
Abstract
A large proportion of forensic mental health (FMH) inpatients experience cognitive impairments, which may impact the extent to which they benefit from interventions aimed at reducing their risk of recidivism. These impairments should be identified and responded to as quickly and accurately as possible. The current study explored when and how FMH inpatients’ cognition is assessed during their stay at a forensic hospital, with a cognitive profile being constructed of the sample. The medical files of inpatients who resided at the hospital in Melbourne (Australia) during January 2016 and December 2019 were reviewed retrospectively. A total of 99 medical files were identified. The type, timing and results of each cognitive assessment were collected. Frequency analysis revealed more than half of the sample received a cognitive assessment, with most of the cognitive assessments being conducted within the first year of an inpatient’s admission to hospital. Between 19% and 31% of inpatients with available cognitive data demonstrated a global cognitive impairment, depending on the cognitive measure being used. These results highlight the value of assessing FMH inpatients for cognitive impairments to respond to them appropriately to increase their chances of rehabilitation. Careful consideration should be given to the type of cognitive assessment tool used among this demographic.
Introduction
Forensic mental health (FMH) inpatients consist of people who have encountered the criminal justice system and, due to severe mental illness, are being cared for in hospital (Huband et al., 2018; O'Donahoo & Simmonds, 2016). At hospital, inpatients typically undergo various bio-psycho-social treatments to help them successfully return to society without posing an ongoing risk to public safety (termed as rehabilitation; Lloyd et al., 2008; O'Donahoo & Simmonds, 2016). These rehabilitative interventions should address FMH inpatients’ criminogenic needs to reduce their risk, as well as be responsive to their individual characteristics, such as their cognitive abilities (Bonta & Andrews, 2007).
FMH inpatients experience a range of factors that increase their risk of experiencing cognitive impairments, such as head injuries, substance abuse, antipsychotic medication use and/or acute mental illness (Andiné & Bergman, 2019; Jackson, 2011; Justice Health & Forensic Mental Health Network, 2018; Lowings & Wicks, 2012; Ogloff et al., 2004). Evidence indicates that a large proportion of FMH inpatients experience cognitive impairments, which are deficits in mental processes such as attention, processing speed, memory, and executive functioning (Bailie et al., 2012; Flinn et al., 2018; Ireland, 2008; Justice Health & Forensic Mental Health Network, 2018; Lowings et al., 2013; Murphy et al., 2021; Shumlich et al., 2019; Young & Justice, 1998; Zhu et al., 2013). For example, Bailie et al. (2012) reported that among a sample of 260 FMH inpatients, 35.80% experienced a cognitive impairment as indicated by performing two standard deviations below the normative mean on the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS).
It is important to assess and respond to impairments in FMH inpatients’ cognitive capacities to maximize benefit from any treatment and assist with rehabilitation (Brekke et al., 2007; Granholm et al., 2008; Puzzo et al., 2019; Richter et al., 2018). Difficulty in attending to intervention programs may increase disengagement before completion, hence reducing any benefits (Aharonovich et al., 2003; Glassmire et al., 2007). Further, FMH inpatients with cognitive difficulties may struggle to understand, remember, and apply skills taught in treatment programs, hence be less likely to make progress (Abbott et al., 2013; Aharonovich et al., 2003; Glassmire et al., 2007; Ireland, 2008; McKee et al., 1997). This may ultimately contribute to longer hospital stays (Kato et al., 1995; Wint & Hill, 1997). It can be inferred that priority should be given to timely assessment of cognitive functioning in an efficient and thorough manner to ensure impairments are accounted for in effective treatment planning (Andrews et al., 2011).
How and when to assess cognition
Cognitive functioning is typically assessed using a range of standardized assessments, which allows for comparison to normative data. Performance two standard deviations below the norm reflect a cognitive impairment. Both brief assessments (i.e., the use of screening tools) and more comprehensive assessments of cognition can be used to determine FMH inpatients’ cognitive capacity. Brief assessments are typically short in duration, easy to administer and narrow in scope, whereas more comprehensive assessments are multi-dimensional and take longer to administer (Roebuck-Spencer et al., 2017). The use of cognitive assessments in forensic contexts and/or settings is a maturing field of practice. Hence, the construction and validation of these instruments are still in its infancy (Heilbronner, 2004; Serafim et al., 2015).
