
Abstract
This study describes and examines the impact of a novel Reflective Practice program tailored to the multidisciplinary clinical workforce at an inpatient forensic mental health setting. Surveys assessing wellbeing, self-efficacy and reflective practice capacity were administered to all clinical staff prior to commencement of the Reflective Practice program, as well as six months post-implementation. Interviews were also conducted with key clinical stakeholders to obtain detailed feedback regarding the impact of the program across the organization following six-eight months of implementation. Staff who participated in post-implementation surveys reported significantly higher confidence in their work when compared to staff at baseline, while clinical stakeholders observed improvements in the cohesion of the multidisciplinary team. In spite of the limitations of the pragmatic study design and small sample size, results suggest the novel Reflective Practice program offers an acceptable model for adoption in an inpatient forensic mental health setting, with potential to improve the wellbeing, learning and morale of a forensic mental health workforce. The findings also highlight the need to support practice development and wellbeing in early career clinicians, where low confidence and high stress are predominant.
Introduction
Reflective practice is critical and deliberate inquiry into professional practice in order to gain a deeper understanding of oneself, others and the meaning that is shared between individuals (Ruth-Sahd, 2003). The goal is not necessarily to address a specific problem or question but to observe and refine practice in general on an ongoing basis. The process of reflective practice originated as a tool for learning from experience in disciplines such as teaching, social work and medicine (Schon, 1983), where individuals would reflect on their encounters with those they worked with. This process of continuous learning from experience is widely considered beneficial for learning (Boud et al., 1985; Schon, 1983) and is increasingly being adopted in healthcare settings such as palliative care (Gravier et al., 2019; Salins, 2018), emergency departments (Pangh et al., 2019), intensive care nursing (Wharton et al., 2021) and midwifery (Wain, 2019). In these settings the practice is not limited to the discipline of nursing, but also considered important for the professional learning and skill development of medical and allied health professionals (Pawar & Anscombe, 2015; Cohn et al., 2010), particularly early in discipline training (Mann et al., 2009; Ruth-Sahd, 2003).
Background
Research to date that examines uptake of reflective practice has taken place primarily in general health (Wilshaw & Trodden, 2015) and mental health settings (Franza et al., 2015; Mankiewicz, 2014; Thomas & Isobel, 2019). Studies in these settings report that reflective practice was helpful with the development of clinical practice, particularly with analyzing clinical situations from a different perspective, improving clinical competency and increasing level of comfort in the role (Caldwell & Grobbel, 2013; Mankiewicz, 2014; Wilshaw & Trodden, 2015). Clinicians also felt the reflective practice process provided a buffer against the emotional toll of clinical work, by allowing an outlet for discussion of feelings and a better understanding of their experiences (Caldwell & Grobbel, 2013; Rees, 2013). Emerging research further reports that staff working in the inpatient setting describe improvement in self-efficacy following participation in reflective practice (Cigala et al., 2019; McConville et al., 2017; Rahimi & Weisi, 2018) as well as emotional wellbeing and resilience (Caldwell & Grobbel, 2013; Grant & Kinman, 2012).
The adoption of reflective practice in healthcare settings however, occurs in varying degrees and formats (Guy et al., 2020; Thomas & Isobel, 2019). For example, reflective practice can be incorporated within clinical supervision (Guy et al., 2020), delivered as stand-alone group discussions (Baker et al., 2021) or adopted through use of reflective journals (Le et al., 2019). In many existing studies, how the process of reflection occurs is not clearly articulated, with limited information available about the structure or process of reflection, or the frequency at which it occurs (Dube & Ducharme, 2015; Heneghan et al., 2014). There are also few examples of formal programs offering a structured reflective practice process that can be embedded into the routine hospital system (Marshall & Kirkland, 2021). The majority of studies to date are limited by the ill-defined concept of reflective practice and the theoretical framework on which the research is based (Dube & Ducharme, 2015, Heneghan et al., 2014). Research examining uptake of reflective practice is largely qualitative, with few studies assessing for quantitative change in reflective skills and capacity (e.g. Self-appraisal, reflection after action, reflection during action) following engagement in reflective practice (Priddis & Rogers, 2018). Subsequently, there is a dearth of understanding of the effectiveness of reflective practice models to improve reflective capacity and there is little understanding of the relationship that exists between the change in reflective practice capacity with both wellbeing and self-efficacy (Caldwell & Grobbel, 2013; Dube & Ducharme, 2015; Priddis & Rogers, 2018). This is particularly important to assess in the forensic inpatient mental health setting, where concerns have been raised around clinician burnout, compassion fatigue and vicarious trauma (Brown et al., 2017; Marshall & Kirkland, 2021; Pirelli et al., 2020). Clinicians in forensic mental health settings encounter unique ethical challenges to clinicians that are not commonplace in general and mental health settings, as well as more frequent incidents of verbal and physical aggression then observed in mainstream hospitals. (Braham et al., 2008; Oates et al., 2020). As such, it is not appropriate to assume the benefit of reflective practice observed among clinicians in general health and mental health settings will be experienced by clinicians in forensic mental health settings.
