
Abstract
In this systematic review, we aimed to identify facilitating or hindering factors for patient participation in inpatient forensic psychiatric care. Ten studies, qualitative (n = 8), quantitative (n = 1), and mixed method (n = 1), were included. Findings were categorized using the European standard for minimum requirements for patient involvement in health care. We identified a supportive care relationship as an essential prerequisite for participation. This includes ensuring that patients feel trust, included in discussions, and seen as a person, beyond the index crime but with an understanding for their psychiatric illness. Patients’ transition phases through their illness and the forensic psychiatric care system initially appeared to negatively influence patient participation. However, as they approached their release from forensic psychiatric care, a positive shift in their willingness to participate in their care became evident. Factors such as stigmatization, safeguarding one’s own security, and the coercive forensic psychiatric care environment, were identified as factors significantly hindering patient participation. Moreover, patients perceived participation in care planning as confusing, as they felt excluded from influencing any care-related decisions. Staff, in contrast, were restrictive with information regarding patient care, which had additional negative effects on patients’ understanding of their situation. We conclude that future research is needed to examine clinical routines and strategies that may improve patient participation. Furthermore, more quantitative research is needed to examine the challenges for this specific patient population and environment. Future interventions should focus on improving the quality of relationships, information-sharing, and patient involvement in key elements of forensic psychiatric care.
Introduction
Forensic psychiatric care (FPC) is specialized psychiatric healthcare provided in secure psychiatric units, often in forensic psychiatric hospitals or specialized wards. Patients within this context present a complex combination of psychiatric disorders, often alongside antisocial and offending behaviors. Their forensic psychiatric care treatment is shaped both by their mental health needs and their involvement with the criminal justice system (Nedopil, 2016). Moreover, forensic psychiatric care is known internationally to be a complex and multifaceted field with lengthy stays. A significant increase in the average treatment duration for patients in forensic psychiatric care over the past two decades has been noted in several studies, including the total duration of treatment and the proportion of patients receiving longer treatment periods (Connell et al., 2019; Jansman-Hart et al., 2011; Rutherford & Duggan, 2008; Tomlin et al., 2021). This was also recently exemplified in a Swedish study reporting that depending on factors such as type of offense and specific diagnosis, treatment duration in forensic psychiatric care varied significantly (Sivak et al., 2023). Long-term institutionalization and deprivation of liberty within forensic psychiatric care systems underscore the necessity for evidence-based methods that support the patients’ involvement in their care. Methods that advocate for patient involvement are considered a decisive factor to successful discharge planning (Britten et al., 2020). To address this imperative, our systematic review aims to examine key factors related to patient participation in forensic psychiatric care.
Patient participation encompasses a spectrum of actions, including sharing information and knowledge with patients, fostering a common understanding of care objectives, supporting strategies for self-care and actively engaging patients in intellectual and/or physical activities. This definition extends beyond mere involvement in treatment decisions and is aligned with established models of patient participation (European Committee for Standardization, 2020; Sahlsten et al., 2008).
Patient participation should be understood in a broad sense where participation versus nonparticipation relates to an individual’s sense of control, a fundamental aspect of the human experience. Furthermore, it is connected to the need for care, encompasses prior experiences, and involves the personal journey from illness to health, all aimed at enhancing the overall care process (Eldh et al., 2004). However, quantitative studies have consistently shown that patients and staff in forensic psychiatric care report the lowest ratings concerning care quality in regard to patient–staff communication, involvement in treatment decisions, and participation in care plans (Carlin et al., 2005; Lundqvist & Schröder, 2015; Schröder et al., 2016).
The European standard for patient involvement in healthcare—minimum requirements for person-centred care, developed by the European Committee for Standardization (CEN) in 2020, is a comprehensive framework, designed to enhance patient involvement in healthcare processes across Europe. It draws on international best practices and research to establish guidelines for patient participation in critical areas such as patient-provider communication, shared decision-making, and documentation.
Research reports that forensic psychiatric care is characterized by high levels of control, low patient participation and long inpatient care periods (Askola et al., 2018; Nedopil, 2016). Patients within the forensic psychiatric care system, often feel powerless and stigmatized. They depict a struggle against the forensic psychiatric care system, wanting to escape care rather than being genuinely motivated to participate in care (Hörberg et al., 2012). These circumstances, along with staff members’ varying levels of willingness to encourage participation, create exceptional challenges to promoting patient participation in forensic psychiatric care settings (Jacob & Holmes, 2011).
Although the management of offenders with psychiatric disorders varies within and outside Europe, there are overlapping core challenges and dynamics, often revolving around the delicate balance between providing ethically acceptable care for individuals with severe mental health issues and upholding public protection and safety (Robertson & Walter, 2008; van der Wolf & van Marle, 2018). Moreover, security must be prioritized in everyday clinical decision-making (Nedopil, 2016; Svennerlind et al., 2010). It is argued that forensic psychiatric care staff struggle with a “dual-role dilemma”, alluding to the dichotomy of caring for patients while protecting society from offenders with psychiatric disorders (Robertson & Walter, 2008). Individuals in forensic psychiatric care are trapped between being a patient and an incarcerated criminal (Holmes & Murray, 2011; Mezey et al., 2010).
