
Abstract
The effect of medium secure care on reoffending is unknown; adequate control groups cannot be identified and exposure to reconviction may be confounded by onward placement and by legal restrictions. Retrospective analysis of convictions for an England and Wales National Cohort of adults discharged from 35 medium secure services during 1997/8. Data were retrieved from the Offenders Index and from each service. Reconviction risk for 711 cases was estimated using Offending Groups Reconviction Scale-2 (OGRS-2). Reconviction (any standard list offense) served as the sole outcome during a uniform six-year follow up. Reconviction outcomes were highest following transfer to prison, reduced by further secure care whilst restriction orders were effective in reducing convictions only in those at high risk. Substantial reductions in reconvictions were observed across the full range of criminogenic risk after control of the above confounding. OGRS-2 proved a useful assay for estimating the effects of secure services on reconvictions. Analysis of more contemporary samples using the current methods and more recent versions of OGRS is warranted.
Introduction
Cost plays a significant part in hindering the development of mental health services in low-income countries (Rathod et al., 2017). It has been argued that mental health services are also under-resourced even in higher income countries (e.g., Australia: Looi & Kisely, 2018). One challenge for mental health services (when trying to command adequate resources) is demonstrating positive outcomes that are important for policymakers and for the general public. In the context of secure forensic mental health services, demonstrating public protection is arguably the most tangible and important outcome of all, but it has proven to be difficult to operationalize in a meaningful way because of multiple confounding.
Very little is known about the impact that secure services have on recidivism and the limited research that is available tends to have been published 10–20 years ago (see Fazel et al., 2016 for review). Evaluating the impact of secure care on recidivism is confounded by a wide range of factors that include discharge destinations (which vary in levels of security, and therefore exposure to risk), levels of post-discharge supervision, and by the absence of appropriate comparator groups. In England and Wales there are several discharge destinations from medium security that include custodial, inpatient and community settings, service users therefore face varying exposure to reoffending risk. Those transferred to prison in England and Wales will probably have poorer reconviction outcomes. Although reported criminogenic effects of prison are small, this supposition is supported by poorer outcomes for people diagnosed with psychosis released from prison rather than mental health care (Igoumenou et al., 2019), by the often-reported criminogenic nature of prisons (Cullen et al., 2011; Duwe & Clark, 2017) and by higher reoffending rates following custodial sentences relative to community penalties (Weatherburn, 2010). There are also legal factors with the potential to confound offending outcomes in secure service users. Standardized methods that take account of patient criminogenic risk characteristics and adjust for post-discharge management factors could potentially provide a uniform method for gauging the effects of services on reconviction that would be flexible to differences over time or between different countries in how patients were managed when they left services.
In England and Wales, restriction orders (MHA Section 41 or 49) are often applied to people discharged from secure care (Jewell et al., 2017; Rutherford & Duggan, 2008) and oblige professionals to continue supervision and monitoring in the community. Provisions that regulate the supervision and/or treatment of service users in the community have been implemented in the USA, Australasia, the UK, several Canadian provinces and several other European countries (Burns et al., 2013). It is reasonable to suppose that bespoke supervision following discharge will reduce the likelihood of further offending and will therefore confound interpretation of reconviction outcomes. Restriction orders have an obvious impact on discharge processes (Coid et al., 2007, 2015; Jeandarme et al., 2016), but their impact on recidivism has not been fully elaborated. Only two well-powered studies have addressed this issue; it has been shown that restriction orders reduced grave offenses (Coid et al., 2007) and ‘any offenses’ (Coid et al., 2015). Restriction orders therefore are effective, but are imposed on the basis of the nature/severity of acute ‘index offenses’ (Andreasson et al., 2014) and may be arbitrary with respect to broader criminogenic risk and needs factors (Bonta & Andrews, 2007), nothing is currently known about how criminogenic need and risk interacts with the effectiveness of restriction orders.
Studies reporting reoffending outcomes following secure care are also been impeded by the absence, or inappropriateness, of control. Studies have tended to compare medium secure service users inappropriately to prisoners (Bengtson et al., 2019; Falla et al., 2000; Fazel et al., 2016; Maden et al., 1999). Studies have also avoided confounding by applying descriptive analysis (e.g., Davies et al., 2007) or by interpreting outcomes in terms of acceptability to policy makers and the public (e.g., Coid et al., 2007). An alternative way to address these problems would be to use statistical methods (e.g., The Offending Groups Reconviction Scale-2: Taylor, 1999) to estimate pre-admission levels of risk as a baseline against which observed reconviction rates can be gauged (see Travers et al., 2013).
