
Abstract
Obesity and metabolic syndrome are disproportionately prevalent among people with mental disorders, particularly those subject to long periods of inpatient care where sedentary lifestyle and medication side effects can be compounding problems. This study reports on a cross-sectional survey of 28 patients under forensic mental health care in a high secure inpatient service in Queensland, Australia. The study comprises a file review, structured questionnaire and an interview, to evaluate the physical health and activity, as well as possible causes of low physical activity of these patients. Rates of overweight (50.0%), obesity (46.6%), and metabolic syndrome (39.3%) were very high within the study population. Mean waist circumference measurements were also high for both females (110.8 cm) and males (109.0 cm). Around one half of the study population (46.4%) did not meet the World Health Organization’s recommended levels of physical activity. Self-reported low levels of physical activity were significantly associated with the presence of comorbid medical illness (p = 0.007). Further research investigating the factors contributing to poor physical health and low activity levels within this population will support attempts to understand and address the physical health needs of this population.
Introduction
Obesity and low physical activity levels of patients under mental health care are associated with poorer health outcomes compared to the general population, including higher rates of cardiovascular disease, premature death, and higher health care costs (De Hert et al., 2011; Druss et al., 2011). This has implications for forensic mental health services. Recent reviews have documented the high rates of overweight and obesity for inpatients under forensic mental health care as well as concerns relating to weight gain during admissions, the development of metabolic syndrome and associated medical illnesses, and the low uptake of current international physical activity guidelines (Moss et al., 2022; Rogers et al., 2019). There is now an acknowledgement that the physical health and physical activity of patients with severe mental illness is an important area for all clinicians to consider in the recovery of their patients. The National Institute for Health and Care Excellence guidelines (2014), as well as the Royal Australian and New Zealand College of Psychiatrists guidelines for schizophrenia (Galletly et al., 2016), recommend the use of psychosocial interventions, including physical activity, to reduce symptom severity, morbidity, and mortality and to facilitate recovery.
In Australia, secure forensic hospitals are the inpatient facilities that generally assess, treat, and provide rehabilitation for individuals with complex mental health needs, who require high levels of physical, procedural, and relational security. These individuals usually have been in contact with the criminal justice system or have been deemed to be high risk civil patients. Individuals admitted to forensic hospitals are usually detained under state or territory Mental Health Act legislation and may be admitted from watchhouses, prisons, or directly from the community. There are approximately 350 high security inpatient beds for people requiring forensic mental health care across Australia, of which 70 are in Queensland. Forensic hospital environments have been considered to contribute to concerns of weight gain and obesity by providing limited food choices and a more sedentary lifestyle with fewer opportunities for spontaneous exercise (Long et al., 2014). Individuals are also more likely to be treated with high doses of weight increasing antipsychotic medications, further compounding the issue.
While there is evidence available from general mental health settings to provide guidance on improving physical health and activity levels (Czosnek et al., 2019), forensic services have been slow to adopt and investigate these findings within their settings. Postulated reasons for this include concerns related to risk such as health risks due to patients’ poor physical conditions, safety issues around physical activity monitoring and equipment, challenges relating to access to patients and staff confidence in providing interventions in settings that are highly restrictive in nature. Where attempts have been made to investigate and improve patients’ physical health and activity in forensic or secure settings, reviews have noted the absence of well-designed, experimental studies and raised concerns related to the quality of the reporting of such studies (Moss et al., 2022; Rogers et al., 2019).
Furthermore, while previous research has identified consistent correlates of physical activity in the general population (motivation, self-efficacy and self-regulation) and for the general mental health population (presence of negative symptoms of schizophrenia and cardio-metabolic co-morbidity), there remains unanswered questions regarding what the determinants of physical activity are for patients under forensic mental health care within a high secure hospital (Rhodes et al., 2017; Vancampfort et al., 2012). Given the findings of high rates of overweight and obesity and weight gain during admissions for forensic patients, there remains gaps in knowledge as to why these issues are so prominent for this population. The current study was designed to assess physical health and activity levels, and to investigate the determinants of physical activity, for patients under forensic mental health care within a high secure hospital.