Development of the intervention
This study included the development of a Reflective Practice program at the Thomas Embling Hospital (TEH), in Victoria, Australia. A Reflective Practice team was established at the hospital to facilitate the implementation of a suitable Reflective Practice program across all units of the hospital. The team comprised a team of three psychologists, one to design and lead the program implementation and development, and two psychologists to co-facilitate program sessions and contribute to development of wellbeing material. Program funding allowed for monthly external supervision with a Forensic Psychiatrist trained in psychotherapy and professional development.
Program development
The final program introduced at the hospital was developed with reference to several frameworks (Balint, 1985; Gibbs, 1988 and Kolb, 1984) and adapted to meet the needs identified by clinical staff. The Balint model (Balint, 1985), used primarily by psychiatrists and general practitioners, is grounded in psychoanalysis and general practice, with the intention of bringing awareness to aspects of transference, countertransference and the unconscious in the doctor and the patient experience. In a pure Balint group session, one or two doctors are required to briefly and informally present a patient case, including their own feelings and reactions. The discussion is focused on the doctor-patient relationship as well as on the central issue chosen by the doctor for that session. The adaptations to the Balint model enabled space for; 1) staff to reflect on and discuss complex patient issues 2) a small psychoeducational component focusing on psychodynamic concepts.
The changes to the model were made in response to the culture at the Thomas Embling Hospital at the time of program implementation. The culture required for the Balint model required clinicians to make themselves vulnerable and to feel safe in disclosures. Whilst this is often a result of time spent in the reflective process, feedback from staff and interviews with senior stakeholders indicated that the climate at hospital required additional cultural change to support the model in its purest form, particularly the psychological safety of staff to share feelings and experiences amongst their colleagues. Additionally, staff had expressed a need for solution-focused orientation to team discussions and organizational initiatives, due to the long-standing sense of being unable to progress with complex cases or workplace issues and calling for resolution.