One study reviewed the use of cognitive assessments at Rampton High Secure Forensic Hospital in the UK (Lowings et al., 2013). Results revealed that the most commonly used cognitive assessment was the Wechsler Adult Intelligence Scale-III (WAIS-III; Lowings et al., 2013). The WAIS, which provides an indication of inpatients’ level of intelligence, may not be assessing characteristics of cognition related to amenability to forensic inpatient treatment. Further, it was not until recently that forensic normative data for the WAIS-IV was published to help improve the accuracy in characterizing FMH inpatients’ cognitive profile (Flinn et al., 2018). It may be that other measures of cognition are more applicable in this context.
Extent of cognitive impairments
Existing research suggests between 15% and 84% of FMH samples have either a specific or generalized cognitive impairment (Bailie et al., 2012; Ireland, 2008; Justice Health & Forensic Mental Health Network, 2018; Lowings et al., 2013; Murphy et al., 2021; Shumlich et al., 2019; Young & Justice, 1998; Zhu et al., 2013). The variability in results may be attributed to the different measures used to assess cognition. Existing studies assessed cognition using measures of either 1) cognitive functioning, which consists of the Wechsler Adult Intelligence Scales (e.g., Wechsler Abbreviated Scale of Intelligence-II [WASI-II], WAIS-III and WAIS-IV; Wechsler, 1997, 2008, 2011) and aim to assess inpatients’ performance on cognitive tasks, or 2) cognitive dysfunction, which consists of the RBANS (Randolph et al., 1998) or Halstead Impairment Index (Matarazzo et al., 1974) and aim to assess inpatients’ level of impairment on cognitive domains. Between 15% and 27% of samples scored within the impaired range on measures of cognitive functioning (Justice Health & Forensic Mental Health Network, 2018; Lowings et al., 2013; Murphy et al. 2021). Whereas, between 36% and 84% of samples scored within the impaired range on measures of cognitive dysfunction (Bailie et al., 2012; Young & Justice, 1998). Overall, whilst this data provides insight into the extent of cognitive impairments present among FMH inpatients, it highlights the difficulty in accurately establishing the proportion of impairment present depending on the type of cognitive measure being used.
Nature of cognitive impairments
When reviewing the existing evidence, it was clear that a proportion of FMH samples scored in the impaired range across all cognitive domains, with particularly poor performance in attention, processing speed, memory and executive functioning (Bailie et al., 2012; Flinn et al., 2018; Mela et al., 2020; Murphy et al., 2021; Viljoen, Iverson, & Brink, 2004). Murphy et al. (2021) reviewed scores from 94 WAIS reports (all versions of the WAIS were included) administered at a secure psychiatric hospital in the UK. Variability within inpatient profiles were noted as indicated by significant discrepancies between composite scores. Similar discrepancies were found by Flinn et al. (2018) among WAIS-IV scores from a sample of 86 FMH inpatients. As concluded by Murphy et al. (2021), these results suggest that FMH inpatients are likely to present with heterogeneous cognitive profiles. This potential heterogeneity highlights that routine cognitive assessment is important to ensure inpatients with impairments are accurately identified and responded to. Further, discrepancies between composite scores most likely highlight the presence of relative cognitive weaknesses and strengths. Knowing inpatients’ relative cognitive strengths and weakness can further help inform treatment planning to optimize benefit from intervention programs.
Clinical practice
Beyond assessment, there is limited data about whether these research findings are reflected in clinical practice. One study conducted by Lowings et al. (2013) reviewed neuropsychological practice at a secure forensic hospital in England. It was concluded that the hospital made a “significant” use of neuropsychological assessments, however, on a “perceived need only basis” instead of being routinely administered (Lowings et al., 2013, p.356, 362). About 63% of the sample received their first neuropsychological assessment within their first year of admission, with a further 15% of the sample assessed within four years of being admitted to the hospital. Lowings et al. (2013) recommended neuropsychological assessments were best administered closer to the time of admission to better inform treatment early in the inpatients’ hospital journey. However, more research is needed to gain an appreciation of the use of cognitive assessments in FMH services to optimize efficacy of practice in these complex settings.
