
Abstract
Mentally Disordered Offenders (MDOs) who have been declared not criminally responsible for their offense due to their mental condition should be admitted to settings with lowest possible level of security to support their social reintegration. In the context of the reorganization of care for MDOs in Belgium, we assessed the predictors and retrospective appropriateness of 3529 MDO admissions in 2017 according to security needs. Although there was a positive association between the security needs of MDOs and the level of security of the settings to which they were admitted, there was a gap between high and lower security levels. Medium-security settings made up 46% of all admissions, covering a variety of security need profiles. Half the sample of MDOs with high security needs was found in low- and medium-security settings, while a significant proportion of MDOs with low security needs was found in medium-security settings. Clinical characteristics predicted admissions more strongly than custodial characteristics. Decision-makers should refine criteria and procedures for MDOs’ care access. Indeed, the mixed results in relation to admission appropriateness in medium-security services may result from the lack of formal guidelines.
Introduction
Mentally disordered offenders (MDOs) are individuals with a psychiatric disorder or mental disability who have offended (Völlm et al., 2018a, 2018b). That definition may, however, apply to people in different situations. In this study, we specifically focus on people who have been declared not criminally responsible for their offense due to their mental condition. MDOs are people who primarily require psychiatric care but for whom access to appropriate care is challenging due to their criminal history. Although contemporary international quality standards in generic mental health care prioritize the delivery of care in the community as well as social rehabilitation and personal recovery (Anthony, 1993; Leamy et al., 2011; Leendertse et al., 2021; Skar-Fröding et al., 2021; Slade et al., 2015; Thornicroft & Bebbington, 1989), MDOs’ access to care is determined by security needs: those of the community, which must be protected from criminal offenses, as well as those of the MDOs, who need a secure environment for their own recovery process (Shepherd et al., 2016; Warburton, 2013). Recovery-oriented care aims to support the social inclusion of people with psychiatric conditions through independent living, employment, participation in social life, a decrease in the stigmatization of people with mental disorders, and helping people to build a meaningful life despite the impairments that are due to illness (Anthony, 1993). These principles, however, may generate tension when applied to forensic patients, as recovery-oriented objectives need to be balanced with the potential risk of violence or criminal recidivism on the part of MDOs (Aga et al., 2017; Vandevelde et al., 2017). In the criminal justice domain, recovery has been related to the concept of “desistance,” i.e., recovery from a criminal behavior (Best et al., 2017). These approaches have many shared components: both emphasize hope, the importance of social support, change in personal identity, and mark a shift toward a strength-based approach (Aga et al., 2017). Furthermore, the MDO him/herself needs to feel safe, which is a precondition for treatment effectiveness and for the success of any recovery process, from illness or from criminal behavior (Shepherd et al., 2016; Warburton, 2013).
In order to solve the potential tension between security needs and recovery-oriented psychiatric care, the guiding principle is that MDOs should be located within a setting with the lowest possible level of security, including care in the community, in order to maximize rehabilitation and the prospect of independent living (Reed, 1992; Völlm et al., 2018a). There is, however, no international consensus on how to adequately organize a comprehensive care system for MDOs that includes the full range of security levels for all security need profiles. Most countries have developed specific forensic psychiatric facilities, with the dual role of treating MDOs and providing the required security level (Dressing & Salize, 2006; Völlm et al., 2018a). Generally, forensic settings are usually preferred for those MDOs most likely to engage in criminal and violent behavior and for whom high security features are required, while MDOs who are less likely to engage in such behaviors may receive care in generic psychiatric services, i.e., those established for the general population with mental health care needs (Völlm et al., 2018a). Compared to generic services, specific forensic services face higher rates of violence by patients against other patients and staff (Broderick et al., 2015; Williams et al., 2020) and, therefore, have specific security features relating to the environment of the setting. These security features are sometimes referred to as the “Trinitarian Model of Therapeutic Security” (Bergman-Levy et al., 2010; Crichton, 2009), a model of stratified therapeutic security (Kennedy, 2002). Environmental security refers to structural interventions such as fenced perimeters, locked doors, and the presence of CCTV in a facility. Procedural security refers, for instance, to the regulation of visits or communication procedures between staff and residents. Relational security refers to technical elements such as staff-to-patient ratio, treatment plan reviews, the development of staff relation skills, and the quality of the relationships between staff and residents, e.g., in terms of trust (Collins & Davies, 2005; Crichton, 2009; Kennedy, 2002). Forensic psychiatric services can provide holistic assessments and specific treatments that address offending behaviors more systematically than general psychiatric services (Broderick et al., 2015; Hodgins, 2009; Völlm et al., 2018a). By contrast, generic psychiatric services are expected to provide care that is more oriented toward rehabilitation and social inclusion. It is, therefore, key to determine which MDOs would receive the most appropriate care in generic services and which MDOs would receive the most appropriate care in specific forensic services. Furthermore, the appropriateness of MDOs’ access to settings with the lowest security level required according to security needs is a key element of quality of care, and thus a key indicator of the performance of a care system for MDOs.