The feasibility of using actuarially assessed risk as a control is supported by consistent reports of sound predictive validity for the OGRS-2 (Taylor, 1999) with groups of service users (Coid et al., 2011; Gray et al., 2004). OGRS-2 has not gained traction in secure services because of its actuarial nature, reliance on ‘proxy’ variables, and wide confidence intervals for individual assessment (e.g. Hart & Cooke, 2013). These limitations do not however hinder the potential utility of the OGRS-2 as a comparator for a well-powered group of secure service users.
Re-analysis of datasets is common in the psychiatric literature and the use of a historic database is warranted by precedent (e.g., Coid et al., 2015). The dataset used here has not been exhaustively analyzed and has scope to address some residual and important issues. The following analyses address 2 clinically pertinent questions. Firstly, what was the association between discharge destination and reconviction outcomes? Secondly, were reconviction rates associated with restriction orders and did these effects interact with criminogenic risk? We plan to use the answers to these questions to make adjustments to risk predictions using the OGRS-2 and then compare predicted versus observed rates of reconviction. The resulting method could potentially provide a standard way to evaluate the effects of secure services on reconviction that is sensitive to longitudinal changes in the service user criminogenic characteristics, discharge pathways and post-discharge supervision.
Method
The Cohort
Service users discharged from 35 medium secure services between 01 April 1997 and 31 March 1998 were followed up through the Offenders Index (OI). The cohort and original ethical arrangements were described by Maden et al. (2004). Further ethical approval for the current secondary analysis was secured from our Cardiff School of Sport and Health Sciences Ethics Committee. The analysis for the current study required discharge destinations, Mental Health Act (MHA) status at discharge and complete conviction histories. There were originally 959 cases, 248 were excluded because conviction histories could not be retrieved from the Home Office, leaving 711 (74%) for whom pre-admission OGRS-2 scores could be calculated and post-discharge conviction outcomes were available. Discharge MHA restricted status was available for all 711 cases, but 32 had no recorded discharge destination. The ‘at risk’ period for all started on the recorded day of discharge and ended precisely six years later.
Measures
The risk assessment instrument employed here was the Offending Groups Reconviction Scale − 2 (OGRS-2: Taylor, 1999). OGRS-2 shows superior long-term predictive validity than structured professional judgment tools (Coid et al., 2011). OGRS-2 was validated on an English an Wales sample of adults released from prison contemporaneously with the observation period of the current cohort. Using OGRS-2, rather than more recent iterations of OGRS allowed control of exposure to risk for reconviction during the same period and in the same national criminal justice context as the original OGRS validation sample. The OGRS-2 predicts the probability (0–100%) of conviction for any standard list offense within 2 years of leaving custody, with retained predictive validity over longer periods (four and six years) for people previously treated in medium secure services (Hill, 2020).
Analyses
All analyses were conducted using IBM SPSS Statistics for Windows, version 26. One-way ANOVA was first used to assess whether risk for reconviction was confounded by discharge locations (open conditions, secure care or prison). Chi Squared analyses along with hazard ratios (with 95% confidence intervals) were used to examine the longitudinal relationship between discharge locations and reconvictions. The association between restriction order status and risk for reconviction (OGRS-2) was explored using a 5 × 2 Chi Squared analysis. Further Chi squared analyses explored interactions between risk status and the effects of restriction orders over time (at two years, four years and six years). The final analyses used the Kolmogorov-Smirnov Goodness of Fit Test to contrast expected and observed conviction rates after OGRS-2 scores had been adjusted to account for the effects of time, discharge locations and restriction orders. Alpha for all analyses was set at .05, alpha inflation was controlled throughout using the Holm Bonferroni method (Holm, 1979). Effect sizes for ANOVA are reported for theta squared (η2), whilst those for Chi Squared are reported using Cramer’s V.
Results
Discharge pathways and reconvictions
Mean OGRS-2 scores for different discharge locations (Open conditions = 38.09, Secure services = 39.91, Prison = 39.86) were indistinguishable (F (2, 676) = 0.375, η2,=.001, p = .687). Criminogenic risk (measured using OGRS-2) did not confound interpretation of differences in offending outcomes between discharge pathways.