Despite the growing adoption of participatory approaches, such as person-centered care, by organizations like WHO, nursing guidelines and European standards, factors affecting patient participation in forensic psychiatric care have not yet been systematically presented in the literature (European Committee for Standardization, 2020; WHO, 2015). This study aimed to summarize the key factors that influence patient participation in forensic psychiatric care. Ultimately, we hope that this review may support future implementations of patient participation in forensic psychiatric care settings.
Methods
Literature search strategy
A systematic mixed-method review was conducted, according to the PRISMA methodology (Page et al., 2021), and registered in PROSPERO (CRD42021255684). The literature search was conducted by VVA, with assistance from librarians at the University of Gothenburg, Sweden, utilizing three electronic databases: Scopus (which includes PubMed), CINAHL, and PsycINFO. Search terms and research questions, formulated within a Population, Exposure, and Outcome (PEO) framework (Figure 1), were collaboratively established by the librarians and three authors (VVA, EA, SO).
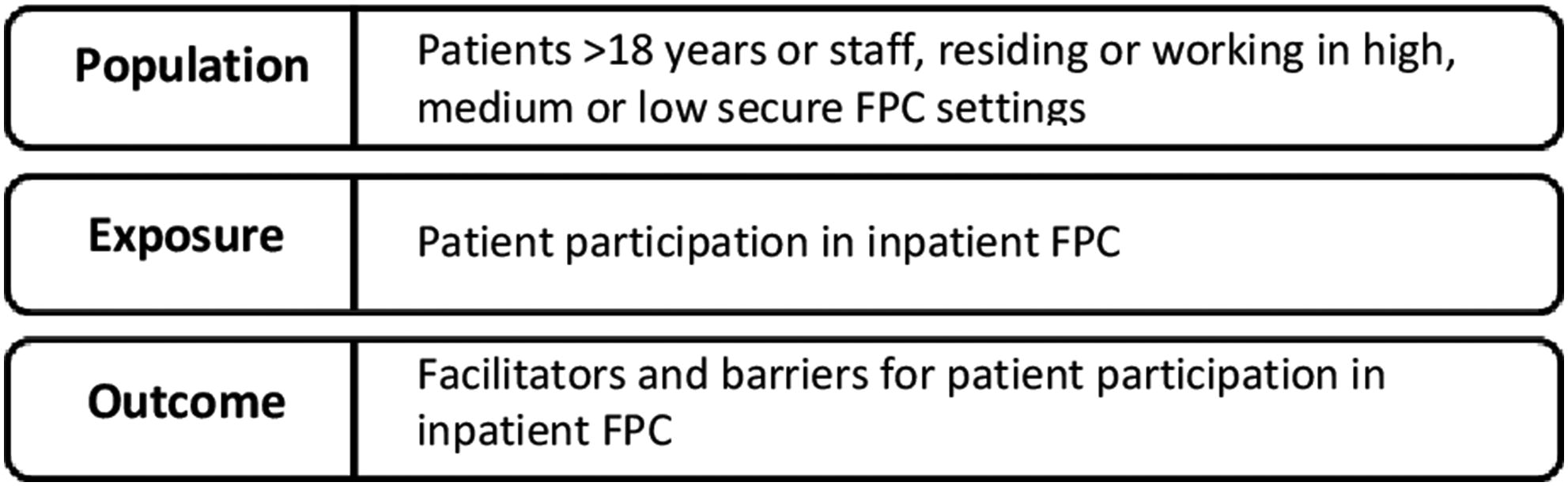
Population, exposure, and outcome framework.
Inclusion and exclusion criteria (Table 1) were determined based on the PEO framework and through collaboration between all authors.
Inclusion and exclusion criteria for published articles.
Database searches were conducted on several occasions, the first in March 2021 and the latest in February 2022, securing the inclusion of newly published articles. The searches resulted in a total of 951 items (Scopus n = 465, PsycInfo, n = 448, CINAHL n = 38). All items were exported to the Rayyan intelligent systematic review screening program. Duplicates and items clearly not meeting the inclusion criteria were removed by VVA. The remaining items (n = 360) were independently blind-screened by three authors (VVA, SO, EA). The 65 remaining items underwent another blind-screening of abstract and full text, and 15 remaining items were assessed for eligibility. The database search produced eight articles (Figure 1). Supplementary searches in journals and reports in the forensic psychiatric care field were undertaken to identify any additional, initially overlooked, studies. This comprehensive search strategy resulted in the inclusion of two additional articles. Additional studies identified through organization or citation searching were discussed by the researchers and the librarian. The former discussed differences of opinion until a consensus was reached. Ten articles in total were selected for the literature review (Figure 2).