Belgium is an interesting case study; many of the issues that other countries are facing are concentrated in the Belgian system. The social-insurance, regulated-market care system provides extensive autonomy to social and care services and results in a highly fragmented system, which does not favor the development of a comprehensive approach for all MDOs’ security profiles. In this context, stratified security models are challenging to implement (De Pau et al., 2021) and care trajectories tend to result from an unstructured judgment process (Jeandarme et al., 2019). Until 2016, Belgium lacked appropriate psychiatric settings for MDOs, either specific or generic (Pesout & Pham, 2019). Only a few MDOs, therefore, had access to specific care services, while many were detained in prison, sometimes in the psychiatric annexes of prisons. Between 1998 and 2016, Belgium was condemned 23 times by the European Court of Human Rights due to its poor care access for prisoners, and its inhumane treatment of MDOs in particular. A mental health reform process has, however, been ongoing since 2011 (Nicaise et al., 2014). Part of the reform policy regarding care access for MDOs, which has been implemented since 2015 (Loi relative à l’internement des personnes, 2014; SPF Santé Publique, 2016), applies specifically to people who are considered not responsible for their offenses due to mental illness. In Belgium, these individuals are subjected to a so-called “internment measure” (To et al., 2015). In accordance with this legal measure, MDOs are asked to develop their own care project, which must include an application for a psychiatric care service chosen by the MDO, with support from the psychosocial service of the prison or residential care service where they reside. Although this measure may appear very person-centered, that aspect is counterbalanced by organizational factors (Aga et al., 2020; De Pau et al., 2020). The application has to be accepted by the service that is applied for (based on the service’s own inclusion and exclusion criteria) and then approved by a specific court, named the “Chambre de Protection Sociale”/“Kamer voor de Bescherming van de Maatschappij” (Chamber for the Protection of Society), which is made up of justice and care experts. The reform also aims to give MDOs access to care in generic settings whenever possible. For that purpose, some generic services have been receiving financial upgrades in order to encourage the admission of MDOs. Belgium, however, has no formal guidelines for MDOs’ care access. The key issue remains, therefore, of how to assess the security needs of MDOs in order to orient them toward the most appropriate setting. The absence of a clear process may make it difficult to match needs for security with MDOs’ secure admission. In the context of an evaluation of the reform policy, we therefore retrospectively assessed the appropriateness of MDOs’ access to several secure-level settings according to their security needs, and attempted to identify the clinical, social, and custodial determinants of access. This is the first time that the whole population of MDOs in Belgium has been surveyed across regions and care settings.
Material and methods
Study setting
This study was part of a larger program to evaluate the current Belgian reform of care delivery for MDOs, namely the For-Care research evaluation that was commissioned and funded by the Belgian Ministry of Public Health (2015–2019). Since 2015, the reform policy aimed to offer personalized and differentiated care by expanding residential accommodation, developing specific treatment offers for subgroups of MDOs, and endorsing the principle of recovery-oriented care delivery in the most appropriate security setting (Loi relative à l’internement des personnes, 2014; SPF Santé Publique, 2016). The policy was also intended to improve the flow of patients by facilitating transition between settings, and in particular transition toward generic mental-health care settings whenever possible, with the support of new liaison outreach teams.
Security levels
Though the reform policy did not include any explicit reference to security levels, its principles (i.e., the transition toward regular mental-health care settings when possible) implied the consideration of higher and lower security settings. In order to avoid differences in the professionals’ interpretation of what a security level was, we developed a classification based on four criteria: the authority or department responsible for organizing the service (justice, health, or welfare), the sources of funding, the generic care sector versus the specific care sector (Alford, 2002; Cartuyvels, 2017), and the features of the Trinitarian Model of therapeutic security (Crichton, 2009). The combination of these criteria resulted in five levels of security: low, medium, high, and highest security services, and liaison outreach teams. The liaison outreach teams were established by the reform in 2014 with a view to supporting generic services providing care for MDOs and facilitating their transition toward lower security levels, particularly MDOs who were detained in the psychiatric annexes of prisons (SPF Santé Publique, 2014). Low-security services mainly included generic mental health services and welfare services with few or no environmental, procedural, and relational security features, in which MDOs and generic users are mixed. Medium-security services were predominantly psychiatric services organized by the health sector but with specific features for forensic users, e.g., separate wards and specific personnel. High-security services were exclusively forensic psychiatric care services with high-security features. Finally, the highest-security services encompassed some specific settings organized by the department of Justice, as well as the prisons and psychiatric annexes of prisons. That level, however, was not included in this study, as those services were not under the authority of the public health department that commissioned the study. This classification and its methodology have been described in detail elsewhere (De Pau et al., 2021).