Methods
Study design
This research comprised a mixed methods study which included a cross-sectional survey by file review, structured questionnaire and a semi-structured interview of patients admitted to the High Secure Inpatient Service (HSIS) at The Park, Centre for Mental Health (Brisbane, Australia). This paper reports on the findings of the cross-sectional survey which was undertaken between February 2019 and February 2020. The conduct and reporting of this survey adhered to the STROBE statement for cross-sectional studies (Vandenbroucke et al., 2007). Ethical approval was granted by the West Moreton Health Human Research Ethics Committee (HREC/18/QWMS/67) and the University of Queensland (clearance number 2018002132).
Setting
The HSIS is a state-wide service in Queensland, Australia, which provides a highly supervised, supportive, and secure hospital environment for approximately 70 individuals. The state of Queensland in Australia has a population of around 5.2 million with an approximate high secure forensic mental health bed rate of 1.34 per 100,000. At the start of the study period the HSIS had 68 admitted patients. Over the course of the study there was a total of 59 admissions and 52 discharges. The hospital admits a mixed cohort of individuals who are found not criminally responsible (of unsound mind) by a court for an offense, who are unfit for trial, or who have been transferred for assessment and treatment from the prison system or the community, as they require inpatient mental health care, but their risk profile does not allow transfer or ongoing admission to a local hospital. This usually occurs under the provisions of the state Mental Health Act 2016 legislation, although in rare circumstances a patient may be admitted voluntarily from prison.
At the time of data collection, HSIS offered patients a variety of physical activity options including a daily campus walk and, less frequently, smaller group activities. Group activities were only able to be offered when there was adequate staffing available. The HSIS is resourced with a gymnasium, outdoor swimming pool, outdoor tennis court and outdoor exercise equipment. The expansive grounds permit small groups to play modified touch football, soccer and volleyball games. Participation in physical activities offered outside the ward environment is limited to those who have been granted campus leave (i.e., permission to leave the ward environment) and whose treating teams have approved the activity. Physical activity has previously been prescribed by the physiotherapist, exercise physiologist or personal trainer, however, currently there is no exercise physiologist or personal trainer employed. Physical activity is usually monitored by the recreational therapists and nursing staff, but again this is highly dependent on staffing numbers and availability. At times, resourcing has afforded Tai Chi to be offered in wards.
Participants
Eligible participants were male and female adults (aged 18 and over) who were admitted to the HSIS. Other inclusion criteria were that the person had a diagnosis of a major mental illness (defined as schizophrenia spectrum and other psychotic disorders, mood and anxiety disorders and severe personality disorders), and were assessed by their treating psychiatrist as having the capacity to consent to the study. One researcher (KM), who was working as a psychiatry registrar (psychiatrist in training) at the time of the study, invited patients to take part in the study after discussion with the patient’s treating psychiatrist. Additionally, capacity to consent to the study was assessed by the researcher (KM) at the time of obtaining written consent. Patients were excluded from the study if they were unable to give informed consent (either by virtue of a deteriorated mental state or due to intellectual impairment) or were unable to comprehend written English. Participants were offered a $10 gratuity.
Eligible participants were advised that their participation was entirely voluntary and that they were free to withdraw from the study at any time. It was highlighted that an individual’s decision to not participate would not affect their routine treatment or their relationship with the treating team.
Data collection
Data were collected by a review of patient file notes, a structured questionnaire and interview. The specific data variables, method of collection and comments are available in the supplementary material.
Demographic variables
Demographic information obtained from the electronic file included date of birth, sex, ethnicity, Mental Health Act status, diagnosis, current medication and doses, comorbid illnesses (including presence of metabolic syndrome), length of stay, weight change and number of seclusion episodes. Demographic information obtained by interview included family history of cardiovascular risk factors and smoking status. Additional information regarding the presence of comorbid illnesses and weight change was also sought at interview.