Current study
The current study aims to build on the limited number of existing studies to explore whether cognitive functioning is being considered in clinical practice, in consideration of the importance of identifying and managing cognitive impairments among FMH inpatients. Differences in legislation, diversion practices and health systems mean it cannot be assumed that Lowings et al.’s (2013) findings generalize to Australia. Therefore, gaining a clear understanding of the clinical practice of cognitive assessments in an Australian context is needed to inform ongoing care of FMH inpatients for best outcomes. For example, if a large proportion of FMH inpatients have cognitive impairments, these results can be used to argue for the implementation of cognitive remediation programs during their hospital admission. Similar to the review conducted by Lowings et al. (2013), the current study reviewed the medical files of a secure forensic psychiatric hospital in Melbourne (Australia) to describe the clinical practice around administering cognitive assessments and the outcomes of these assessments.
The following research questions were explored: How, and when, is inpatients’ cognitive functioning assessed at the hospital? What proportion of inpatients experience a cognitive impairment, and what type(s) of cognitive impairment(s) is/are experienced?
Method
Study design and setting
A retrospective audit of Thomas Embling Hospital inpatient electronic medical files was conducted, as approved by the Forensicare Operational Research Committee and the Swinburne University of Technology Human Research Ethics Committee. The requirement for consent was waived by the ethics committees given the impracticality of obtaining consent from inpatients and the low-risk nature of the study.
Thomas Embling Hospital is a 136-bed secure hospital located in Melbourne (Australia) that offers a continuum of reintegration care for people with a severe mental illness who have engaged in significant offending behavior.
Participants
The sample for this audit consisted of forensic inpatients admitted under a custodial supervision order 1 who resided within the hospital between 1 January 2016 and 31 December 2019. Their electronic medical files from admission to Thomas Embling Hospital until discharge or 30 June 2020 were audited. The type of inpatient and the four-year timeframe were chosen to ensure feasible data collection. A total of 101 inpatients were being treated at hospital during the specified timeframe. Two inpatients were removed from the audit as their files could not be accessed at the time of data collection. The total sample consisted of 99 inpatients.
Procedure
Staff at the hospital had indicated that each inpatient should have a Psychological Assessment Report (PAR-90’s), which would contain basic demographic and clinical information along with scores on two brief cognitive assessments, namely the RBANS and WASI. An initial audit tool was constructed on Microsoft Excel in order to gauge how freely available and accessible this information was for each inpatient, as well as how the information was reported in their files. For example, for the cognitive assessment data, the researchers were interested in gauging whether scores were reported for all subscales or not, and whether raw scores or scaled scores were reported. The audit tool captured basic demographic and clinical variables for all inpatients, identified which inpatients had a PAR-90 available, and how many of those reports contained RBANS and/or WASI scores. The initial tool also coded for whether the inpatient was referred for a neuropsychological assessment and whether they received any other cognitive assessments throughout their stay at the hospital.
The first author completed the audit. A pilot for the initial tool was conducted on 20 inpatients included in the study. Another researcher conducted the same audit on five of the initial 20 inpatients to ensure reliable data collection. The same data were found as the first author. The tool was modified at this stage. For example, the Neuropsychiatry Unit Cognition Screening Tool (NUCOG; Walterfang et al., 2003) was administered among a significant number of inpatients, hence record of this measure was added to the audit tool. Additionally, results from more comprehensive neuropsychological assessments were also added to increase the amount of relevant data included in the results. Once the tool had been amended, the complete audit was conducted for the 99 inpatients present in the sample. An outline of the final audit tool can be viewed in the supplementary material. Where necessary, inpatients’ hardcopy files were also audited (e.g., inpatients with files predating the introduction of an electronic filing system).
Variables and measures
Basic demographic and clinical data were included in the audit, which consisted of inpatients’ admission and discharge date (if applicable), their age at admission, sex, education, ethnicity, initial primary and secondary diagnoses, medication within the first year of admission, nature of their index offense, nature of prior convictions (if applicable), history of substance use, and evidence of neurological risk factors (i.e., prior head traumas, neurodevelopmental and/or neurogenerative disorder diagnosis, prior concussions, and/or prior loss of consciousness).
Table 1 above outlines the main cognitive assessments coded for in the audit. The amount, type, timing, and results of these cognitive assessments were noted for relevant inpatients. Additionally, the amount, timing, reason, and outcome of the neuropsychology referrals were noted. Inpatients’ relative cognitive strengths and weaknesses (i.e., relative to their own overall cognitive functioning), and cognitive deficits were identified from their neuropsychological assessment reports.
Outline of the main cognitive assessments included in the audit.