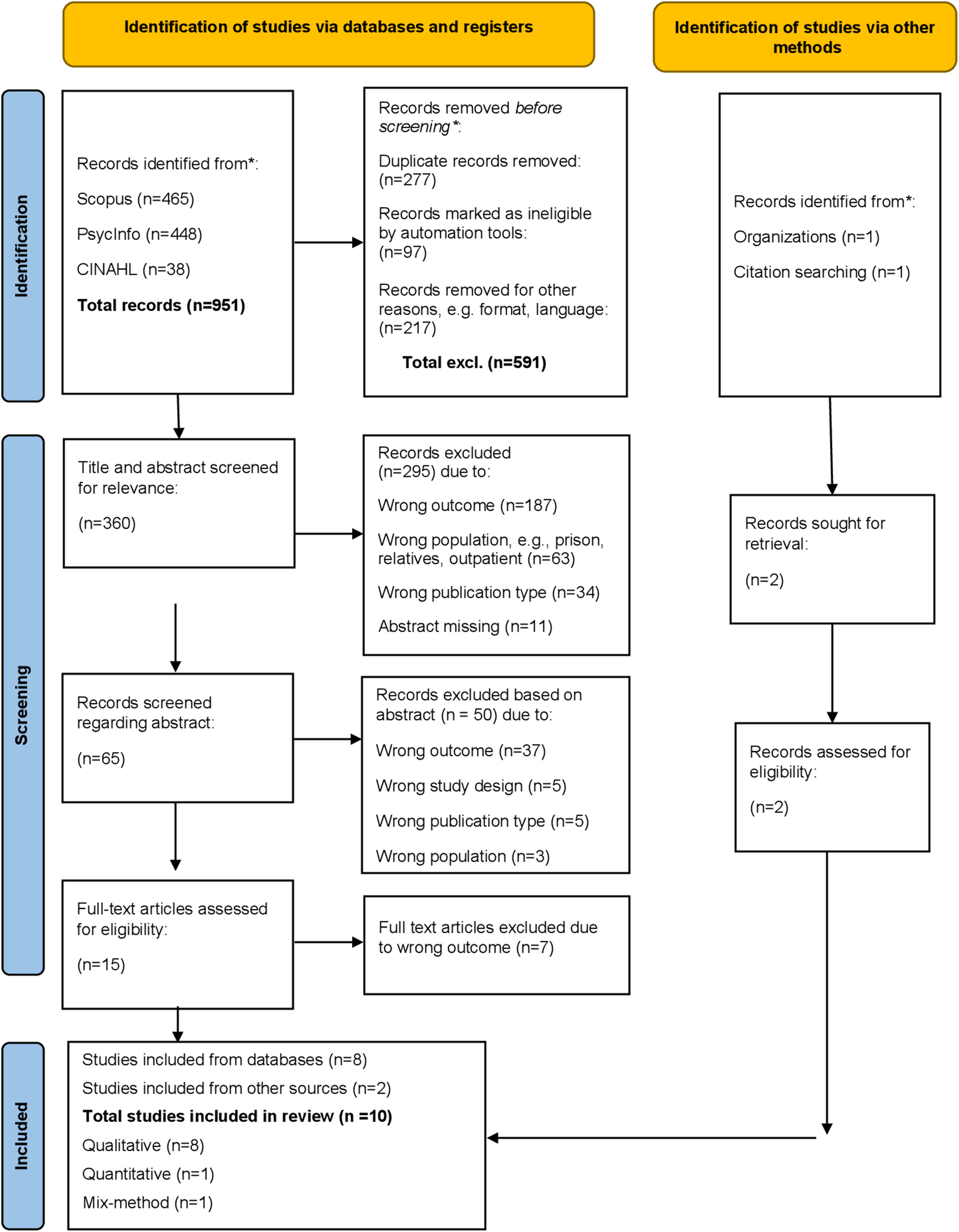
PRISMA flowchart.
Quality assessment
We conducted a quality assessment of the included studies using the framework by Caldwell et al. (2005), covering both quantitative and qualitative aspects (Table 2). While this did not solely determine study inclusion, it facilitated the evaluation of methodological rigor and overall evidence quality. Throughout the analytical process, the quality assessment findings guided our interpretation of results and informed our discussions on the implications of the included studies. Our objective was to find a balance between acknowledging the strengths and limitations of the evidence and drawing meaningful conclusions about patient participation in inpatient forensic psychiatric care.
Overview of studies.
PCC: person-centered care; FPC: forensic psychiatric care.
Analysis and synthesis
Data extraction was performed according to Bettany-Saltikov and McSherry (2016) and data analysis followed Braun and Clarke (2006) method for thematic analysis. We extracted general information (Table 2) and information addressing the research question (direct quote, summary backed up by a quote or quantitative data). Thereafter, the process of analysis continued in both an inductive and a deductive stage.
Inductive stage
All included studies were read repeatedly. Data were extracted by VVA and critically revised by SO. Included studies were repeatedly examined and evaluated to ensure that they accurately reflected the inclusion criteria of this systematic review, specifically distinguishing between articles with a main focus on patient participation in care and those where participation was only highlighted as a conclusion. This assessment was conducted by all authors to maintain the research question relevance. Perspectives from patients, staff and both were categorized in three groups using descriptive codes. These codes were critically revised again by all authors, creating subthemes describing the data in a broader sense, focusing on its meaning. This process involved comprehensive examination and evaluation of the extracted information to ensure its accuracy and relevance. Subthemes with similar content were merged and revised to ensure that research questions were appropriately addressed. The subthemes were related to each other in creating the overarching themes. Subthemes and themes were discussed by all authors.
Deductive stage
A deductive approach was employed in coding and theme development. All data were presented under predefined themes, using three of four European standard for patient involvement (2020) concepts as a framework, as shown in Figure 3. The fourth category, ‘Patient and public involvement in management, organization, and decision-making in policy making,' was excluded from our deductive analysis as our systematic review specifically targeted factors influencing patient participation in clinical practice. Consequently, we limited the incorporation of categories in our analysis presentation to concepts aligned with this focus. Results from the three groups (patients, staff, both) were combined (Bettany-Saltikov & McSherry, 2016). This combined approach incorporates both deductive and inductive elements and ensured a comprehensive analysis of patient participation in the inpatient forensic psychiatric care context.