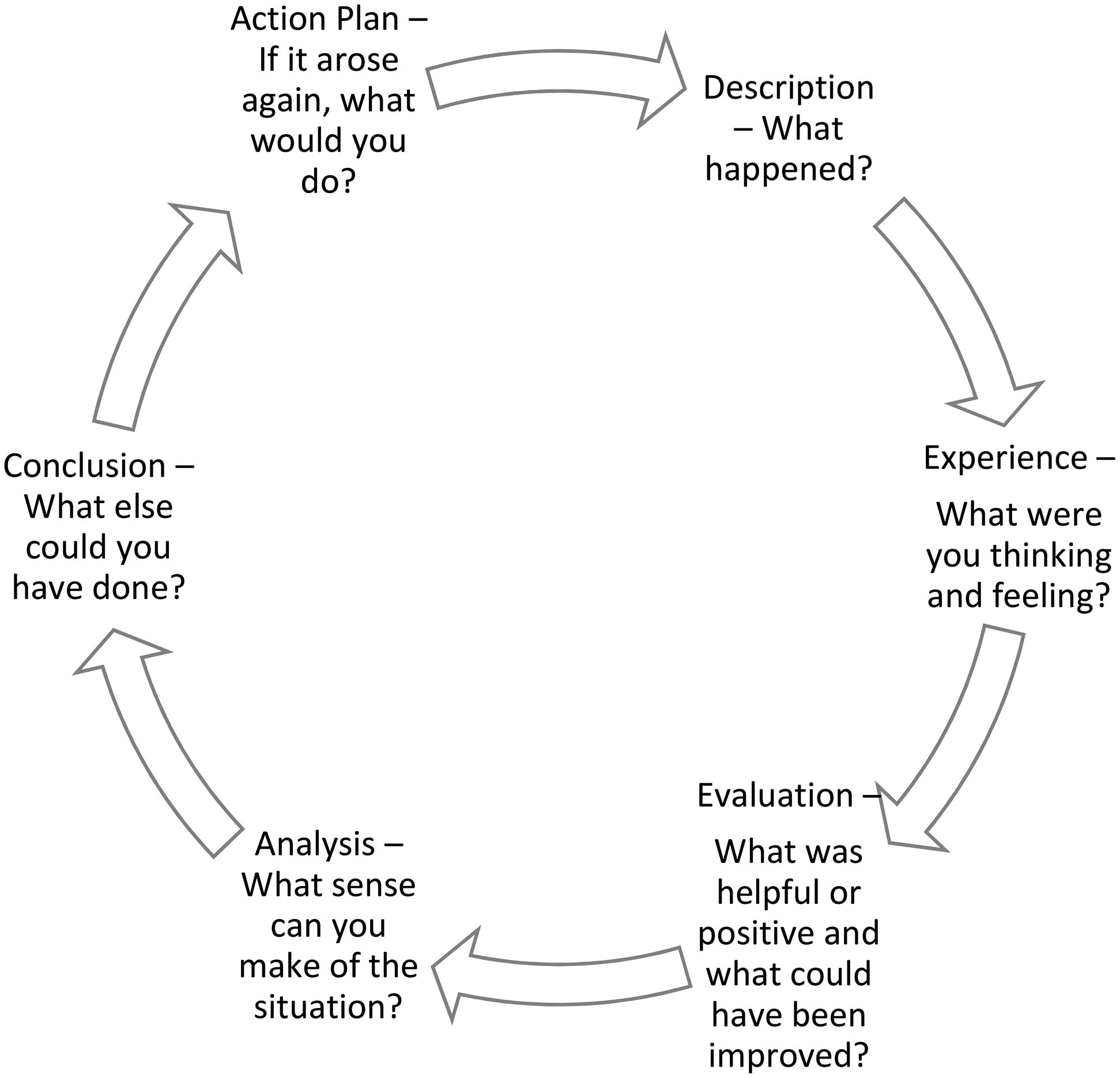
Reflective Practice program facilitators followed a similar reflective cycle structure as proposed by Gibbs (1988) and Kolb (1984) (see Figure 1). In this context, participants were guided through a process of discussing what happened during a specific incident. In the case of a specific patient, the discussion explored what participants’ were thinking and feeling, how this impacted them/their work, what they made of the situation (analysis), what they were left with, and how, after discussion, they now viewed the situation.
The framework underpinning the Reflective Practice program also incorporated the delivery of wellbeing workshops to promote positive psychological strategies (see Figure 2). The inclusion of the complementary wellbeing workshops allowed the reflective practice team to address the immediate need of clinical staff for solution-focused support. Additionally, scheduling issues and operational and budgetary constraints meant that in half of the allocated time available for sessions, only one facilitator was available to deliver the Reflective Practice program. Thus, wellbeing workshops, comprising didactic information and experiential exercises were developed in advance, and delivered by another facilitator to meet both the needs of staff and the operational limitations that existed in the hospital.
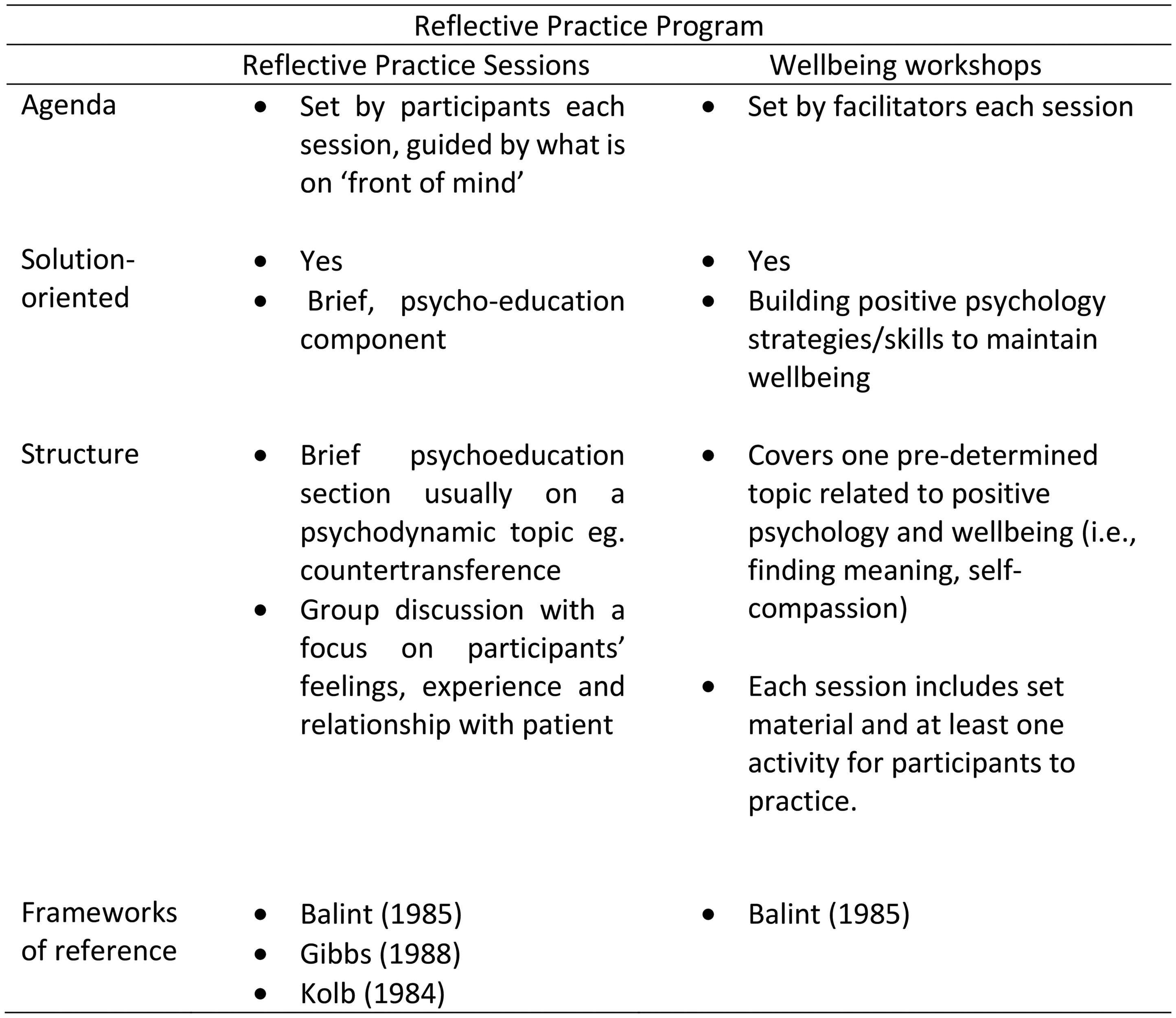
Difference between reflective practice sessions and wellbeing workshop.
Program delivery
Reflective Practice program sessions were provided monthly for each unit of the hospital, for one hour. In order to facilitate attendance of all clinicians on the unit, a roster of covering staff was arranged by senior operational management staff who sat outside of each of the units. The sessions were provided individually to each unit of the hospital, and all clinical staff who were rostered on attended. As noted, whilst reflective practice sessions occurred on half of the hospital’s units, on alternate units, the wellbeing workshops were provided, to focus solely on positive psychology strategies to maintaining emotional wellbeing.