Mental health act status
The majority of individuals are admitted to high secure inpatient units under relevant Mental Health Act legislation. In Queensland, patients who have been charged with a serious offense who are found of unsound mind or unfit for trial are placed under Forensic Orders (FO) while individuals who lack the capacity to consent to treatment for their mental illness are placed under Treatment Authorities (TA). Individuals who are transferred from a place of custody (e.g., watchhouse or prison) to mental health inpatient facilities such as HSIS are admitted as classified patients and may be admitted voluntarily or involuntarily. Involuntarily classified patients are treated under a TA – Classified.
Diagnosis
Psychiatric diagnoses according to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) were recorded. Grouping was required for statistical disclosure control.
Medications and chlorpromazine equivalent dose
Differences in antipsychotic medication doses were expressed as chlorpromazine equivalents, with conversion utilizing estimated equivalent doses documented in the current Maudsley Prescribing Guidelines 13th Edition (Taylor et al., 2018).
Presence of metabolic syndrome
The presence of metabolic syndrome was determined by the current International Diabetes Federation (IDF) definition (IDF, 2006). In addition to central obesity (defined as waist circumference with ethnicity specific values or a body mass index [BMI] > 30 kg/m2), two of the following must be present: raised triglycerides (1.7 mmol/L or specific treatment for hyperlipidaemia), reduced HDL-C (<1.03 mmol/L in males and <1.29 mmol/L in females or specific treatment for this lipid abnormality), raised blood pressure (systolic BP ≥ 130 or diastolic BP ≥ 85 mm Hg or treatment of previously diagnosed hypertension) or raised fasting plasma glucose (≥5.6 mmol/L or previously diagnosed type 2 diabetes).
Seclusion
A rate of seclusion was calculated by dividing the total number of episodes of seclusion by the length of stay (days).
Anthropometric and physiological variables
File records of height (m) and weight (kg) were used to calculate BMI (kg/m2) and weight change. All other variables (waist circumference, blood pressure, resting heart rate, cholesterol, HDL-C, LDL-C, triglycerides and fasting glucose) were the latest result documented in the electronic file or electronic pathology results at the time of data collection.
BMI and weight change
BMI was categorized underweight (BMI < 18.5 kg/m2), healthy weight (BMI 18.5 to 24.99 kg/m2), overweight (BMI 25.0 to 29.99 kg/m2), or obese (BMI ≥30 kg/m2) in alignment with the World Health Organization (WHO) cutoff standards (WHO, 2000). Weight change during admission was calculated from the most recent weight and weight on admission.
Physical activity variables
The International Physical Activity Questionnaire - Short Form (IPAQ-SF) was used to determine amounts of physical activity and sedentary behavior in the study population. Its use has been validated in a population of individuals with schizophrenia (Faulkner et al., 2006). The IPAQ-SF is a self-report questionnaire with seven questions about the type of physical activity undertaken in the past seven days, which can provide an estimate of metabolic equivalent minutes per week (MET-min/week). Metabolic equivalent (MET) is a measure of energy expenditure during physical activity, with 1 MET equivalent to the energy used by the body while at rest. Moderate physical activity is considered to be between 3.0 and 6.0 METs. A MET-min/week of 600 was used as a cut off for reaching the current WHO’s recommendation that adults aged 18-64 should do at least 150 minutes of moderate intensity aerobic activity per week (Bull et al., 2020).
Study sample size
Participant numbers from previous cross-sectional studies examining the physical and health variables of patients under forensic mental health care have ranged from 28 to 408 depending on the size of the hospital and length of the study (Bergman et al., 2020; MacFarlane et al., 2004). The low number of high security beds per population in Queensland was a significant rate limiting step with regards to participant numbers in our study. Other factors limiting participant numbers related to capacity to consent to participation and length of stay (individuals transferred from prison often had much shorter admissions). We aimed to recruit as many participants as we were able to across the course of the 12 month study.
