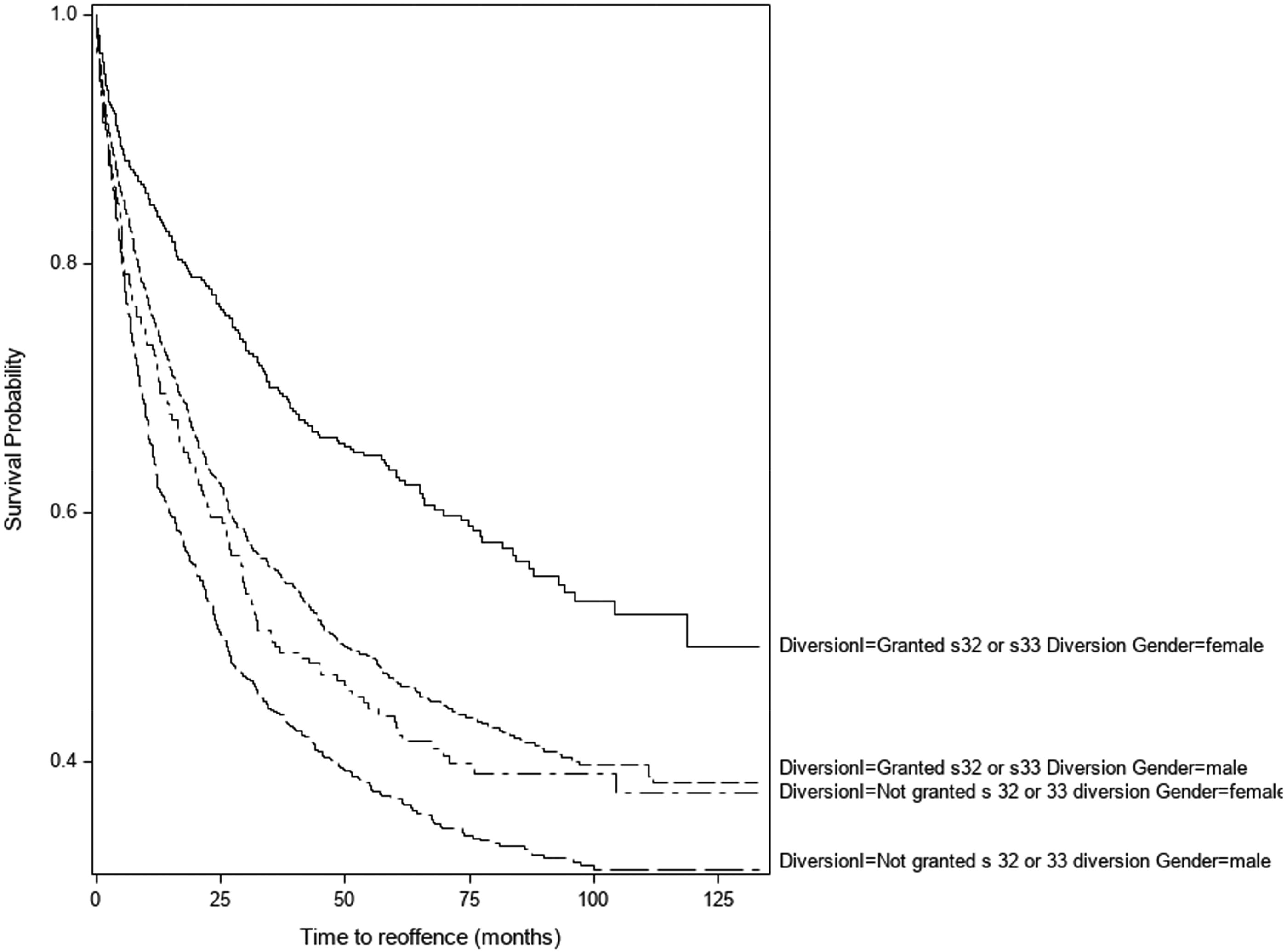
Survival curve – 1st Reoffense after finalized index court appearance amongst those recommended court diversion (s32/33) by gender and diversion outcomes.
The impact of diversion on incidence of violent reoffending
Those not granted court diversion had higher proportion of violent reoffending compared to the diverted (incidence rate 3.79 per 100 person-years for the undiverted group compared to 2.88 per 100 person years in the diverted group; see Figure 5 for survival curve; χ2 = 23.79 with 1 df, p < .001). Time to violent reoffense was also shorter amongst the under 40 years age group (18 to 29 years HR = 1.90, 95% CI [1.44, 2.05], p < .001 compared to 30 to 39 years HR = 1.59, 95% CI [1.18, 2.10], p < .001), males (HR = 1.52, 95% CI [1.16, 2], p = .006), those with a personality or substance use disorder diagnosis (HR = 1.61, 95% CI [1.13, 2.30], p < .05), and major city residents (HR = 1.47, 95% CI [1.14, 1.89], p < .001). In multivariable Cox regression analysis (Table 4), the association between diversion status and violent reoffending was not statistically significant but the other univariately significant predictors remain significantly associated with the incidence of violent reoffending.