Data collection and rationale for the choice of instruments
As part of the reform policy, an experimental routine registration system was designed by the authorities and implemented across the country. The registration system included all the requests for admission that were made in 2017, either in forensic or in generic settings, with the exception of the services classified as “highest-security.” The registration system recorded the following categories: 1. Sociodemographic: gender and age, 2. Clinical indicators: psychiatric diagnosis categories including the presence of a mental disability; 3. Legal indicators: the MDOs legal status, the index offense type; 4. Use of services: the admission service and the length of stay at the time of registration. For the purpose of the study, the researchers also requested the inclusion of HoNOS-Secure (Dickens et al., 2007) in the registration system, in order to assess the security needs of MDOs. The “Health of the Nation Outcome Scale” (HoNOS)-Secure is composed of two subscales. The first scale is the “clinical scale” (Wing et al., 1998), which includes 12 items related to four domains: behavior, handicap, symptoms, and social functioning. It assesses a user’s level of psycho-social functioning. The second is the “security scale,” which includes 7 items related to three domains: the need for physical, relational, and procedural security measures (Dickens et al., 2010; Long et al., 2010). All items, in both the clinical and security scales, are 4-point Likert scales (0 = no problem, 4 = severe problem). Thus, the clinical scale returns a score ranging from 0 to 48 (highest severity), while the security scale returns a score ranging from 0 to 28 (highest need for security). The reliability and validity of HoNOS-Secure is widely established in the literature (Dickens et al., 2010; Liddiard et al., 2019). With the help of HoNOS-Secure, we aimed to retrospectively assess whether MDOs had accessed services of the appropriate security level according to their security needs. Indeed, in accordance with the procedure for accessing care services, no structured triage had been applied prospectively.
The HoNOS-Secure was selected on the basis of the literature review of routine outcome measures for forensic mental health services by Shinkfield and Ogloff (2014). We looked for an instrument that, in addition to scientific validity and robustness, fulfilled several practical criteria. It needed to be easy to use, not time consuming, with no requirement for extensive training. The instrument also needed to be suitable for a number of different disciplines as it had to be used by different professional profiles. It also had to be free for use and available in both Belgian national languages, Dutch and French. Two instruments were recommended by Shinkfield and Ogloff: the DUNDRUM quartet of instruments (O’Dwyer et al., 2011) and HoNOS-Secure (Dickens et al., 2007, 2010; Liddiard et al., 2019). DUNDRUM was the most complete in terms of admission triage security, need for security assessment, adherence to treatment, and recovery assessment (Flynn et al., 2011; Freestone et al., 2015; Moynihan et al., 2018). DUNDRUM, however, required formal training prior to use, and its recovery module required face-to-face interviews with the users, which was not feasible in this study (Shinkfield & Ogloff, 2014). At the time that the study was carried out, the DUNDRUM was not yet validated for use in Belgian settings (Habets et al., 2019). HoNOS-Secure, on the other hand, only required minimal training, took less time to use and was easier to implement, and was more widely used internationally (Keulen-de Vos & Schepers, 2016; Shinkfield & Ogloff, 2014). Furthermore, HoNOS had been used in the evaluation of the generic psychiatry reform policy, which meant that scores from the clinical scale were available, measured against a benchmark of 2,000 adults with severe mental illness who were recruited across the country in all generic service types (Lorant et al., 2016, 2017, 2019). HoNOS-Secure appeared, therefore, to be adequate to assess, retrospectively, whether MDOs in Belgium were accessing services at the appropriate security level and whether the use of an instrument to support future formal triage procedures was feasible.
Statistical analysis
First, global descriptive analyses and F or t-tests were used to characterize the population across secure settings, including security needs. Then, the appropriateness of MDO admissions in security levels according to security needs was assessed: a ROC curve analysis was used to examine the concordance of the HoNOS-Secure scores and their predictive property on the security level of admission, and multinomial logistic regressions were performed to measure the effect of security needs on the security level of admission. Finally, predictors of admission to the different security levels were assessed using multinomial logistic regressions, controlling for the MDOs’ clinical, social, and custodial characteristics. All analyses were carried out using SAS 9.3 for Windows.