The top panel of Figure 1 shows conviction rates at two, four and six years cross-tabulated with discharge locations. Reconvictions were most frequent in the group discharged to prison followed by the open conditions group, whilst the group transferred to further secure care had the lowest rate of reconviction. The association between discharge pathway and observed reconviction rates was significant for the two-year (X2 = 11.67, V = .106, p = .003), four-year (X2 = 12.258, V = .108, p = .002) and six-year (X2 = 13.782, V = .115, p = .001) follow up points. Additional analysis showed that remand/convicted status of service users (MHA Section 48 vs 47) remitted to prison was not associated with subsequent reconvictions (2 years, X2 = .144, V = .022, p = .704, ns, 4 years X2 = .306, V = .032, p = .580, ns and 6 years X2 = .696, V = .048, p = .404, ns) . This observation rules out the possibility of increased pseudo-reoffending (delayed convictions for offenses committed by those on remand-status before psychiatric admission) driving the elevated reconviction rates for those transferred to prison.
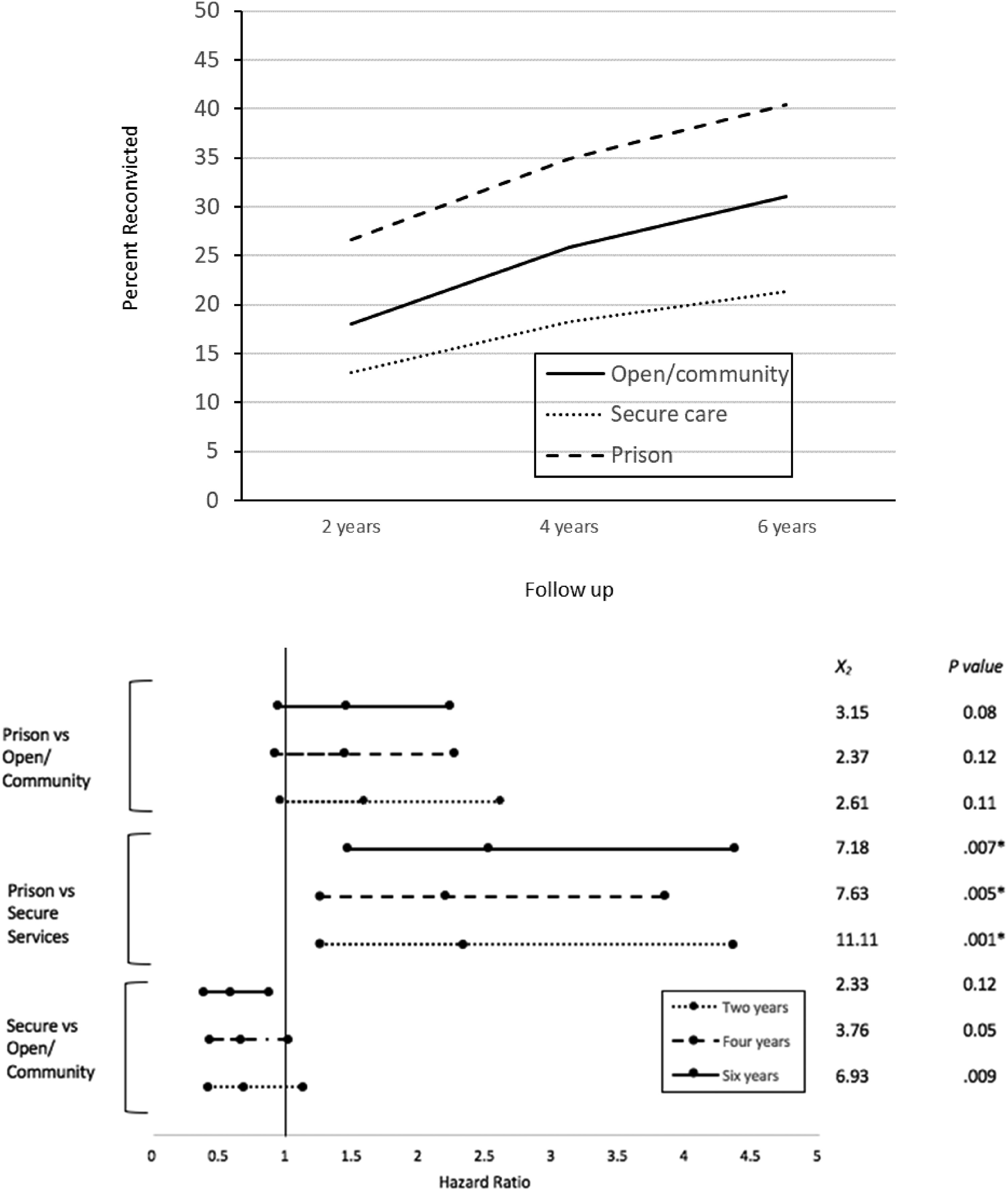
(Upper panel) Cumulative reconviction rates for any and violent offenses for 3 different discharge pathways at 2-, 4- and 6-years follow up points; (Bottom panel) Risk of reconviction across two to six years between each discharge pathway (ratio > 1 shows increased percent of patients reconvicted with first discharge pathway as reference category); * significant associations after alpha adjustment.