Statistical analysis
Descriptive statistics were used to summarize patient data. Discrete variables were summarized using frequencies and percentages. Continuous variables that were normally distributed were summarized using means and standard deviations (SD), while continuous variables that were not normally distributed were summarized using medians and interquartile (IQR) ranges. The proportions of patients with metabolic syndrome and a range of other medical illnesses were recorded. Inferential analyses conducted were exploratory in nature and aimed to explore potential relationships between variables. Pearson’s correlation coefficients were computed to assess the relationships between levels of physical activity and a range of possibly related factors including BMI, waist circumference, length of stay, antipsychotic dose, and rate of seclusion. Two sample t-tests were performed to assess if there were any significant differences in the presence of comorbid medical illness, metabolic syndrome and sex when comparing physical activity levels (MET-minutes). Two-sided p-values of less than 0.05 were considered statistically significant. All quantitative analyses were conducted using R version 4.1.0 (R Core Team, 2021).
Results
Demographics
At the start of the study 68 individuals were already inpatients at the HSIS. Over the study period there were 59 admissions. Thirty-one patients who were referred by their treating psychiatrists were determined to meet study criteria. Of these, three individuals declined to participate. A total of 28 participants were included in the study (Figure 1).
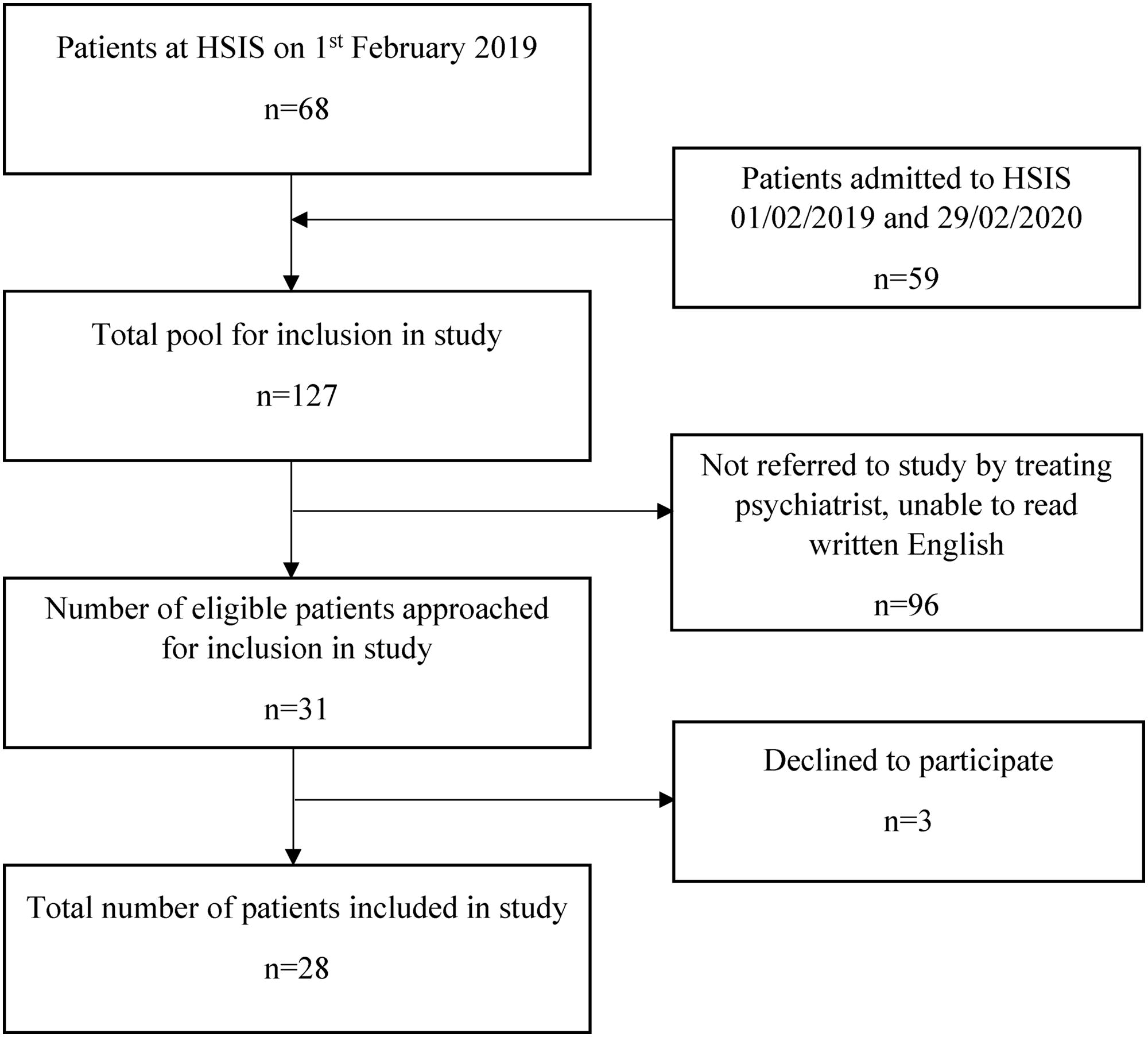
Participant recruitment and eligibility.