Note. WASI = Wechsler Abbreviated Scale of Intelligence. RBANS = Repeatable Battery for the Assessment of Neuropsychological Status Update. NUCOG = Neuropsychiatry Unit Cognitive Screening Tool.
The cutoff scores represent 2 standard deviations below normative means.
Statistical analysis plan
As in any study accessing existing clinical data, operationalizing the variables depended on the quality and quantity of data available. Some data, especially global cognitive scores from the WAIS, WASI, and RBANS, were reported inconsistently among staff members (e.g., some reported raw scores, some reported ranges and others reported qualitative descriptors), and unfortunately raw scores for these assessments were not always recorded. Hence, it was decided to convert cognition data to qualitative categories based on the Weschler classification system (e.g., ‘extremely low’ [summary score below 70], ‘borderline’ [70-80], ‘low average’ [80-90], average [90-110], and ‘high average’ [110-120]) to optimize sample size. This limited the statistical analysis that could be conducted with sufficient power, hence the study focused on describing the clinical practice and cognitive profiles of FMH inpatients. This was achieved via frequency analysis of relevant variables, as described below.
Results
The total sample consisted of 99 inpatients aged between 20 and 72 (M = 37.08, SD = 11.23) with admissions up to 22 years (Median = 6, IQR = 8). Table 2 summarizes the demographic and clinical characteristics of the total sample. Almost all inpatients had a violent index offense (98% of sample) and a Schizophrenia Spectrum Disorder diagnosis (96%). Almost all inpatients’ files mentioned some form of drug and alcohol use as reported in a psychological assessment or indicated in a risk assessment (82%). The extend of this drug and alcohol use was difficult to determine for all inpatients given the nature of reports. However, 35% of the sample had a substance-related diagnosis, indicating significant drug and alcohol use at some point in their lives. Further, a large proportion of the sample was administered antipsychotic medication within the first year of admission (50%) and had evidence of neurological risk factors (38%).
Total sample (n = 99) demographic and clinical characteristics.
Note. *n = 38 participants who had evidence of neurological risk factors. Some of those participants had multiple risk factors present.
ABI = Acquired Brain Injury, TBI = Traumatic Brain Injury.
Research Question 1: How, and when, is inpatients’ cognitive functioning assessed at the hospital?
A frequency analysis was conducted to determine how and when inpatients’ cognition was assessed. Results revealed that 75 inpatients (76% of the total sample) received a cognitive assessment. At the time, the hospital aimed to assess each inpatients’ cognition briefly within the first 90-days of admission via both the RBANS and the WASI. These assessments are administered by a provisional or registered psychologist. Of the 75 inpatients with a cognitive assessment, 39 (52%) only received a brief cognitive assessment, 2 and 9 (12%) received a more comprehensive cognitive assessment. 3 Twenty-seven inpatients (36% of the 75 inpatients with a cognitive assessment) received both a brief and more comprehensive cognitive assessment. Reasons for a more comprehensive cognitive assessments by a neuropsychologist were based on functional and/or other difficulties experienced by inpatients as observed by their treating team, self-reported or family-reported cognitive difficulties experienced by inpatients, or in some cases based on results from the brief cognitive assessment. It should be noted that not all inpatients who had a cognitive impairment necessarily received a more comprehensive assessment.
Twenty-four inpatients (24% of the total sample) did not receive a cognitive assessment. Reasons for this were explored retrospectively through examination of relevant case notes, admission reports, and/or staff members. Reasons included: inpatient declined assessment (six inpatients), unstable mood/symptoms (five inpatients), inpatient referred for comprehensive assessment instead (three inpatients), inpatient disengaged/resisted (two inpatients), and inpatient has limited English proficiency (two inpatients). For six inpatients no reason for the lack of cognitive assessment was specified in the available data.
Of those with an assessment recorded, the instances of cognitive assessments during their admission ranged between one and seven. The number of measures administered to inpatients ranged between one and 37. Results of the audit revealed that across the sample, 56 different measures of cognition were administered to inpatients, 4 with the most commonly used assessments being the RBANS and WAIS (each was administered to 41 inpatients). Of the 75 inpatients with cognitive assessment data available, a total of 41 inpatients (55%) received their first cognitive assessment within their first year of admission, nine inpatients (12%) were first assessed in their second year of admission, three inpatients (4%) in their third year of admission, five inpatients (7%) in their fourth year of admission, and the remaining of inpatients (20%) between their fifth and eleventh year of admission.