Survival curve – 1st violent reoffense after finalized index court appearance amongst those recommended court diversion (s32/33), by diversion status.
Incidence of reoffending amongst those diverted and undiverted, and in relation to violent offenses.
Discussion
In this study of people with mental illness presenting to local court in NSW and determined to be eligible for diversion, those actually diverted from the justice system to mental health services had a significantly lower rate of subsequent reoffending compared to those who were not diverted. Individuals not granted court diversion had a rate of reoffending for any offense that was 43% higher than those granted court diversion, and the association persisted after controlling for a range of key covariates. We also found court diversion to be associated with reduced time to violent recidivism, but the association was not significant on multivariable analysis, indicating that the impact on violent reoffending was at least in part due to the higher risk status of the non-diverted group rather than the direct impact of diversion.
Main findings
Factors associated with diversion
The cohort’s socio-demographic and clinical characteristics were comparable to other published descriptions of court diversion/liaison service samples and mental health court programs in NSW and internationally (Albalawi et al., 2019; Ray, 2014; Rowlands et al., 1996; Sharples et al., 2003). In the current study, a lower proportion of the sample was of Aboriginal and/or Torres Strait Islander background (17%) compared to the reported proportion for those with finalized court appearances at any court in NSW in 2021 (23.1%), this difference may reflect the increased frequency of court appearances involving Aboriginal and/or Torres Strait Islander people (BOCSAR, 2021), a reduced rate of referral to the SCCLS for this group, or problems of under-reporting in the data sources we relied on.
In the current study, 1,661 (67%) were granted court diversion despite 2,476 individuals being identified by NSW SCCLS mental health clinicians as eligible for court diversion under sections 32 (community-based diversion) and 33 (inpatient-based diversion) of the relevant NSW legislation (MHFPA). There were significant differences between individuals granted and not granted diversion by magistrates with regard to their socio-demographic and clinical characteristics. Individuals had increased likelihood of court diversion if they were aged over 40 years, female, of non-Aboriginal and/or Torres Strait Islander background, had a primary diagnosis of a common mental health disorder (e.g., depression), were charged with a violent index offense, had legal representation, or lived in an inner regional area. These findings, including differences in court diversion rates by gender, ethnicity, diagnosis and type of offense, have previously been reported in other Australian studies (Albalawi et al., 2019; Sharples et al., 2003).
These results suggest that for certain groups considered eligible for court diversion, there are barriers to accessing court diversion, highlighting the need to better understand the court diversion decision-making process. Particularly worrying is the lower rate of court diversion for Aboriginal and/or Torres Strait Islander people in this study and others (Albalawi et al., 2019), despite the well-known need to address the over-representation of Aboriginal and/or Torres Strait Islander people within the criminal justice system in Australia (BOCSAR, 2021). The lower rate of diversion in this population may be related to a number of factors including racial bias, an increased likelihood of multiple charges, and a higher rate of previous criminal convictions that may impact on a magistrate’s assessment of the appropriateness of court diversion and thus influence sentencing (Joudo & Joudo, 2008; Snowball & Weatherburn, 2007).
Another group less likely to be diverted were those with primary substance use and/or personality disorders, which is consistent with other NSW-based court diversion studies (Albalawi et al., 2019; Sharples et al., 2003). This may be explained by the nature of the legal definition of mental illness contained in diversion legislation but it does highlight an important area of unmet clinical need. Moreover, the lower rate of court diversion for those charged with nonviolent offenses (including drug-related offenses) may reflect the availability of alternative effective diversion options, such as the NSW Magistrates Early Referral into Treatment (MERIT) programs, for those with substance use problems (Larney & Martire, 2010) or the belief that nonviolent property offenses are associated with higher rates of reoffending (Agnew-Pauley & Holmes, 2015; Weatherburn et al., 2021). Interestingly, the higher likelihood of court diversion for individuals charged with violent offenses may have occurred because magistrates perceive a clearer causal link between mental illness and violence (Gotsis & Donnelly, 2008). Those with legal representation may have had better court diversion rates because legal representatives facilitate viable treatment plans, a critical factor in magistrates supporting community-based mental health diversion (Gotsis & Donnelly, 2008). For older individuals and women, the increased likelihood of court diversion may reflect a range of other factors such as the seriousness of the offense, previous offending history and perceptions of likelihood of treatment compliance (Senior, 2011) or reoffending.