Hazard ratios with 95% confidence intervals were calculated to reflect all possible contrasts amongst the discharge pathways at each of the three follow up intervals see bottom panel of Figure 1. Outcomes for service users transferred to prison were significantly worse than those for the service users transferred to further secure care at all follow up points. Reconvictions for those discharged to open conditions were initially (at two years) lower than for those transferred to prison but did not differ significantly thereafter. Reconvictions were generally less frequent in the group transferred to further secure care than for those discharged to open conditions, this difference emerged by the fourth year and continued until the sixth. These analyses confirm that discharge pathways confounded reconviction outcomes; the next analysis will consider whether restriction orders (which are intended to reduce harm following discharge) were similarly confounding.
Restriction orders and reconvictions
There was no association between predicted risk for reconviction (using OGRS-2) and restriction orders, X2 = 3.860, V = .074, p = .425, ns. The imposition of restriction orders was independent of actuarially predicted risk, furthermore the effects of restriction orders on reconviction that are reported next were not confounded by reconviction risk.
The following analysis sought to explore whether reconviction rates were in fact lower for service users who were subject to MHA restriction orders (Section 41 or 49) and whether this effect interacted with risk for reconviction (OGRS-2 status). A series of one-tailed Chi Squared analyses were conducted that contrasted reconviction rates for the restricted versus unrestricted services users within each of the OGRS-2 risk quintile groups. The analyses were applied separately to each of the three follow up points (two, four and six years after discharge). Restriction orders were only associated with reduced reconvictions in the highest (4th & 5th quintile) risk groups, see Figure 2.
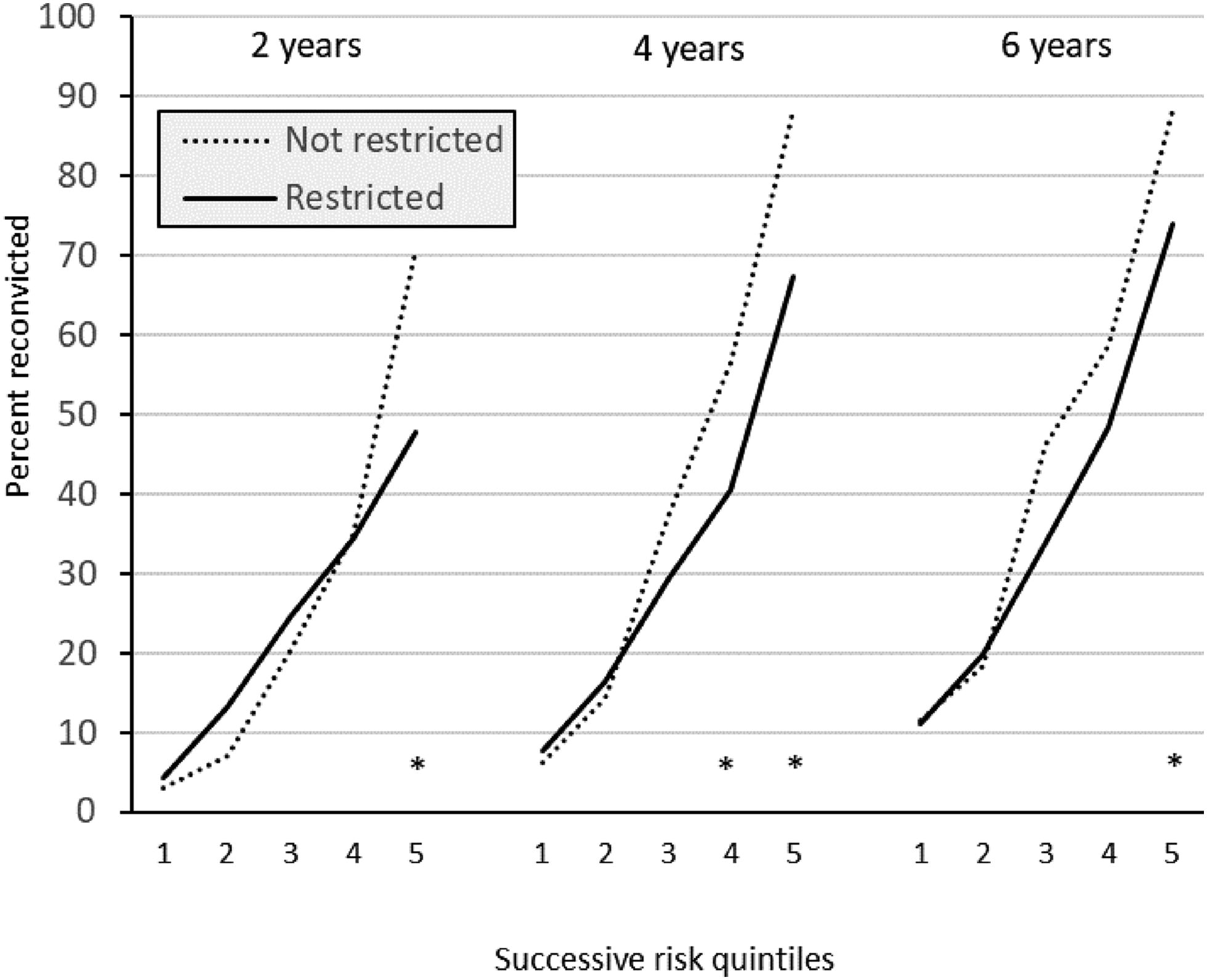
Cumulative percentage of restricted and unrestricted service users convicted for any standard list offense at 2, 4 and 6 year follow up. The cohort were divided into successive OGRS-2 risk quintiles, * p<.05.