The purpose of the current study was to describe the impact of a novel, structured Reflective Practice program in a forensic mental health facility, where challenges such as rostering of staff and management of patient risk were significant. Specifically, the study aimed to 1) assess the effectiveness of the reflective practice framework program in improving staff wellbeing, self-efficacy and reflective capacity, 2) examine staff experience and acceptability of the program across all levels of the organization and 3) further explore the potential relationship between reflective practice and self-efficacy that has been identified in previous research.
Method
Research design
This study adopted an exploratory, mixed method research design. Surveys were administered to all clinicians at baseline and six months post implementation of the program to collect quantitative data on clinician wellbeing, self-efficacy and reflective capacity. The quantitative survey data was designed to assess the effectiveness of the Reflective Practice program in improving staff wellbeing, self-efficacy and reflective capacity (study aim 1) and explore the potential relationship between reflective practice and self-efficacy (study aim 3). Feedback interviews were also conducted with key clinical stakeholders following six-eight months of implementation to qualitatively examine perceived impact and acceptability of the program across all levels of the organization (study aim 2). The study was approved by the Swinburne University of Technology Human Research Ethics Committee
Study setting
Thomas Embling Hospital (TEH) is a 136-bed secure facility operated by the Victorian Institute of Forensic Mental Health (Forensicare), Victoria’s leading provider of forensic mental health care. Forensicare operates in the public sector and also provides community- and prison-based services. TEH has eight units, ranging from acute to continuing care, as well as a dedicated women’s unit. In 2020, 364 part-time and full-time clinical staff worked at TEH, and could access the Reflective Practice program.