Research Question 2: What proportion of inpatients experienced a cognitive impairment, and what type(s) of cognitive impairment(s) is/are experienced?
Frequency analyses were conducted using the 75 inpatients who received a cognitive assessment to gain insight into the extent and nature of cognitive impairments experienced. Of the 75 inpatients who received a cognitive assessment, 72 inpatients had a global cognitive functioning score, which was extracted from either their RBANS, WASI, WAIS, and/or NUCOG scores. Inpatients were considered to have a cognitive impairment when their RBANS, WAIS and/or WASI total scores fell below 70, and/or when their NUCOG total score fell below 80. Considering RBANS, WAIS and WASI scores, global functioning scores ranged between ‘extremely low’ (i.e., total score below 70) to ‘high average’ (i.e., total score between 110 and 119).
A total of 28 inpatients had two cognitive assessments administered in close proximity (i.e., less than three months between assessments) reflecting the hospital’s protocol of assessing inpatients using both the RBANS and WASI within 90 days of admission. Ten of these inpatients (36% of the 28 inpatients who had two cognitive assessments) scored within the impaired range on one assessment and not the other. The results of the two assessments could not be meaningfully averaged as the measures have different purposes. To account for this discrepancy, the proportion of inpatients with a global cognitive impairment were calculated using both the highest and lowest cognitive assessment scores for those with two recorded scores at admission. When the lowest scores were used, 22 inpatients (31% of the 72 inpatients with a global cognitive score) scored within the impaired range on their first recorded cognitive assessment. When using the highest scoring cognitive assessment results for those with two assessments recorded at admission, 14 inpatients (19% of the 72 inpatients with a global cognitive score) scored within the impaired range on their first recorded cognitive assessment.
Results from some of the most commonly used cognitive assessments and inpatients’ available neuropsychological reports were used to gain a greater insight into the nature of cognitive impairments experienced among this sample. Table 3 outlines the proportion of inpatients who scored within the impaired range on the RBANS, WASI, WAIS, NUCOG, and MMSE. As shown, between 19% and 46% of measures were scored within the impaired range depending on the measure used. While impairments were noted across all cognitive domains assessed across the sample, inpatients were most likely to be impaired in higher-order cognitive domains, such as memory and executive functioning.
Frequency and proportion of assessments scored in the impaired range.
Note. The total number of assessments consists of the number of inpatients who had the appropriate cognitive raw scores available for this analysis to occur.
No further analysis or interpretation of the NUCOG and MMSE will occur as these results do not contribute unique findings beyond those that the RBANS and the WAIS/WASI results provide.
Forty inpatients (53% of the 75 inpatients with assessments) were identified with a more comprehensive assessment recorded in an available neuropsychological report. Figure 1 below outlines the proportion of reports that noted a relative cognitive strength, weakness and/or deficit in the following cognitive domains: attention, processing speed, verbal abilities, non-verbal abilities, memory/learning, and executive functioning. Similar to Table 3, Figure 1 demonstrates that of the cognitive domains noted in neuropsychological reports, inpatients were most likely to be impaired on memory/learning and executive functioning. Inpatients were less likely to experience difficulty in verbal and non-verbal abilities. A small percentage of the sample demonstrated relative strengths across all cognitive domains.