Reconviction rates after adjustment for exposure, discharge location and restriction orders
Reconviction rates increased over time and interacted with restriction orders and discharge destinations in complex ways. The final analyses were designed to ‘distil’ the effects of medium secure services by adjusting predicted rates of reconviction (OGRS-2) in light of the effects of three confounds; the effects of discharge pathways, restriction orders and duration of exposure.
Three adjusted OGRS scores were calculated for each service user, one for each of the three follow up points. The first adjustment was for the rate at which the cohort acquired reconvictions over time. No time adjustment was necessary for the two year follow up point (OGRS-2 was designed to predict this outcome). All OGSR-2 scores at the four year follow up were increased by the difference in reconviction rates between the two and four year follow up points (+8.2%), OGRS-2 scores for 6 years were increased by the difference between two and six years (+12.8%).
A second set of adjustments was designed to account for the effects of discharge locations (see Figure 1). Adjustments here used reconviction rates for the group discharged to open conditions as a reference and increased expected rates for those transferred to prison by +8.6% at two years, +9.0% at four years and +9.4% at six years, expected rates for the group transferred to further secure care were lowered (−5.0% at two years, −7.6% at four years and −9.6% at six years).
The final adjustment took account of the observed interaction between risk and restriction orders; restriction orders were associated with lower reconviction rates only in the two groups at highest risk. Consequently, the predicted probability of reconviction was adjusted downward for service users with restriction orders who were in the 4th and 5th OGRS-2 quintile groups (see Figure 2). Adjustments were restricted to instances where statistically significant reductions in reconvictions were observed and reflected the observed difference in reconviction rates between restricted and unrestricted groups. Expected probabilities were reduced by 22.8% at 2 years for the 5th quintile risk group, by 16.0% & 20.8% respectively for the 4th & 5th quintile groups at 4 years and by 14.3% at 6 years for the 5th quintile group (see Figure 2).
Comparison of predicted versus observed reconviction rates was achieved using the one-sample Kolmogorov-Smirnov Goodness of Fit Test; observed reconviction rates were compared to mean adjusted OGRS-2 scores for each of the 5 quintile risk groups at each of the 3 follow up intervals (2, 4 and 6 years). Reconviction rates were lower than expected for all risk groups in the first 2 years, for all but the highest risk group at 4 years and for all except the 3rd quintile group at 6 years follow up (see Figure 3). Reconvictions were significantly fewer than expected across the full range of criminogenic risk. Overall, the current analysis suggested that reconviction rates were 18.5% lower than expected at 2 years, 18.8% lower at 4 years and 19.2% lower at 6 years (see Figure 4).