Participant demographics are outlined in Table 1. The majority of patients were male (78.6%). The mean age of patients was 41.7 years (SD = 14.1). For males this was 42.3 years (SD = 13.9) and for females it was 39.5 years (SD = 15.7). Patients’ length of stay, at the time of their participation, ranged from 55 days to 6,852 days, which is approximately 18.8 years (median 741, IQR 1322.5).
Cohort characteristics.
All patients recruited for the study had a diagnosed major mental disorder: schizophrenia and other psychotic disorder was the most prevalent (75.0%), followed by schizoaffective disorder (14.3%) and bipolar affective disorder (10.7%). All patients were detained in hospital under the Queensland Mental Health Act 2016 under the following orders: Forensic Order (75.0%), Treatment Authority—Classified (14.3%) and Treatment Authority (10.7%). Nearly half (46.4%) were treated with dual second-generation antipsychotic therapy. The average chlorpromazine equivalent dose of antipsychotic medication prescribed to patients was 606.1 mg.
Anthropometric, physiological and physical activity measures
Anthropometric and physiological findings relating to BMI, waist circumference, blood pressure, heart rate, triglycerides and cholesterol by gender and total sample are presented in Table 2. The mean number of MET-minutes achieved by patients was 1232.7 (SD 1410.3) per week (Table 2). Approximately half (53.6%) of the sample population self-reported physical activity levels that met the current WHO physical activity guidelines for adults.
Anthropometric, physiological and physical activity measures for inpatients under forensic mental health care.
BMI = body mass index, bpm = beats per minute, HDL-C = high density lipoprotein cholesterol, LDL-C = low density lipoprotein cholesterol, MET-minutes = metabolic equivalent minutes, WHO = World Health Organization, PA = physical activity.
Metabolic syndrome and medical illnesses
Table 3 documents the high rates of metabolic syndrome (39.3%) found in our study population sample. The rate was higher for males (45.5%) compared to females (16.7%). Of note, 17.9% of our study population had comorbid endocrine disorders while 10.7% had comorbid cardiovascular and respiratory illnesses.
Metabolic syndrome and comorbid illnesses.
Factors associated with physical activity
The results of bivariate analyses between physical activity levels and a range of health and environmental factors are presented in Table 4. No statistically significant correlations were found between physical activity levels and BMI, waist circumference, length of stay, antipsychotic dose, or rate of seclusion. Table 5 outlines the results of t-tests between physical activity levels and demographic and health factors. When comparing physical activity levels between groups, those with comorbid medical illness reported significantly lower levels of physical activity (t (26) = −2.91, p = 0.007).
Results of bivariate analyses between physical activity levels and a range of health and environment related factors.
Results of t-tests between physical activity levels and demographic and health factors.