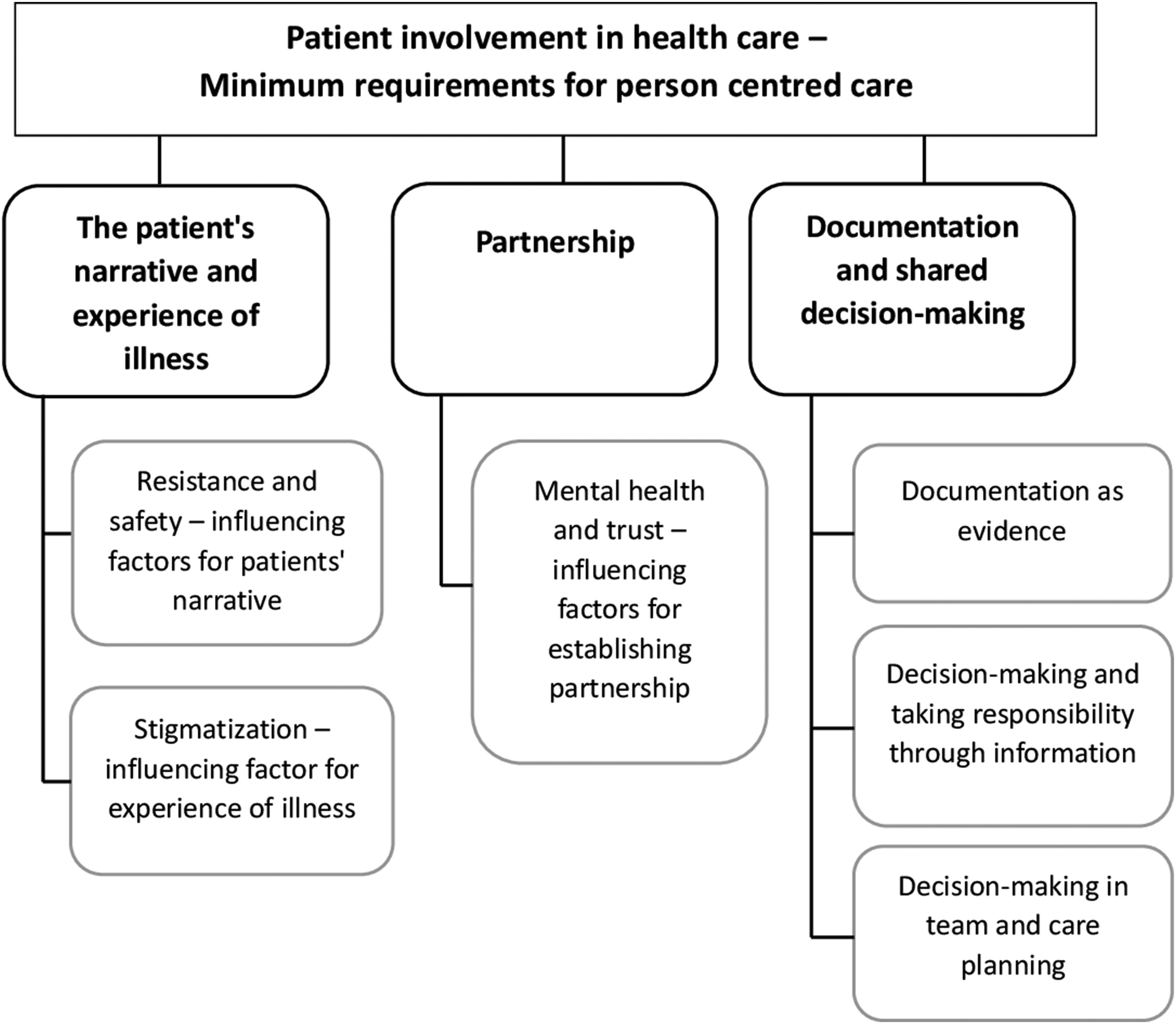
Concepts from the European standard for patient involvement (2020) and subthemes from the analysis.
Results
Study characteristics
Primary studies with qualitative (n = 8), quantitative (n = 1) and mixed-method (n = 1) designs were identified. Most studies were conducted in Sweden (n = 6) and investigated patient participation (n = 7) or patients’ experience of participation in central aspects of inpatient forensic psychiatric care (n = 3). Studies included 9-114 participants and provided the perspective of patients (n = 4), staff (n = 4) or both (n = 2). Studies were conducted in forensic psychiatric care hospitals with low, medium, or high security levels. Table 2 presents ‘facilitating factors’ and ‘hindering factors’ in each article. This is followed with an overall description of patient participation in inpatient forensic psychiatric care settings, along with the codes and subthemes emerging from the analysis.