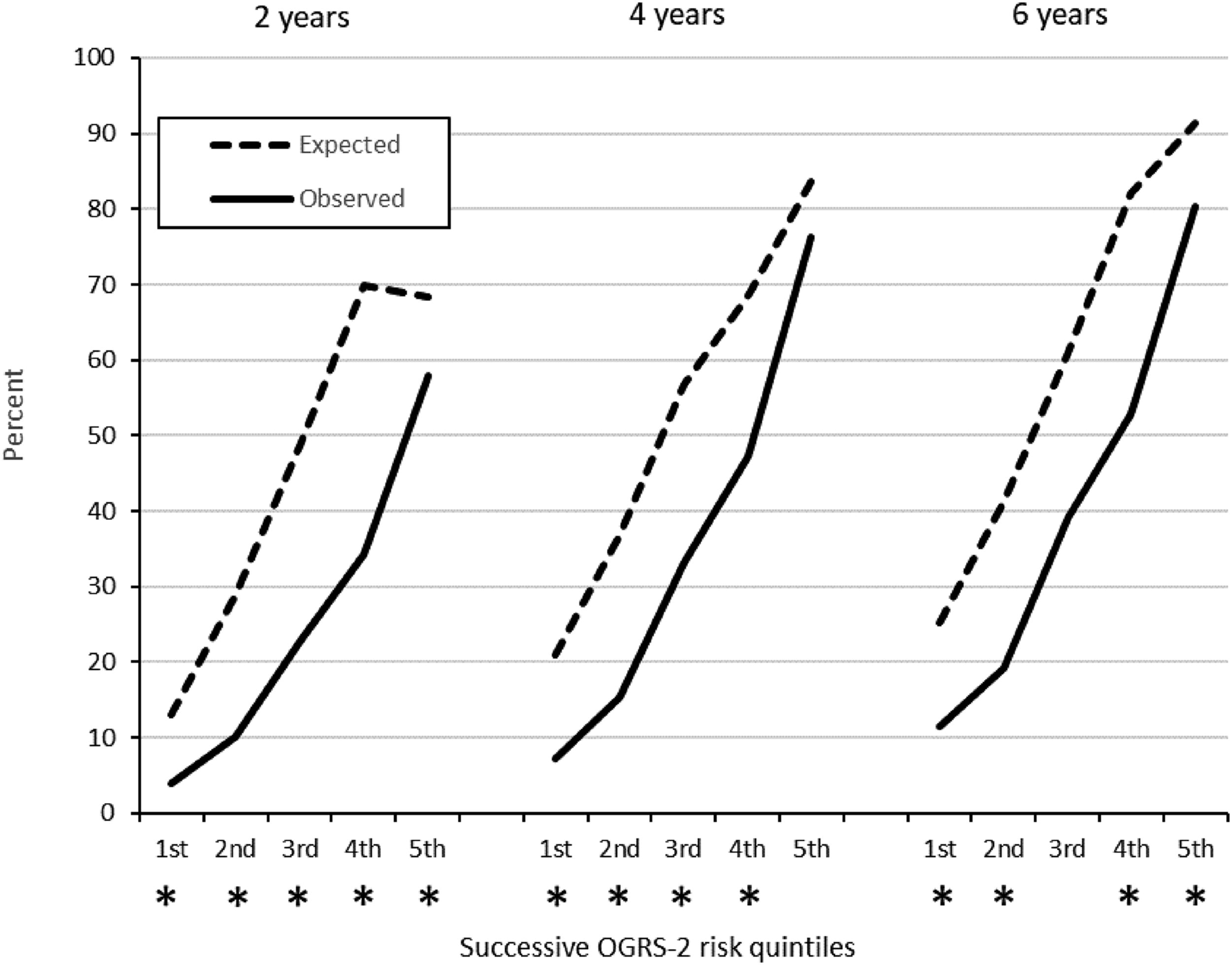
Expected and observed reconviction rates for any offense after adjustment of mean OGRS-2 scores to account for the effects of time, discharge destinations and restriction orders, * p<.05. One sample Kolmogorov-Smirnov test for goodness of fit was used, alpha was adjusted using Holm-Bonferroni method.