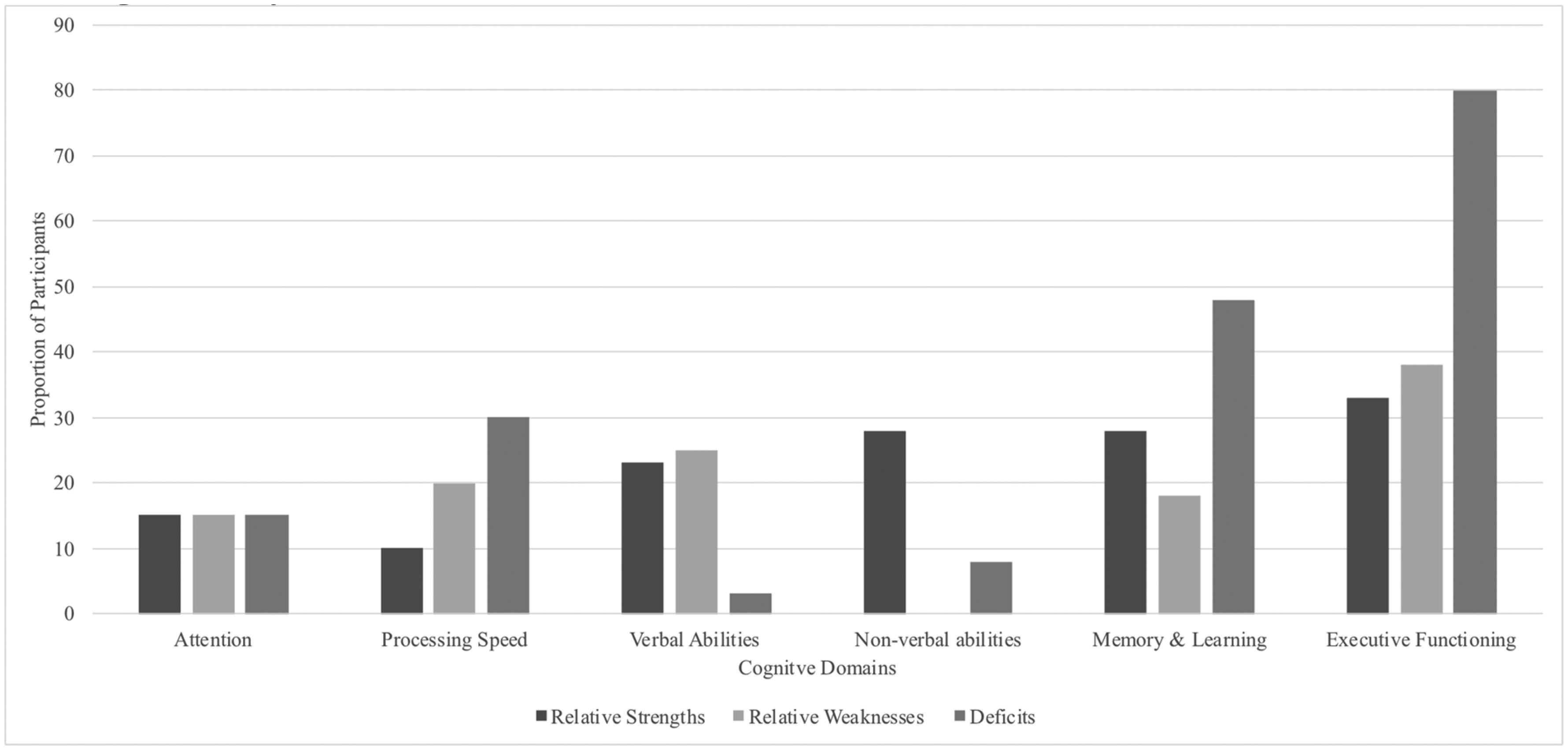
Proportion of sample (n = 40) with an indicated relative cognitive strength and weakness, and cognitive deficit.
Discussion
A retrospective audit of a secure psychiatric hospital’s inpatient medical files was conducted with the aim to describe the frequency and outcomes in regards to the administration of cognitive assessments. Results from this study revealed that three quarters of the sample received a cognitive assessment, with most of these assessments being conducted within the first year of an inpatient’s admission to hospital. Cognition was most commonly assessed using the RBANS and WAIS. Between 19% − 31% of inpatients with available cognitive data demonstrated a global cognitive impairment, with the most common impairments seen in memory and executive functioning.
How and when is cognition assessed
For most inpatients, cognitive functioning was assessed at some point during their stay at hospital. The number and type of cognitive assessments administered to inpatients varied. This is most likely dependent on the clinical presentation and needs of the inpatient, and purpose of the assessment. For example, reasons documented for assessments in neuropsychological reports included to establish a baseline of cognitive functioning, to monitor cognitive functioning, as well as to understand inpatient’s specific difficulties as reported by staff (e.g., impulse control, executive functioning, memory). Assessments were also conducted to inform risk assessments, or were completed in the context of inpatients wanting to complete further education programs. Cognition was most commonly assessed via brief cognitive measures, and typically occurred within the first year of an inpatients’ admission to hospital. However, similar to the findings of Lowings et al. (2013), the current study demonstrated that there was at least a one-year delay in assessing about 40% of inpatients, even though the hospital aims to briefly assess all inpatients within 90-days of admission. These results highlight the practical barriers present among FMH services preventing the implementation of policies (i.e., to routinely assess cognition upon admission) to be translated into clinical practice. Reported barriers in the current study included poor engagement and mental state. This aligns with prior research suggesting complex mental health profiles of FMH inpatients can overshadow and take precedence over assessing cognition (Bailie et al., 2012).