Perceptions and understanding of the concept of patient participation in forensic psychiatric care
Patient participation in inpatient forensic psychiatric care was described by staff and patients as important but challenging, due to the limitations of coercive care, the judicial system and severe psychiatric illness (Hauso et al., 2021; Magnusson et al., 2020; Nyman et al., 2022; Selvin et al., 2021; Söderberg et al., 2022). Both staff (Magnusson et al., 2020; Söderberg et al., 2020) and patients (Barnao et al., 2015, Söderberg et al., 2022) highlighted a supportive care relationship as fundamental for participation. Moreover, we found that patients were aware of being in a powerless situation. Institutional and legal aspects of forensic psychiatric care, such as the indeterminate duration of coercive care, were highlighted as factors promoting feelings of hopelessness, which also reinforced the perception of forensic psychiatric care as storage rather than care (Nyman et al., 2022; Söderberg et al., 2022). Feelings of not being treated as a human being were reinforced by the perception that activities were not matched to preferences or needs, augmenting the feeling of institutional practices being prioritized over individual needs (Barnao et al., 2015; Söderberg et al., 2022). This affected participation, stigma, and patients’ possibility to make progress (Söderberg et al., 2022).
Staff reported a lack of structure and organizational support for working with participation. Consequently, participation depended on the staff’s willingness to give patients options. These efforts might create a feeling of participation or reduce perceptions of coerciveness but did not actually increase participation in care (Magnusson et al., 2020; Selvin et al., 2021; Söderberg et al., 2020; Söderberg et al., 2022). Some studies highlighted potential factors for enhancing participation, e.g. discussion or dialogue about treatment or assurance that staff understood their mental health status (Hauso et al., 2021; Nyman et al., 2022; Selvin et al., 2016; Söderberg et al., 2022).
Factors influencing patient participation in forensic psychiatric care
The identified themes are presented in accordance with three concepts from the European standard for patient involvement (Figure 3).
The patient´s narrative and experience of illness
Resistance and safety – Influencing factors for patient narratives
Regarding patient narratives, the initial forensic psychiatric care admission phase appeared to be particularly hindering. Being committed to forensic psychiatric care was described as a period of resistance, trying to adjust to a vulnerable position where staff are omnipotent and to an environment where rules are perceived as punishments (Barnao et al., 2015; Livingston et al., 2013; Nyman et al., 2022; Söderberg et al., 2022). Misuse of power and unfair or inconsistent treatment created mistrust and distance between patients and staff, affecting how patient narratives were shared. Patients withheld information about themselves and avoided initiating relationships with staff (Livingston et al., 2013; Nyman et al., 2022; Söderberg et al., 2022). We found that safety was a facilitating factor, as sharing one’s narrative requires feeling physically and emotionally comfortable (European Committee for Standardization, 2020). In interviews, patients reported limited space to express their own opinions or to intervene in unfair situations, as this might threaten their own safety (Nyman et al., 2022). Patients reported feeling safe and having opportunities to express their needs as factors facilitating participation (Söderberg et al., 2022). The connection between participation and feeling safe was further noted by Livingston et al. (2012) where patients believing that their choices were valued and respected were more inclined to feel safe.
Stigmatization – Influencing factor for experiences of mental illness
We found that patients’ experiences of mental illness were connected to stigmatization. Patients described focus on illness and on their negative characteristics, instead of on the current risk of reoffending and on their strengths, as barriers to them being regarded as persons in addition to the “forensic patient” label. This hindered participation by establishing an “us and them” environment (Barnao et al., 2015; Livingston et al., 2013; Nyman et al., 2022). Being a forensic psychiatric care patient was associated with being regarded as dangerous and sentenced “for life”, which affected patients’ hopes for the future, recovery and motivation to participate in their care (Hauso et al., 2021; Nyman et al., 2022; Selvin et al., 2016). The mixed-method study found that patients with a high rate of internalized stigma, and who identified as unworthy, dangerous, and lacking positive self-perception, regarded themselves as incompetent to make decisions and distrusted their own capacity to change to a greater extent than others (Livingston et al., 2012).
In one study, participation was reportedly affected by staff (nurses’) preferences and the extent to which they perceived patients as difficult or high-risk, rather than by the patients’ index crime. In clinical practice, staff avoided contact and wielded power unnecessarily, which hindered participation (Magnusson et al., 2020).
Partnership
Mental health and trust – Influencing factors for partnership
Most studies highlighted a supportive care relationship as a fundamental facilitator for participation (Barnao et al., 2015; Livingston et al., 2013; Magnusson et al., 2020; Nyman et al., 2022; Selvin et al., 2016; Söderberg et al., 2020; Söderberg et al., 2022). We found that patients described their motivation to participate in the care process as closely connected to the quality of this relationship and their mental health status (Nyman et al., 2022; Selvin et al., 2016; Söderberg et al., 2020). In two interview studies by Selvin et al. (2016, 2021), staff and patients reported impaired mental health at the beginning of care as a factor that decreased participation. When mental health status improved, motivation and ability to participate in care increased and patients consequently sought something in which to participate. Furthermore, the mixed-method study found that patients experiencing a supportive care relationship also performed better in self-empowerment and basic functioning (Livingston et al., 2012). These quantitative results concurred with several qualitative interview studies, with patients describing staff’s active and genuine engagement as a prerequisite for encouraging patient responsibility and participation (Livingston et al., 2013; Nyman et al., 2022; Selvin et al., 2016, 2021; Söderberg et al., 2022). Staff and patients had the same view, mentioning that interactions outside the ward environment, such as communal areas in the inpatient facility or escorted leave, played a crucial role in building trust and understanding on more equal terms. These interactions enabled insights into patients’ previous lives, interests, and future dreams (Livingston et al., 2013; Magnusson et al., 2020; Söderberg et al., 2022). Patients stressed the importance of staff encouragement, in order to feel involved and motivated in this partnership (Barnao et al., 2015; Livingston et al., 2013; Magnusson et al., 2020; Nyman et al., 2022; Selvin et al., 2016). The studies report that fluctuation in a patient’s mental health, e. g. being active one day and inactive the next, were additional reasons presented by staff for low participation and failure to establish partnership (Livingston et al., 2013; Magnusson et al., 2020; Selvin et al., 2021).