Participants
Clinical staff at the hospital comprised nursing, allied health (psychology, occupational therapy and social work) and medical disciplines. All clinical staff could access the Reflective Practice program and were invited to take part in the evaluation of the program. Senior management staff at the hospital (eg. operational managers, nurse unit managers, clinical leads) were also included in the evaluation due to their role overseeing the implementation of the program (i.e., providing backfill to support clinicians to attend the program as a unit) and supervision of clinical staff which enabled observation of the impact of the program on staff.
Data collection
Clinicians were invited to complete questionnaires, prior to participating in the program and six months post-implementation of the program. The questionnaires comprised a series of validated measures assessing reflective practice capacity, emotional wellbeing and occupational self-efficacy, as well as items examining staff perceptions of the program and clinical experience. The questionnaire took approximately 20 minutes to complete and was administered both online and in pen and paper format. All surveys were completed anonymously. Participants were asked to assign a unique code to the completed survey so responses to the survey at the two timepoints could be matched to the individual to assess the change in outcome measures over time. Plain language statements were also provided with the surveys, outlining the details of the research study and the associated risk and benefit to participating. Written consent was not obtained from clinicians who chose to complete the survey in order to preserve anonymity.
Key clinical stakeholders at the hospital were also invited to participate in semi-structured interviews six to eight months post-implementation of the program. These stakeholders included representatives from operational management, Nurse Unit Managers (NUMs) and senior medical, nursing and allied health staff. The purpose of the interviews was to obtain an understanding of the perceived impact of the program across all levels and departments of the organization. Feedback from organizational management was particularly of interest given their role in coordinating the logistical aspects of the program implementation (ie., organizing rosters to accommodate program attendance). The interviews were conducted online and over the phone and took approximately 30 minutes of time. The interview questions were designed to examine the impact of the Reflective Practice program across the organization. Written consent was obtained from all clinical stakeholders who took part in the interviews. Prior to commencing the interviews, a verbal overview of the research and the associated risk and benefit to participating was also provided by the researcher.
Measures
The surveys comprised questions around basic demographic information, prior experience of Reflective Practice and measures assessing reflective practice capacity, self-efficacy and wellbeing.
The reflective practice questionnaire
Reflective practice capacity was assessed via the Reflective Practice Questionnaire (Priddis & Rogers, 2018). The Reflective Practice Questionnaire (RPQ) comprises 48 Likert scale items assessing four core components of reflective capacity (ie., reflection after action, reflection-in-action) and six associated correlates of reflective practice capacity (ie., Confidence, uncertainty, job satisfaction). The measure has been validated with Australian mental health clinicians (n = 45), general Australian population (n = 188) and medical professionals in the USA (n = 150). All subscales of the questionnaire indicate good internal reliability (α=.82 to .91).
Occupational self-efficacy questionnaire
Self-Efficacy was assessed via the Occupational Coping Self-Efficacy Questionnaire for Nurses (Pisanti et al., 2008). The measure contains nine statements describing stressful situations which commonly arise in the nursing workforce and asks respondents to rate how easily they are able to cope on a 5 point Likert scale (1 = not at all easy to cope with to 5 = totally easy to cope with). The scale has been validated in nursing populations internationally and indicates good internal reliability (α=.77 to .79) and correlations with factors on the Coping Inventory Stressful Situations Short Version scale (Endler &Parker, 1999) and Maslach Burnout Inventory (Maslach et al., 1997) provide support the criterion validity of the questionnaire.
The officer wellbeing scale
The Officer Wellbeing Scale was administered to assess emotional wellbeing (Trounson et al., 2019). The OWS presents a list of 19 emotional states and asks staff to rate how frequently they have experienced these states in relation to their work on a scale of 1 (Never) to 7 (Always). The scale has been validated in a sample of Victorian prison officers, indicating a two factor model comprising Distress and Thriving subscales. The scale has been validated with 174 Victorian prison officers and shows good internal reliability (α=.94) and positive association with workplace adversity. Although there are several differences between the job description of prison officers and clinicians, the scale was considered more suitable for use than wellbeing measures used in general population or healthcare populations, because forensic mental health clinicians encounter similar challenges in daily work as staff in correction settings, such as experiencing and witnessing incidents of verbal and physical aggression.