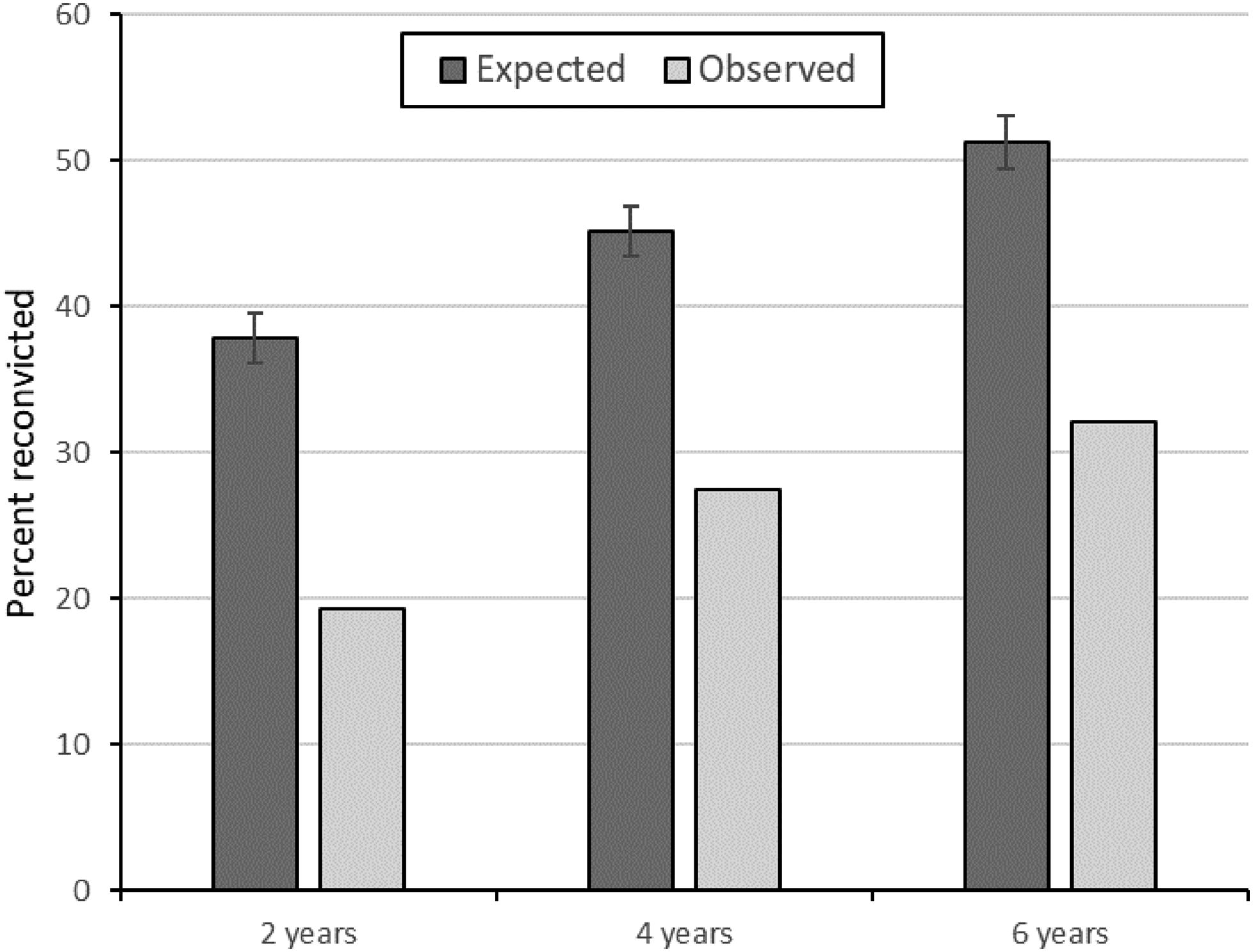
Expected and observed reconviction rates for the whole cohort at 2-, 4- and 6-year follow up. Error bars show 95% confidence intervals for expected reconviction rates.
Discussion
The evidence from this current study suggests that treatment in English and Welsh medium secure services in the late 1990s was highly effective in reducing reconvictions across the full range of criminogenic risk in a national cohort of service users discharged in 1997/8. This study also revealed the size and nature of confounding by two important post-discharge factors (discharge placement and restriction orders). After adjustment, the differences between observed and expected reconviction rates were substantial and sustained (see Figure 4). The methods outlined provide a within-subjects method for circumventing the very difficult task of identifying an acceptable comparison group, this was achieved by using OGSR-2 to estimate reconviction rates that ‘would otherwise have been expected’ and contrasting these with observed rates.
Discharge pathways had a substantial impact on reconviction rates, these were highest amongst those transferred to prison, intermediate in those discharged to open conditions and lowest for service users transferred to further secure care. The size of these differences was stable over time with prison transfers reconvicting 2.5 times more often than those transferred to secure care and 1.5 times more often than people discharged to open conditions, the elevated rates of reconviction are nearly identical to those reported previously for people diagnosed with psychosis and released from prison rather than psychiatric care (Igoumenou et al., 2019). The negative impact of prison transfer on reconvictions was especially worrying as the frequency of remission to prison has doubled over recent decades in the UK (Doyle et al., 2014; Maden et al., 1999, 2006) and has even prompted concern over the effectiveness of schemes designed to divert people from criminal justice into mental health services (Birmingham et al., 2017).