Factors associated with reoffending
Amongst those with mental illness eligible for court diversion, the granting of court diversion was associated with a significantly lower time to recidivism. This pattern of reduced reoffending for individuals granted mental health diversion extended across the discrete follow-up periods examined (30 days to 36 months) and across different types of reoffenses including violent, nonviolent, and minor offenses. There was, however, little apparent difference in the proportions found across different types of reoffenses between the court diverted and non-diverted groups, limiting the extent to which these findings are meaningful in practice. Other studies have reported a reduced rate of reoffending amongst those granted court diversion (Albalawi et al., 2019; Bradford & Smith, 2009; Weatherburn et al., 2021) but no previous studies have compared the reoffending rates for diverted individuals to a control sample also deemed to be eligible for such diversion at time of the relevant court appearance.
In addition, those diverted under section 32 to community mental health treatment were found to have a lower proportion reoffending compared to those diverted under section 33 to hospital. This may relate to the severity of mental illness, the effectiveness of mental health treatment (hospital vs community), and the underlying risk of reoffending posed by the two subgroups of diverted patients. This finding requires replication in larger samples and further examination to understand the underlying factors driving any difference in reoffending outcomes.
Beyond the granting of court diversion, a number of socio-demographic and other characteristics were independently associated with an increased risk of reoffending and including factors also found to be associated with a lower likelihood of diversion being granted. The factors associated with not being granted court diversion included being in a younger age group (under 40 years), being male, having an Aboriginal and/or Torres Strait Islander background, having a primary personality and/or substance use diagnosis, having a nonviolent index offense charge and living in a major city. Risk of reoffending following the index offense was associated with younger age (under 40 years), being male, having an Aboriginal and/or Torres Strait Islander background, having a primary personality and/or substance use diagnosis, having a nonviolent index offense charge and living in a major city. Thus, the characteristics of those ‘at risk’ of not being diverted are very similar to those associated with an increased risk of reoffending. More research is needed to understand the barriers to diversion, why diversion fails to prevent reoffending for some groups, and how interventions for ‘at risk’ individuals might improve diversion and criminal justice outcomes. Finally, it is important to note that the association between diversion and a reduced rate of violent reoffending was rendered non-significant once other correlates of violent reoffending were accounted for. This finding suggests the association with violent reoffending may be largely due to the higher risk status of the undiverted group rather than supporting a direct impact of diversion itself but replication in a larger sample is needed to confirm this result.
Limitations
The current study benefits from enabling a direct comparison between diverted individuals and an undiverted control group also deemed eligible for diversion which, in the absence of the ability to conduct randomized controlled trials in the field, adds robust evidence to the literature supporting the notion that mental health diversion at court can reduce reoffending. It also benefits from including data from both a comprehensive clinical service database and official criminal records, reducing the likelihood of sampling and information biases, as well as enabling examination of a wide range of covariates. There are, however, several potential limitations arising from the nature of the data sources. Firstly, the information available in the study is limited to information routinely recorded by SCCLS clinicians and available in the BOCSAR ROD, resulting in the possibility of misclassification errors and an absence of information on several potential factors of interest (e.g., individual-level socioeconomic status, and reoffending outside the NSW jurisdiction). Secondly, the study is limited to an examination of the first stage in the diversion process (i.e., the legal granting of diversion by a magistrate), while the nature and outcome of the mental health treatment received by individuals following diversion is unknown. In addition, there is no specific information available on the factors that contribute to a Magistrates’ decision about mental health diversion. While the study sample size was relatively large compared to other research in the field, the power to examine associations between diversion and violent reoffending may have been insufficient. Furthermore, the study was unable to censor for deaths that occurred during the study follow-up period. Finally, it is difficult to generalize the findings of this study to other jurisdictions with different legislative, judicial, and healthcare contexts.
Conclusion
The study findings support the notion that mental health court diversion is an effective strategy to improve the criminal reoffending outcomes for individuals with a mental illness. However, it is important to acknowledge that there are barriers to accessing such diversion, particularly for those who are male, of younger age, of Aboriginal and/or Torres Strait Islander background, who do not have a diagnosis of a serious mental illness (such as schizophrenia), who are non-urban residents or who are charged with nonviolent offenses. Similar factors may drive reoffending, adding to the likelihood of a poor outcome. In meeting the mental health needs of those presenting to court, diversion may actually be one of the few interventions consistently found to be associated with reduced recidivism. It should be expanded and supported where possible, reducing barriers to access, and improving outcomes for those at particular risk. Further research is required to better understand the barriers and to develop incentives and interventions to improve the rates of mental health diversion for all eligible individuals.
Footnotes
Conflict of interests
The author(s) declared the potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Two authors of the paper are clinicians for the Statewide Community and Court Liaison Service (SCCLS) and have clinical responsibility for individuals seen by the service. The opinions expressed do not represent the opinions of the Justice Health & Forensic Mental Health Network (JH&FMHN).
Acknowledgements
The authors would like to thank and acknowledge the NSW Statewide Court & Community Liaison Service (Justice Health & Forensic Mental Health Network, NSW, Australia) and the clinicians working within that service for their diligence.