Extent of cognitive impairments
The extent of global cognitive impairments varied among inpatients. This variability may be underpinned by the discrepancies in rates of impairments found between the different assessment types. For example, nearly half of the RBANS assessments administered at the hospital were scored within the impaired range. This was considerably higher compared to the WASI, for which only 15% of assessments were scored within the impaired range. A total of 28 inpatients had both the RBANS and WASI administered within a three-month period. A greater number of the inpatients were impaired when assessed with the RBANS than when assessed with the WASI.
The results of this study align with existing research. Gold et al. (1999) compared scores on the RBANS and WAIS (the WASI is an abbreviated measure of the WAIS) among 129 inpatients and outpatients with Schizophrenia. Results revealed that patients consistently scored lower on the RBANS compared to the WAIS-III (Gold et al., 1999). Focusing on forensic samples, Bailie et al. (2012) found that approximately 36% of an American sample of 260 FMH inpatients were impaired when assessed using the RBANS, yet research focusing on WAIS findings demonstrated that approximately 15% − 17% of FMH patients scored within the impaired range (Lowings et al., 2013; Murphy et al., 2021).
Theoretically these discrepancies are expected considering the aim of the cognitive measures being used. As mentioned before, the WASI aims to measure cognitive performance, hence may be less sensitive at identifying the types of cognitive impairments relevant to the treatment of FMH inpatients, compared to the RBANS which was designed to identify cognitive impairments (Gold et al., 1999). The RBANS may arguably have more utility for this demographic when considering treatment planning, risk and responsivity.
Nature of cognitive impairments
The current sample’s global functioning scores ranged widely between ‘extremely low’ and ‘high average.’ A range in global cognitive scores was also found by Flinn et al. (2018) and Murphy et al. (2021), indicating similar heterogeneity in cognitive profiles among FMH inpatients in the current study. Inpatients in the Murphy et al. (2021) study was also more likely to experience impairments in higher-order cognitive domains, such as memory and executive functioning. These results also support Mela et al.’s (2020) findings which demonstrated that forensic psychiatric outpatients performed poorly on measures of executive functioning and visual memory.
Implications for clinical practice
The results from this study have clinical implications for how and when cognition is assessed, and how to respond to the results of these assessments. Different cognitive measures are assessing differing constructs (functional impairment versus performance) and result in varying levels of cognitive impairments being identified. It is important that FMH services thoughtfully consider the type of cognitive measures they use to screen inpatients upon admission. Consideration should be given to the clinical utility and sensitivity of the assessment. It is argued that measures of cognitive dysfunction will be more sensitive, reliable, and valid to use among FMH inpatients compared to using measures of cognitive performance to better understand their capacity for responsivity to future interventions. This may prevent inpatients labeled as cognitively intact by the WASI from being overlooked for necessary support to engage with interventions.
Various brief measures of cognitive dysfunction may be appropriate to use. For example, the RBANS has been used among FMH inpatients (Bailie et al., 2012). The MATRICS Consensus Cognitive Battery (Nuechterlein et al., 2008) or the Brief Assessment of Cognition for Schizophrenia (BACS; Keefe et al., 2004) may also be used considering the large proportion of FMH inpatients diagnosed with Schizophrenia. It should be noted that the authors do not wish to undermine the usefulness of the WASI among this demographic, however, when resources are limited in FMH services, it is argued that an assessment of cognitive dysfunction be prioritized early in treatment planning. Clinicians should exercise clinical judgment in deciding which assessment to utilize.
The heterogeneity present among the current sample suggests that it cannot be assumed that FMH inpatients’ share a similar cognitive profile. This highlights the need for routine cognitive assessments to help determine inpatients’ cognitive impairments, strengths, and weaknesses. In turn, addressing cognitive impairments in treatment planning early in admission may arguably provide the best chances of inpatient rehabilitation. For example, this sample’s deficits in memory and executive functioning suggest that they may struggle to remember and apply skills and strategies taught to them through intervention programs aimed at mitigating their risk to society. Successful treatment requires clinicians to compensate for these impairments. Adapting existing interventions to account for these deficits, as opposed to interpreting lack of progress to deficits in motivation, is likely to improve the persistence of staff, and reduce negative appraisal.