Discussion
Physical health findings
Our study documented very high rates of overweight or obesity (96.6%) and metabolic syndrome (39.3%) for individuals under forensic mental health care within an Australian cohort. When compared to a similar forensic population in the UK, the patients in our study had higher rates of endocrine disorders (17.9% compared to 3.0%) but similar rates of comorbid cardiovascular disease (Cormac et al., 2005). A comparison of a range of comorbid illnesses and smoking can be found in the supplementary material. Patients under forensic mental health inpatient care also appear to have higher levels of cardiovascular disease and rates of smoking compared to the general adult population in Australia (Tanamas et al., 2013). This is a serious concern for individuals who are detained in high secure inpatient settings and for the services who manage the care of these individuals. These findings are consistent with the findings of recent systematic reviews which have highlighted the high prevalence of metabolic syndrome, diabetes, dyslipidaemia, hypertension, overweight/obesity and cardiovascular disease in people with psychotic disorders in secure settings compared to the general population (Ma et al., 2020). Of particular note is that these have been reported in earlier studies from overseas, demonstrating that there has been little change for this cohort of individuals over the past 15 years. Concerningly, overweight and obesity are reportedly set to overtake smoking as the risk factor contributing the most to the burden of disease in Australia (Australian Institute of Health & Welfare, 2020).
Waist circumference, a simple and inexpensive measure of unhealthy body fat, has been found to be the strongest predictor of metabolic syndrome in a meta-analysis of metabolic syndrome in people with schizophrenia (Mitchell et al., 2013). However, measurement of waist circumference continues to be underutilized in clinical practice and these measures are often absent on electronic monitoring forms (Stanton et al., 2017). In a recent scoping review, waist circumference was reported in only four of 17 studies documenting physical health and activity outcomes for individuals under forensic mental health care, a population that is known to be at increased risk of developing metabolic syndrome, diabetes mellitus and cardiovascular disease (Moss et al., 2022). The current study documented elevated means of waist circumferences for both males (109.0, SD 15.2) and females (110.8, SD 21.4), which is consistent with the high rate of metabolic syndrome also found in this population (39.3%). The measurement of waist circumference is also an important measure for documenting improvements in anthropometric measures, with statistically significant improvements in waist circumference documented following physical activity interventions in forensic populations (Hjorth et al., 2014; Murphy et al., 2019).
Physical activity levels
Our study found that low physical activity levels were significantly associated with the presence of comorbid medical illness. This finding further highlights the importance of screening for and managing physical health issues in patients under forensic mental health care. We are not aware of previous studies examining factors contributing to low physical activity levels within a forensic inpatient setting. We explored potential relationships between physical activity and range of health and environmental related factors including BMI, waist circumference, length of stay, antipsychotic equivalent dose and rate of seclusion. However, tests of correlation did not reach statistical significance for these factors. We acknowledge that our study size was small, and that all of our correlations were considered weak. We also note that based on the effect sizes that we observed (r = −0.03 to −0.24 and r = 0.05) we would have needed a larger sample size to demonstrate statistical significance. In addition, we collected data on physical activity with the IPAQ-SF, a self-report measure. While this has been validated for use with individuals with schizophrenia (Faulkner et al., 2006), there is some documented evidence that people with severe mental illness underestimate the amount of sedentary behavior they engage in and overestimate vigorous activity levels (Vancampfort et al., 2017).
Six small heterogenous studies have previously reported on physical activity for patients under forensic mental health care (Bacon et al., 2012; Bergman et al., 2020; Hilton et al., 2015; Long et al., 2014; Long et al., 2015; Savage et al., 2009). A variety of different measures were used to capture physical activity levels including accelerometry, the IPAQ-SF (Swedish version), the New Zealand Physical Activity Questionnaire Short Form, the Problem Identification Checklist and documented time during activities/session attendance, making it difficult to compare physical activity levels between studies. Bergman et al. (2020) also documented whether individuals met the current WHO guidelines for physical activity and found that 36% of participants (9/25) did not. Within our study population, 46.4% of participants did not meet current guidelines. While this is not worse than current data for the general population, which suggests that more than half (55%) of the general Australian population do not meet the physical activity guidelines (Australian Bureau of Statistics, 2015), it could be asserted that our population should be aiming for greater physical activity levels given their significant health risks of overweight, obesity, comorbid illness and metabolic syndrome.