Data analysis
All data were analyzed using SPSS version 26. Means, standard deviations and frequencies were calculated to describe study participants. Independent t-tests were conducted to examine the difference in wellbeing, self-efficacy and reflective practice capacity between staff responding to the baseline and post-implementation survey. Hodge’s g was calculated to assess the size of significant differences detected by the t-test. Through the assignment of unique codes, a small number of pre and post responses were able to be matched to an anonymous staff member, to examine change in the outcome measures over time (n = 10). A paired samples t-test was conducted on this subset to assess for the individual change in self-efficacy, wellbeing and reflective practice capacity following participation in the program. Cohen’s d was calculated to measure the size of any significant change observed.
Further independent t-tests were conducted on responses post-implementation to examine the difference in staff scores between across length of time at the hospital (five years or less versus six years plus), the number of program sessions attended (low = 1-3, high = 4-10) and the type of program session attended (Wellbeing workshops only versus reflective practice or combination of reflective practice and wellbeing sessions). A Bonferonni correction was applied to the additional analyses exploring differences in post-implementation scores (.05/3=.017). Chi-square tests were performed to examine the difference in level of understanding and perceived use of the program at the two timepoints. Where more than 20% of categories contained n < 5 responses in the contingency table, the Freeman-Halton extension of Fishers exact test was examined. Pearson’s correlations were calculated to examine the size and direction of the relationship between reflective capacity, self-efficacy and wellbeing.
Finally, a six-stage reflexive thematic analysis was conducted on the stakeholder feedback interviews to identify, analyze and reports key themes within the data (Braun & Clarke, 2006). This method involved an inductive, and iterative approach to familiarization with the data and the generation of codes and themes.
Results
A total of 47 clinicians completed the survey pre-implementation of the program and 30 completed the post-implementation survey. Table 1 presents the characteristics of responding staff members both prior to and post-implementation of the Reflective Practice program. The responding sample was loosely representative of the clinical population, with only representation from the psychiatry discipline lacking.
Characteristics of survey respondents.
TEH (Thomas Embling Hospital).
Table 2 describes staff participation in the Reflective Practice program at the hospital. The number of program sessions attended by staff ranged from 1-10, with over one third taking part in a combination of reflective practice sessions and wellbeing workshops since commencing the program (n = 12, 40.0%). Post-implementation, staff were significantly more likely to report good to excellent understanding of reflective practice when compared to staff pre-implementation (X2 = 11.186, p = .011). There was no significant difference observed in the rating of the usefulness of reflective practice between staff pre and post implementation of the program, with the majority indicating usefulness at both timepoints.
Engagement with reflective practice program and perceived usefulness.
n = 2 missing from pre-implementation, ^n = 1 missing from post-implementation, +Fisher-Freeman-Halton.
Table 3 outlines the wellbeing, self-efficacy and reflective practice capacity scores amongst staff at pre-implementation and post-implementation of the program. Staff post-implementation reported significantly higher scores on confidence in their work when compared to staff pre-implementation (t(66) = − 1.792, p = .039, g = .433). Similar results were observed, when examining the change in scores among the subset of participants who were matched pre and post-implementation (n = 10).Among this smaller group, a significant improvement was observed in several correlates of reflective practice capacity, with staff indicating a significant increase in confidence in their work (t(9) = 3.687, Cohen’s d = 1.28, p =.003; M = 2.40, SD = .44 and M = 3.35, SD = .95, respectively for pre and post scores), as well as a reduction in uncertainty managing patients (t(9)=3.078, Cohen’s d = 0.59, p = .007; M = 3.55, SD = .60 and M = 3.18, SD =.67, respectively for pre and post scores) and a desire for improvement (t(9) = 2.57, Cohen’s d = 0.58, p = .015; M = 5.10, SD = .74 and M = 4.60, SD =.97, respectively for pre and post scores).
Scores on outcome measures pre and post-implementation.
p<.05, ^RPQ (Reflective Practice Questionnaire).
Correlations between reflective practice capacity subscales and outcome measures at post-implementation (n = 30).
significant at p<.05.
Conversely, further examination of post-implementation data found staff with five years or less experience at the hospital indicated significantly lower scores on confidence in their work when compared to more experienced staff (six years plus) at the hospital (M = 3.06, SD = .93 and M = 3.94, SD=.82 respectively; t(28) = 2.72, p =.011) as well as significantly higher stress (RPQ) scores (M = 3.50, SD =.77 and M = 2.63, SD = .63 respectively; t(28) = 3.34, p = .002). Following the application of a Bonferonni correction for multiple comparisons, there were no significant differences in the outcome measures across the number of sessions attended nor the type of sessions attended (p > .017).