Various approaches have been evidenced for how to best tailor psychological treatment based on known cognitive impairments (e.g., see Gallagher, McLeod, & McMillan, 2019 for review). Additionally, increased attention has been given to the use of cognitive remediation therapy among FMH samples to try and improve cognitive functioning (Ahmed et al., 2015; O'Reilly et al., 2019), and therefore improve adherence to and benefit from interventions and programs. Clinicians should also draw on inpatients’ cognitive strengths when adapting interventions and programs. The current results suggested that FMH inpatients were not likely to experience difficulties in non-verbal abilities, hence visual aids could be used to help facilitate engagement in treatment programs.
Strengths and limitations
The results of the current study should be viewed in light of its design. A retrospective review of medical files allowed for the investigation of real-life practice at a secure psychiatric hospital with a relatively representative sample of Victorian FMH inpatients. Valuable insights have been gained in terms of the clinical use of cognitive assessments and the cognitive profile of this sample. However, the study is not without its limitations. The retrospective design relied on measures routinely administered by the hospital and the data that could be found in the medical files. Hence, the design decreased the quality and quantity of data, which limited the statistical analyses that could be conducted. For example, covariates (e.g., comorbidities, length of stay, medication use) were not controlled for. To ensure feasibility, the design also focused on certain reports (e.g., admission assessment report) to gain information. It may be that some cognitive assessments (or other information) were not captured in the current study due to human error in reporting, filing, and retrieving relevant data, creating a potential under- or over-representation of cognitive impairments among this demographic. Consequently, caution should be exercised when interpreting and generalizing the current results.
Future research
Notwithstanding the limitations, the current results highlight an important area for future research. Variability in methodology and cognitive assessments used across literature makes it difficult to compare findings. In order to further argue for the need to assess and address cognitive impairments among FMH inpatients, there is a need to confirm the extent of the problem through a well-designed and executed prevalence study or meta-analysis. In addition, there is a need for research to identify appropriate cognitive assessments among FMH inpatients. More research is needed to compare and validate commonly used cognitive assessments among FMH samples to determine the most efficient and cost-effective measure for use in clinical practice due the scarcity of resources in forensic settings. It has also been recommended by Flinn et al. (2018) to consider the development and use of forensic normative data for the WAIS if such a measure continues to be used among FMH samples. Such research will help improve how cognitive impairments are identified and responded to among FMH inpatients to inform their rehabilitation to help reduce their risk of recidivism. Given the research progress in compensating for and/or managing cognitive impairments among FMH inpatients, it would be useful for future research to investigate the practical challenges of translating this information into real-world clinical practice and how this can be done in the most effective and efficient way.
Conclusion
In conclusion, more than half of the sample received a cognitive assessment during their stay at hospital, with most of the cognitive assessments being conducted within the first year of an inpatient’s admission. Results revealed that between 19% and 31% of FMH inpatients experienced a global cognitive impairment, with particular poor performance in memory and executive functioning. This highlighted the importance of assessing for cognitive functioning among this demographic as an important responsivity factor. There is a further need to carefully investigate and consider how cognitive functioning can be assessed for in the most efficient and accurate way among FMH inpatients. Gaining this insight may allow for appropriate adaptation to be made to inpatients’ care and treatment aimed at rehabilitating them.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Stuart Lee and thank him for the contributions he made to this study.
1
Inpatients admitted under a Custodial Supervision Order receive compulsory mental health treatment whilst under forensic care.
2
A brief cognitive assessment was operationalised as the use of a cognitive screening tool (e.g., RBANS, WASI, Neuropsychiatric Unit Cognitive Screening Tool [NUCOG; Walterfang et al., 2003], Mini Mental State Exam [MMSE; Folstein, Folstein, & McHugh, ![]() ]) or a standalone measure (e.g., WAIS, Card Sorting Test, etc.)
]) or a standalone measure (e.g., WAIS, Card Sorting Test, etc.)
3
A more comprehensive cognitive assessment was operationalised as the use of two or more cognitive measures (e.g., WAIS and WMS).
4
Some of these measures included cognitive assessment batteries (e.g., WAIS, WMS), as well as subtests of larger cognitive assessment batteries that were used as stand-alone measures (e.g., using only the Stroop test or TMT from the DKEFS battery).
Conflict of interest
The authors have no conflicts of interest to report.