The current study is the first to explore the impact of restriction orders on reconvictions in light of actuarially assessed risk. We found that the application of restriction orders was unrelated to risk for reconviction, we also found that restriction orders were only associated with reduced reconvictions in those at highest risk of reconviction. These findings are consistent with previously reported lack of association between restricted status and patient criminogenic risk (Andreasson et al., 2014) and also with reported reductions in reoffending for both grave (Coid et al., 2007) and any offenses (Coid et al., 2015) in people subject to restriction orders. Our analysis added an additional dimension to this picture by revealing that the effect of restriction orders interacted with preadmission risk. Such potential interactions must be taken into account when factoring in the impact of restriction orders on post-discharge offending.
Secure services in England and Wales are constantly evolving and it could be argued that the current findings may be of mere historical interest. For example, Wales has seen expansion in low secure beds over the last 20 years and medium secure service users have been increasingly discharged into low secure settings (Hill, 2020). However, our findings make a substantial contribution by providing a baseline of reconviction outcomes from early in the evolution of medium secure services, they also show that reconvictions were related to levels of criminogenic risk, discharge pathways and legally mandated supervision in quite complex ways. By adapting estimates of risk to account for post-discharge confounding we offer a method of evaluation that would be adaptable to changes in the use of different discharge destinations and the use of restriction orders (or similar community supervision) over time. We believe that the current method could also be applied to data from service users all over the world, so long as (in each instance) the predictive validity of the OGRS modeling is established as it was here (see this paper’s sister; Hill et al., in press). The main advantage of OGRS modeling of risk for reconviction is that it generates a numeric estimate of reconviction risk, reconviction outcomes can therefore be averaged for groups of service users and it becomes possible to compare the performance of services in different places, at different times and as new policies or services are put in place. Our findings suggest that criminogenic risk is not the only consideration when evaluating reconviction outcomes for secure service users and researchers should also explore the effects of onward placement and mandated supervision to adjust their expectations regarding likely offending outcomes for groups of service users.
Limitations
The most obvious limitation of the current analysis was its reliance on historical data; the cohort left medium secure services in 1997–1998 and the end of the follow up period was 17 years ago. It could be argued that relevance for current services is limited by the 2007 amendments to the Mental Health Act (1983) and/or by the development of new services that have complicated care pathways (Joint Commissioning Panel for Mental Health, 2013). This issue can only be resolved empirically by exploring longitudinal changes in the utilization of different discharge pathways and by exploring their impacts on reoffending.
The absence of differences in OGRS-2 scores for the groups assigned to various discharge pathways negated possible confounding of reconviction outcomes by pre-admission risk for reoffending. It must be acknowledged that this interpretation over-simplified potential interactions between mental illness, risk and reconvictions. For instance, the link between mental illness and risk in those transferred to prison is likely to have been weaker than in those discharged either into the community, or, transferred to further secure care. This possibility is problematic because treatment for mental illness may have less impact on subsequent offending in any group where it is not part of (or is only weakly associated with) the causal pathway of offending behavior. Furthermore, the people discharged into the community will most likely have shown some evidence of reduced risk that made staff confident that they could be discharged safely whilst those transferred to further secure care will have given staff continuing cause for concern. In contrast, those transferred to prison will have been released at the end of their tariff irrespective of whether their perceived risk had decreased. This potential confounding issue could be resolved in the future by interpreting outcomes in light of methods for estimating treatment responses like the DUNDRUM quartet (Adams et al., 2018; Kennedy et al., 2013).
The OGRS model has been through three iterations of updating (OGRS: Copas & Marshall, 1998; OGRS-2: Taylor, 1999; OGRS-3, Howard et al., 2009; OGRS-4, Mavron, 2019) with each revision claiming to have improved the validity of the model. It could be argued that the version of OGRS used here was obsolete. In fact, our choice to use OGRS-2 was a deliberate one and based on both the validation sample and the service user cohort being exposed to potential reconviction in the England and Wales criminal justice system at the same time. Choosing OGRS-2 therefore controlled for potential longitudinal changes in investigative and/or judicial practice. Any subsequent reconviction studies of secure service users should opt for a more recent iteration of the OGRS model to enable contemporaneous outcome evaluation.
Implications and recommendations
The current findings relate to future evaluations of medium secure care and to ongoing changes in forensic mental health practice. Matching groups simultaneously on both mental health and criminogenic risk is not feasible; our recommendation is that future follow up studies of secure services should employ OGRS. Follow up studies of secure service users should also adjust for confounding by discharge locations and legal restrictions.
Poorer outcomes for the service users remitted to prison suggest that this practice may have negated some of the benefits accrued through medium secure care. Increasing use of this discharge pathway is a cause for concern and further work is needed to examine more contemporary outcomes following remission to prison from medium secure care.