Weight change during admissions
A recent paper by Pedersen et al. (2022), investigating associations between hospitalization time and change in body weight and other cardiometabolic risk factors among forensic mental health patients, documented a significant positive dose-response association with weight change for hospitalized patients compared to outpatients. The forensic patients who were exclusively treated outside of hospital gained 0.7 kg per year on average while those that were hospitalized 100% of the time (between January 2016 and April 2020) gained 4.7 kg/year. Other studies have reported that weight gain during a forensic hospital admission was highest in the first year (Long et al., 2014). Our study attempted to report on weight change during a forensic hospital admission. The amount of missing data would not allow for further exploration of weight change over time (e.g., occurring in the first 12 months) or whether the use of seclusion impacted that change.
There were two significant challenges that the researchers faced with collection of this data. Firstly, in the majority of cases there was no weight recorded at admission, making it difficult to report on weight change from this point. One postulated reason for the lack of data related to physical health measures and weight on admission, was that forensic patients are often placed into seclusion rooms at the point of admission due to risk concerns and therefore baseline measures and weights were not obtained. Secondly, there was no mandate to routinely collect data on weight, so that the most recent weight was from differing time points during an individual’s admission and may have been some months prior to the study. Additionally, there was no standardized procedure for monitoring or documenting weight, so weight measures were documented in various places (e.g., some wards kept their own physical health data in paper files, other patients had data documented in an electronic metabolic monitoring form and some patients had their weight documented in electronic progress notes from a multi-disciplinary team meeting). An electronic metabolic monitoring form has been available for all mental health patients in Queensland since approximately 2012 and its use has been evaluated (Benson et al., 2018). However, there was no regular use of the form in our study setting at the time of the study.
Implications for forensic services
A recent practice guideline for managing weight in adult secure service recommends that pre-admission physical health information is collected and that there is regular weight monitoring (Public Health England, 2021). The challenges we faced with collecting physical health data highlights the need for forensic services to implement formal processes for assessing and monitoring physical health and weight. This may include the use of an electronic metabolic monitoring form, which would allow the data to be available in one known place, increasing the likelihood for early detection and therefore early intervention for weight gain. There is scope for forensic services to consider further how measurements of waist circumference can be maximized to consider metabolic risk, document progress and improvements in physical health and how best to incorporate these in electronic monitoring forms. In addition to the monitoring of physical health and weight, there is a need for forensic services to consider how to prescribe, encourage, measure and document physical activity for patients.
The absence of a clinical tool to assess physical activity has been a barrier to the implementation of physical activity programs within mental health services (Rosenbaum et al., 2020). There are no current recommendations for Australian forensic services regarding the assessment, monitoring or documentation of physical activity. Methods of measuring physical activity include the use of self-report questionnaires (e.g., International Physical Activity Questionnaire, Simple Physical Activity Questionnaire), self-report activity diaries, direct observations and devices (e.g., accelerometers, pedometers). The questionnaire used in the current study, the International Physical Activity Questionnaire (IPAQ), was developed for assessing levels of total physical activity and is the most commonly used questionnaire for research purposes. Although accelerometers have been used in research studies to provide objective results, their use remains largely impractical for standard clinical care (Engh et al., 2019). The Exercise Vital Sign (EVS), a tool that uses self-reported information to determine whether individuals meet physical activity guidelines, has shown promising results when compared with accelerometry and has been incorporated into electronic medical records (Kuntz et al., 2021). Forensic services have a duty of care to identify patients not meeting current physical activity guidelines and to provide action. A tool such as the EVS would allow forensic services to identify patients not meeting physical activity guidelines, enable this information to be documented in a patients record and facilitate comparisons over time.
It is not enough to merely document low levels of physical activity or that an individual does not meet current physical activity guidelines. Forensic services need to consider how they respond to low levels of physical activity, how they monitor for improvements and how they address the unique barriers for this population and environment. Barriers previously identified in forensic settings include staff capacity, patient movement restrictions, personal autonomy, low motivation, sedation, and lack of equipment and space (Moss et al., 2022). A whole of service approach is needed from both executive and clinical staff that ensures careful planning and explicit scheduling of physical activity time and prioritization of both physical and mental health. Further training of staff is also required to increase confidence for the promotion and prescription of physical activity and improve attitudes toward physical activity as an effective treatment response for sedentary behavior (Kinnafick et al., 2018).