Pearson’s correlations were obtained to examine the association between reflective capacity scores, with self-efficacy and wellbeing at six months post implementation. Significant large effects were observed for the association between lower job satisfaction scores and both higher distress (r = − .514, p = .004) and lower thriving scores (r = .562, p = .001). Good communication was associated with high wellbeing (thriving) scores (r = .509, p = .004) and to a lesser extent self-efficacy (r =.366, p =.047). Finally, high stress was associated with high staff distress (r = .576, p =.001). No other significant correlations were observed.
A total of six feedback interviews were conducted with key clinical stakeholders at the hospital. Participants included Nurse Unit Managers (n = 2), Operational Managers (n = 2) and Psychiatric Consultants (n = 2). Analysis of the stakeholder feedback identified three distinct features pertaining to the benefit of the program and facilitators and barriers to the program.
Observed benefit of the program
Participating stakeholders all noted a positive response to the Reflective Practice program across the hospital (see Figure 3). A noticeable improvement in team cohesion on the unit was reported, as well as increased communication across the multidisciplinary team and collaboration across disciplines. The improvements were attributed to the solution focused dialogue enabled by the reflective practice sessions. Staff felt that the focus on problem-solving facilitated skill development, particularly around managing emotional responses to complex patients and dynamics of the inter-disciplinary team. The solution- focus of the program also assuaged the initial reluctance to attend the program initially observed among clinicians already receiving clinical support and supervision, as the practical value of the program was quickly realized. Some staff members had disclosed that providing relief for staff on other units to attend the program fostered inter-unit collaboration and expanded their own skills and ability to adapt to various tasks.
Observed benefit of the Program.
Importance of organizational support
Most staff recognized the effort and resources invested in the implementation of the Reflective Practice Program at the hospital, particularly that relief staff were provided for the entire unit to attend sessions (see Figure 4). Initial reluctance to attend the Reflective Practice Program was observed, largely due to concerns around workload or handing over care of complex patients to an unfamiliar clinician. Although there was consistent messaging from hospital leadership to prioritize program attendance, it was the practical resources offered (backfill of staff so that clinicians could attend the program as a unit) that contributed to staff feeling that senior management were committed to supporting wellbeing and clinical). Clinicians valued having specific time allocated to their wellbeing and skill development and felt that stepping off the workspace encouraged more open discussion amongst the team. Protected time to focus on workplace wellbeing and refine clinical practice was especially valued by nursing staff, who traditionally do not have the time or resources allocated to leave the floor.
Importance of organizational support.
Program structure
All participating stakeholders highlighted that the frequency of the program was not meeting the needs of staff (See Figure 5). Due to the variations in rosters, large service demand and monthly delivery schedule most staff had not received consistent program delivery (attendance ranged from 1-10 sessions). All participants felt that in order to obtain the maximum benefit of the program, more frequent and consistent engagement was required. The program content however, was highly valued by staff. The patient centric format of the reflective practice sessions enabled an easy, open and honest dialogue between team members. Staff also disclosed that having an external clinician, objective to the unit, reduced the tensions of speaking openly in a hierarchical team.
Program structure.
Discussion
This study sought to address many of the limitations in previous research on the benefit of reflective practice by providing clarity around definitions, model and process (Dube & Ducharme, 2015; Heneghan et al., 2014). The novel, structured reflective practice program was positively received by staff from all levels of the forensic inpatient mental health service, with improved team cohesion observed across the multidisciplinary team reported following engagement with the program. In line with previous research indicating the benefits of reflective practice for skill development (Caldwell & Grobbel, 2013; Hancock, 1998; Rees, 2013; Wilding, 2008), clinicians in this study reported increased confidence and reduced uncertainty in clinical roles following participation in the Reflective Practice program. Although post-implementation, there was no significant difference in staff reports of the perceived usefulness of reflective practice as a support process, this was likely due to the high number of staff that disclosed belief in the usefulness of such a process prior to commencing the program (80%).