Trust and honest communication were also identified as key components for a mutual care relationship (Livingston et al., 2013; Söderberg et al., 2020; Söderberg et al., 2022). From the patients’ perspective, fairness, transparency, and accountability were decisive for experiencing trust and thus partnership in the treatment-planning process. However, trust was described as difficult to achieve due to its conditional nature (Barnao et al., 2015; Livingston et al., 2013; Selvin et al., 2016; Söderberg et al., 2020).
Documentation and shared decision-making
Documentation
It was evident that documentation of patients’ everyday lives played significant roles at review board hearings and risk assessments. Documentation could be used as evidence to limit privileges or lead to punishment. It was considered a hindering factor for patients’ willingness to share emotions or reveal thoughts, especially at the beginning of care (Barnao et al., 2015; Livingston et al., 2013; Nyman et al., 2022; Selvin et al., 2016). Patients expressed wanting more insight into their records in order to understand the evidence presented at review board hearings (Livingston et al., 2013). Adjusting the information method to the patients’ needs was a facilitating factor; written information was considered to decrease staff-patient misunderstandings (Livingston et al., 2013; Magnusson et al., 2020; Selvin et al., 2021). Staff highlighted writing case reports with greater transparency, following a standardized disposition, promoting professional working methods, and improving trust and confidence in the system (Livingston et al., 2013; Selvin et al., 2021).
Shared decision-making and taking responsibility through information
Participation in decision-making was defined by patients as being invited to influence decisions. This meant being listened to, having denied requests explained and being invited to conversations about crucial care components such as care plan, risk assessments and review board preparations (Nyman et al., 2022; Selvin et al., 2016; Söderberg et al., 2022). Nonetheless, studies revealed that they felt trapped in a system with non-negotiable areas (Livingston et al., 2013; Nyman et al., 2022; Selvin et al., 2016).
Interviewed staff described feeling responsible to decline patients’ requests, unrealistic goals and even act against the patients’ will, due to their professional knowledge (Magnusson et al., 2020; Selvin et al., 2021). Staff chose to not disclose sensitive, confidential information at all, believing that the patients could not comprehend it. This hindered clear communication (Livingston et al., 2013; Magnusson et al., 2020; Selvin et al., 2021) and affected patients’ understanding of their own situation (Magnusson et al., 2020; Nyman et al., 2022; Söderberg et al., 2022), prerequisites for shared decision-making and taking responsibility.
Taking responsibility was highlighted by patients (Nyman et al., 2022; Selvin et al., 2016; Söderberg et al., 2022) and by staff in Söderberg’s interview study, where staff gradually tried to hold patients accountable for their behavior, attempting to acknowledge that they were capable of taking responsibility (Söderberg et al., 2020). In several studies, patients stated that participation in decisions was dependent on information from staff (Barnao et al., 2015; Livingston et al., 2013; Nyman et al., 2022; Selvin et al., 2016). However, while staff focused on the importance of explaining decisions (Livingston et al., 2013; Selvin et al., 2016), patients expressed wanting to be included in discussions prior to decisions (Selvin et al., 2016; Söderberg et al., 2022).
Decision-making in team and care planning
Several studies found that patients’ experiences of team meetings and care-planning participation included confusion about their role and perceptions of being unable to influence decisions (Barnao et al., 2015; Livingston et al., 2012; Livingston et al., 2013; Nyman et al., 2022; Selvin et al., 2016; Söderberg et al., 2022). Staff and patients wanted to collaborate in tailoring the treatment plan early on and expressed a need for proactive communication in order to feel involved in the care process (Livingston et al., 2013; Magnusson et al., 2020; Selvin et al., 2016, 2021).
Factors hindering shared decision-making were exemplified by routines, commonly inviting patients to only parts of team discussions or requesting that they leave before decisions were made. Being excluded from the whole team meeting resulted in patients feeling left out and thus deprived of the possibility to understand their own care (Livingston et al., 2013; Nyman et al., 2022; Selvin et al., 2016).
Similar findings were reported by Livingston et al. (2012) and Livingston et al. (2013) where limited opportunity to discuss discharge criteria and exclusion from treatment decisions were experienced as factors hindering participation.
Patient characteristics, such as education level, lack of illness insight and unrealistic goals, were factors staff perceived as hindering patient participation (Livingston et al., 2013; Magnusson et al., 2020; Selvin et al., 2021). The perception of the patient as incapable of understanding or making decisions influenced staff’s motivation to engage in shared decision-making (Selvin et al., 2021).