Forensic services also need to provide environments that support patient physical activity goals and interests and provide opportunities for patients to achieve recommended levels of physical activity. It is acknowledged that an inpatient forensic setting is a highly specialized environment that poses unique challenges with respect to implementing physical activities. Encouraging ward-based physical activity sessions can address issues related to movement restrictions. Forensic services should consider adapting factors that have been shown in non-forensic settings to increase attendance and physical activity levels including creating an environment of autonomy, competence and relatedness by organizing small groups for activities, having a qualified instructor, allowing patients to self-select exercise intensity, providing continuous encouragement and positive feedback throughout the sessions and following-up on those participants who missed sessions (Gomes et al., 2014; Vancampfort et al., 2015). This may further be achieved by allowing for the co-design of physical activity interventions, which recognizes the importance of lived experience of mental illness within a forensic setting. The authors acknowledge that while the focus on this paper is on physical activity, there are a number of other weight-loss options for patients including weight-loss medication and surgery.
The long-stay nature of hospitalizations for individuals under inpatient forensic mental health care allows for the implementation and evaluation of physical activity interventions. There is a need for longitudinal studies with larger sample sizes to identify relevant modifiable factors that can be targeted to encourage greater engagement in physical activity. Future research that considers patient perspectives is critical to understanding the barriers and enablers to physical activity in this setting. Furthermore, there is scope for forensic services to consider key performance indicators (KPIs) with regards to physical health care and activity for patients. Having KPIs will allow forensic services to undertake a benchmarking process, whereby forensic hospitals can be compared on a range of performance measures to facilitate quality improvement. Ultimately, the development of recommendations guiding practice for implementing physical activity into the routines of patients under forensic mental health care will assist forensic services in addressing the physical health needs of their patients.
Limitations
This study highlighted the significant challenge that researchers of forensic populations face with regards to data collection, related to both the availability and the reliability of the data. For our study, this limited the planned evaluation of weight change during inpatient forensic hospitalization. Another limitation was the use of self-reported physical activity levels. As outlined, despite the IPAQ-SF being validated for use in individuals with schizophrenia, it is not as accurate as objective measures.
The small target population limited our study size which likely impacted the finding of statistically significant results. The inferential analyses were exploratory in nature, and the small sample size may have also precluded identification of all the relationships that exist. Our target population was further limited by the researchers prioritizing a study that included the informed consent of the patient. The researchers, acknowledging that this population is a vulnerable group, aimed to protect the rights of patients with regards to their health information. The researchers also note that information related to diet, a significant contributor to overweight and obesity, was not collected for this particular study.
Conclusion
This study reports the significant relationship existing between comorbid medical illness and low physical activity levels for patients under forensic mental health care in a high secure inpatient service. It also highlights the need for, and importance of, the routine collection of standardized physical health and activity data for this population. There remains a lack of high-quality studies in this area, providing future researchers scope to consider how forensic services can improve the health and physical activity of individuals under their care and consider future recommendations. The long-stay nature of forensic mental health inpatient admissions provides both the opportunity and time for physical activity interventions to be designed, implemented and evaluated. Providing a range of opportunities for regular physical activity for this cohort will partly address the current gap in achieving contemporary international guidelines. To our knowledge the physical activity preferences for individuals under forensic mental health inpatient care has not been reported. By incorporating specialized assessments, collecting objective data, allowing choice of activities and supporting individuals to increase levels of physical activity, forensic services can assist individuals to improve their cardiovascular fitness which, in turn, reduces morbidity and mortality and improves overall health outcomes.
Footnotes
Acknowledgements
We thank the staff and patients at the High Secure Inpatient Service, The Park – Centre for Mental Health.
All authors listed contributed to the review article and are in agreement with the manuscript. The paper has not been published elsewhere and has not been submitted simultaneously for publication elsewhere.
Authors’ contributions
Katherine Moss: Conceptualization, Methodology, Data Curation, Writing – Original Draft. Carla Meurk: Methodology, Verification, Writing – Review and Editing. Megan Steele: Analysis and Interpretation, Writing – Review and Editing. Ed Heffernan: Writing – Review and Editing, Supervision.
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.