The acceptability of the novel structure of the Reflective Practice program was indicated by participant requests for more frequent program sessions. It was initially thought that staff at the hospital had a low level of ‘readiness’ to participate in the Reflective Practice program and would need gradual exposure to feel comfortable being vulnerable amongst their peers. However, these results suggest that appointing program facilitators with familiarity with the organization and knowledge of the challenges clinicians encounter, contributed to the psychological safety and readiness of participants to engage with the reflective practice process. Notwithstanding, various unit groups demonstrated the idealization and denigration of the process/reflective space over time, which required ongoing processing and management by facilitators. This is noted as evidence of the need for experienced and suitably trained facilitators alongside regular supervision for facilitators to process their own countertransference.
The study also highlighted the need to introduce the process of reflective practice to clinicians early in career training, to support learning and integrate clinical theory and practice (Mann et al., 2009). In forensic mental health settings in particular, supporting newly qualified clinicians is particularly important given the unique features of patient cohort (i.e., high prevalence of comorbidity and incidence of aggression) as well as risk of vicarious trauma and burnout (Brown et al., 2017; Oates et al., 2020; Pirelli et al., 2020). Such challenges also lend support for the need to include wellbeing workshops as a part of a Reflective Practice program, to provide proactive support for staff, in the form of specific coping strategies, alongside the reflective process.
The acceptability of the program in the inpatient setting relied heavily on buy-in from senior management and implementation from ‘the top down’. Clinicians commenced the Reflective Practice program despite feeling uncertain about leaving work unfinished and clients in the care of unfamiliar staff, only because the program was promoted as a priority by senior management. Providing backfill for staff not only facilitated clinician engagement with the program but promoted skill development, by allowing clinicians to work outside their usual role and extend their skills while covering for colleagues.
It is important to note however, that resistance to the program was observed among some clinicians, particularly early in the program when benefit was not realized. In this implementation of the Reflective Practice program, there was no clear channel of responsibility organized to deal with staff resistance and other operational issues as they occurred. This meant that any grievances with the initiative were at times brought to the Reflective Practice program sessions and required intervention/comment by facilitators. Future implementations would benefit from more consideration of change management principles, including key stakeholders and their associated responsibilities in implementing such change. Aside from being good practice and maximizing the likelihood of success of the program, this would also preserve the reflective space for issues that are beneficial to the staffing group in the longer term. Such logistical issues also contributed to the slow exposure to the Reflective Practice program sessions, with some staff attending but not participating. Slow exposure to the program was an inevitability with the implementation of the program, given that nursing shifts in particular varied week-to-week and clinicians could not consistently attend the program.
Low dosage (ie., program attendance) is a significant limitation of this study. Although the flexibility of the Reflective Practice program schedule was essential for the sustainability of a hospital-wide implementation that could be embedded into the organizational systems, the pragmatic approach to program delivery culminated in varied attendance in the program and small samples for statistical analyses. For example, comparisons of the scores on outcome measures according to the type of program session attended (ie., wellbeing workshops versus a combination of reflective practice sessions and wellbeing workshops) were limited by the number of participants who attended (n = 6, wellbeing workshops only, n = 11, reflective practice sessions only and n = 11, combination of both sessions). Further, individual change in clinician scores of reflective practice capacity, wellbeing and self-efficacy following participation in the Reflective Practice program could only be examined in a small sample of staff members (n = 10). Calculations of the effect size in such a small sample of participants can increase the margin of error of estimates. Subsequently, the substantial increase in confidence and reduction in uncertainty of clinical practice observed following engagement with the program should be interpreted with caution and understanding that further study is required to ensure the replicability of the findings observed.
Aside from the low dosage, only 10% of clinical staff took part in the research (n = 47) and few psychiatry respondents were observed. Although it is possible that the program did not have any impact on the wellbeing or self-efficacy of clinicians in the inpatient forensic mental health setting, it is also likely that small differences in these outcome measures could not be detected because of the low dosage and power of the study (sample size required to detect an effect). It is recommended that future research of the program adopt a longer implementation period (12-24 months) in order to obtain a larger sample size that allows for the flexibility of the program.
Due to the limitations of the pragmatic study design and small sample size, this research is largely exploratory. Nevertheless, the study provides clarity around the definitions, model and process adopted in reflective practice. Embedding the novel, structured Reflective Practice program into clinician rosters, facilitated clinician engagement with the program and enabled early observations of improved team cohesion and confidence in clinical work. The results highlight the potential for the novel structured Reflective Practice program, to support clinician learning and morale. Further research can build on the exploratory findings identified in this study by examining the replicability, and relationship between program dosage with wellbeing, self-efficacy and reflective practice capacity, particularly among early career clinicians.