Hauso et al. (2021) measured changes after the implementation of a recovery-oriented practice in medium- and high-security units. They found significant improvements after 12 months of patients’ participation in shared decision-making and in creating care plans. In several studies, patients suggested more frequent team meetings; both staff and patients described feedback on progress as important to facilitate movement through the forensic psychiatric care process and increase patient responsibility (Barnao et al., 2015; Livingston et al., 2013; Nyman et al., 2022; Selvin et al., 2021).
Patients’ views on care-plan participation ranged from feeling like team members with the possibility to give feedback to not knowing that a care plan existed (Barnao et al., 2015; Livingston et al., 2013; Nyman et al., 2022; Selvin et al., 2021).
Discussion
In this systematic review of ten articles, we explored patient participation in inpatient forensic psychiatric care settings. Factors influencing participation appeared to be complex, often intertwined, making categorization such as “hindering” or “facilitating” challenging. Therefore, we organized our findings according to three concepts (Figure 3) aligned with the European standard for patient involvement (European Committee for Standardization, 2020). Several challenges emerged, including the impact of coercive care, the stigma of being an offender with severe psychiatric illness and concerns about safety. We found that staff and patients recognized that participation involved concepts of patient narratives, partnership, and documentation, concurring with practices emphasizing participation, such as person-centered care. Eliciting the patient’s narrative is the foundation for cultivating partnership and the basis for documentation and shared decision-making (European Committee for Standardization, 2020).
We found that patients’ perceptions of their participation varied, ranging from mistrust and resistance to a desire for collaboration and assuming responsibility. These differing perceptions often aligned with the stage in their forensic psychiatric care journey. Trust has previously been described as a prerequisite for eliciting or sharing narratives (Mopuru et al., 2018; Schröder et al., 2016; Livingston et al., 2013; Selvin et al., 2016; Söderberg et al., 2020; Söderberg et al., 2022).
The initial phase of forensic psychiatric care admission is often traumatic for patients. They often display defensiveness, toward staff, the treatment process, or the entire care setting, in reaction to the unfamiliar and potentially intimidating environment. Future research should explore strategies to reduce this initial defensiveness, examining interventions focusing on establishing trust and creating a supportive and safe environment.
Research consistently indicates that patients in forensic psychiatric care who have experienced complex trauma often exhibit disrupted relationships with caregivers and engage in antisocial behavior (Bruce & Laporte, 2015; Stinson et al., 2016; Topitzes et al., 2012). Given the pervasive impact of trauma on mental health symptoms, social skills, and aggression (Bohle & de Vogel, 2017; Bianchini et al., 2022) patient participation is seemingly affected negatively, and collaborative working methods are hampered. This underscores the importance of trauma-informed care in supporting patients’ ability to actively engage in their care. Trauma-informed care that emphasizes trust, partnership, and phases of recovery (Butler et al., 2011), is essential to reinforce patient participation in forensic psychiatric care settings.
This indicates that recognizing patients’ phases in adapting to coercive care and the consequent effects on willingness and/or ability to participate is an important factor for participation in clinical practice. Furthermore, it may be necessary to reframe “eliciting the patient’s narrative” upon initial admission to forensic psychiatric care. For example, nonparticipation can be a problem-solving strategy in the initial, resistance phase, purporting to regain agency in an unsafe environment. Concurring with previous studies of outpatient forensic psychiatric care (Waxell & Wiklund Gustin, 2022), this indicates that participation cannot be separated from coerciveness and control in a forensic psychiatric care setting (Magnusson et al., 2020; Söderberg et al., 2022).
Eliciting patient narratives may also require a focus on supporting patients in adapting to the new environment (Marklund et al., 2020; Olsson et al., 2014; Pelto-Piri et al., 2019). Awareness of the phases in the forensic psychiatric care journey might help staff integrate patients’ shifting needs without eliminating possibilities for participation. Patients’ openness to support from professionals (Waxell & Wiklund Gustin, 2022) has been described as pivotal to initiating partnership.
Stigma, described as the feeling of not being treated as fully human, as well as focusing on patients’ negative characteristics, was identified as a factor hindering partnership. Negative and neglective staff actions were reported to reinforce stigma and contribute to patients feeling dehumanized (Mezey & Eastman, 2009; Entwistle & Watt, 2013). We found that negative emotions concerning patients affected staff interactions and led to avoidance and misuse of power (Magnusson et al., 2020). Jacob and Holmes (2011) argue that disconnectedness becomes an internalized staff response in environments interpreted as dangerous.
The dual-role dilemma of guarding and caring that was highlighted herein as hindering partnership (Livingston et al., 2013; Söderberg et al., 2022), is presented by Jacob and Holmes (2011) as a prerequisite of forensic psychiatric care. Mistrust and constant vigilance are described as inherent parts of the professional relationship in forensic psychiatric care (Jacob & Holmes, 2011).
One proposed solution to overcome the “us and them” dynamic is to facilitate interactions outside the ward, where patients and staff can participate together in activities or discussions that contribute to establishing trust and fostering a more balanced and collaborative relationship. Marshall and Adams (2018) noted that intellectual and physical activities allow relationships within forensic psychiatric care to overcome stigma and power imbalance, emphasizing that these partnerships cannot be examined without recognizing the influence stigma has on building relationships.
Low participation seemed to result from an overall absence of organizational routines that supported patient participation in planning, reviewing, and evaluating the care plan and of patient access to documentation (Magnusson et al., 2020; Söderberg et al., 2020). A previous review in general psychiatry found that staff do not involve patients if they consider them incapable (Jørgensen & Rendtorff, 2018). This finding was echoed in this review (Livingston et al., 2013; Magnusson et al., 2020; Selvin et al., 2021). Furthermore, the perception of the patient as incapable (Selvin et al., 2021), together with perceived security reasons, influenced the staff’s motivation to engage in shared decision-making. Information gatekeeping was identified as an important barrier to documentation and shared decision-making. Previous research highlights the importance of supporting participation, even when patients’ capacity and possibility to affect decisions are limited (Waxell & Wiklund Gustin, 2022). Hauso et al. (2021) demonstrated that the implementation of a recovery-oriented practice in forensic psychiatric care improved patient involvement in care plans and influence in decision-making. This is in line with the findings of Senneseth et al. (2022), who concluded that patient involvement in care discussions was unnecessarily compromised in favor of perceived security.
Marklund et al. (2020) and Hörberg et al. (2012) have previously reported that forensic psychiatric care patients are forced to adapt to the forensic psychiatric care structure and neglect their individuality, in order to gain or keep privileges. Marklund et al. (2020) concluded that a stigmatizing environment affects patients’ motivation to participate, since it diminishes the individual relevance of provided care. Furthermore, honesty and transparency with forensic psychiatric care patients regarding the extent to which choice is possible, have been identified as important (Mezey & Eastman, 2009). This is coherent with our results (Magnusson et al., 2020; Selvin et al., 2016, 2021; Söderberg et al., 2022). Previous literature suggests that neglecting crucial components of participation, while prioritizing structure, routines and security, can impair treatment outcome (Marklund et al., 2020; Mezey & Eastman, 2009; Waxell & Wiklund Gustin, 2022) and safety (Pelto-Piri et al., 2019). To ensure the minimum requirements for patient participation according to the European standard, forensic psychiatric care environments should provide realistic and humanistic opportunities for patients to participate, for instance, in care planning and risk assessment.
Implications for clinical practice
Examining patient participation in forensic psychiatric care reveals both challenges and promising practices. A common theme in the reviewed articles is the significance of trust and partnership in fostering patient participation, aligning with person-centered care principles. This highlights the potential benefit of training programs tailored for forensic psychiatric care, equipping staff with skills for therapeutic alliances and safe environments. Prioritizing supportive care relationships and incorporating patient narratives into policies and organizational structures is essential in order to optimize possibilities for participation (Britten et al., 2020). However, it is essential to recognize that narrative elicitation, a key aspect of person-centered care, requires specific skills and strategies. Incorporating tailored forensic psychiatric care staff training programs that equip professionals with these narrative elicitation skills, might promote therapeutic alliances and create safe environments (Naldemirci et al., 2020). This aligns with the European standard for patient involvement in healthcare for continuous quality improvement in healthcare settings; the document emphasizes patient participation in quality indicator design, implementation and evaluation (European Committee for Standardization, 2020). Additionally, embracing trauma-informed care principles (Butler et al., 2011) and actively involving patients in care planning, risk assessments and decision-making can further integrate patients’ perspectives into their treatment (Söderberg et al., 2023). Söderberg et al. (2023) study on power imbalance in court hearings suggests a need for more transparency and collaboration in decision-making, mirroring the importance of patient involvement in critical elements of forensic psychiatric care. Implementing these practices at the policy, organizational and staff levels may significantly enhance patient participation, improve care outcomes, and support rehabilitation in the forensic psychiatric care system.
Methodological considerations
We followed the guide for systematic literature reviews in nursing authored by Bettany-Saltikov and McSherry (2016). Many studies were excluded due to not being empirical or conducted in an exclusively forensic psychiatric care inpatient setting. We acknowledge that there may be interventions and practices in forensic psychiatric care settings that promote patient participation without explicitly stating this as their primary aim. This review may thus not reflect all aspects of patient participation in inpatient forensic psychiatric care. It is essential to continue examining various practices and interventions to gain a more comprehensive understanding of how patient participation is facilitated and enhanced in these complex healthcare environments. Many studies had methodological limitations, such as small sample sizes or potential selection bias, which should be considered when interpreting our results. The articles generally had high quality-assessment scores, although most lacked ethical considerations, which is particularly noteworthy given that they all concerned coercive care.
Despite these weaknesses, we believe that the knowledge presented here is highly relevant when planning and evaluating models aiming to enhance patient participation in clinical forensic psychiatric care. This review summarizes factors affecting participation, adds knowledge about contextual challenges to improving participation in forensic psychiatric care environments and includes both staff and patient perspectives on participation.
Conclusions
This review presents the challenges and opportunities in relation to patient participation in inpatient forensic psychiatric care settings and highlights the significance of supportive care relationships. It is noteworthy that neither staff nor patients explicitly mentioned any structured forms of participation in critical aspects of the clinical care process. While several studies indicate that increasing patient participation seems appropriate for forensic psychiatric care, more research specifically analyzing implementation of patient participation methods is required to ascertain how these might work in clinical practice.
In summary, possible ways to enhance patient participation without increasing the risk of offending behavior must be explored. More research on perceived safety and actual risk related to patient participation is needed. Compromising essential elements of participation, such as narrative, partnership and documentation, may contribute to keeping patients in passive, unsafe and excluded positions, which might consequently affect discharge planning and care outcomes.