Results
Descriptive statistics on MDOs are presented in Table 1. In total, 3529 admissions of MDOs were registered in 2017 in 70 different services across the country. MDOs may have been admitted several times during the year. As the data were anonymized, we could not clearly identify the number of individual MDOs who applied for a place in a psychiatric service. By cross-tabulating individual characteristics such as gender and sex, however, we estimated that a minimum of 2518 and a maximum of 3009 different MDOs were registered. Due to the experimental registration system, only voluntarily participating services completed the HoNOS section. The HoNOS-Secure section of the registration system was completed for 1175 (33.3%) MDO admissions. Participation in the use of the HoNOS-Secure instrument was, therefore, limited.
Descriptive statistics of MDOs’ clinical, social, and custodial characteristics per security level, Belgium, 2017.
a χ 2 test, b F-test.
*p ≤ 0.05, **p ≤ 0.01, ***p <.001.
§The total number is the number of admissions of MDOs registered in 2017 in Belgium. It may happen that the number of different MDOs is slightly different, as one MDO may have been admitted to different services during the year.
Of all the MDO admissions recorded, 90% were of male MDOs with an average age of 43 years (std = 11.6). Admissions were mostly of MDOs with psychotic (52.3%), substance-related (42.2%), and personality disorders other than psychopathy (44%). Twenty-one percent were of MDOs with intellectual disabilities. The majority of the MDOs registered were on conditional release (76.5%). The most common index offense (i.e., the offense that led to the internment measure), was assault and battery (32.4%), followed by theft (21.1%) and harm to persons (18.8%).
In regard to the different security levels, 16% of MDO admissions were registered in low-security settings, 45% in medium-security settings, and 2% in high-security settings. In addition, 37% of MDO admissions were registered by the outreach teams. Several individual characteristics differed significantly between security levels. In particular, the proportion of admissions of MDOs with personality disorders increased according to the level of security: 32.6% in low-security, 57.1% in medium-security, and 84.5% in high-security settings. Likewise, there were higher proportions of admissions for MDOs with developmental, sexual-related disorders, and mental disability in high-security settings and, overall, MDOs in high-security settings had a higher number of concomitant psychiatric disorders (mean = 6.7, std = 4.6). MDO admissions in high security settings, however, were significantly less related to psychotic disorders and substance-related disorders than in lower security settings. Most admissions to high-security settings were of MDOs under a compulsory placement order, while most MDOs in low- and medium-security settings were on conditional release. Interestingly, 30.5% of admissions managed by the newly established outreach teams were of MDOs detained in prisons. In terms of offenses, a higher proportion of MDO admissions in high-security settings were related to murders (27.6%), while thefts were more common in medium-security settings. The number of concomitant offenses was slightly lower in low-security settings (1.5 std = 1.0)
Overall, the 1175 MDO admissions for which the HoNOS-Secure section was recorded had an average score of 10.8 (±6.4) on the clinical subscale and an average score of 6.4 (±4.9) (median = 6) on the security subscale (see Table 2). The average score on the security subscale increased in accordance with increases in the security level of the settings and the average security subscale score for MDOs registered by the outreach teams was between low and medium. The HoNOS security subscale score was 6.1 (±4.7) for outreach teams, 4.7 (±4.3) for low-security, 7.5 (±4.8) for medium-security, and 18 (±3.6) for high-security settings. There was, therefore, a major cutoff between the MDOs’ security need score in high-security settings and in the other levels. As shown in Table 2, the F-test had a value of 59.5 (p < 0.001), indicating that the security level was associated with statistically different HoNOS-Secure scores. We also computed a contrast test comparing the highest security level to the other three levels and found a significant contrast test with a chi-square of 115.28 (p < 0.001).
Available HoNOS-Secure scores (clinical and security subscales) of MDOs admitted to care services per level of security, Belgium, 2017.
***p <.001.
Overall, 94% of the scores for the security subscale were below 15, corresponding to a low to moderate security need profile (see Figure 1). A significant proportion of MDO admissions with such scores occurred in medium-security settings (41.2%). Eleven percent of MDOs with a security need score lower than 4 were, however, admitted in medium-security settings, while 3% of MDOs with a security need score higher than 10 were admitted to low-security settings. Furthermore, although only 6% of MDOs had a security need score higher than 15, 50% of them were admitted to medium-security settings and 10% to low-security settings.
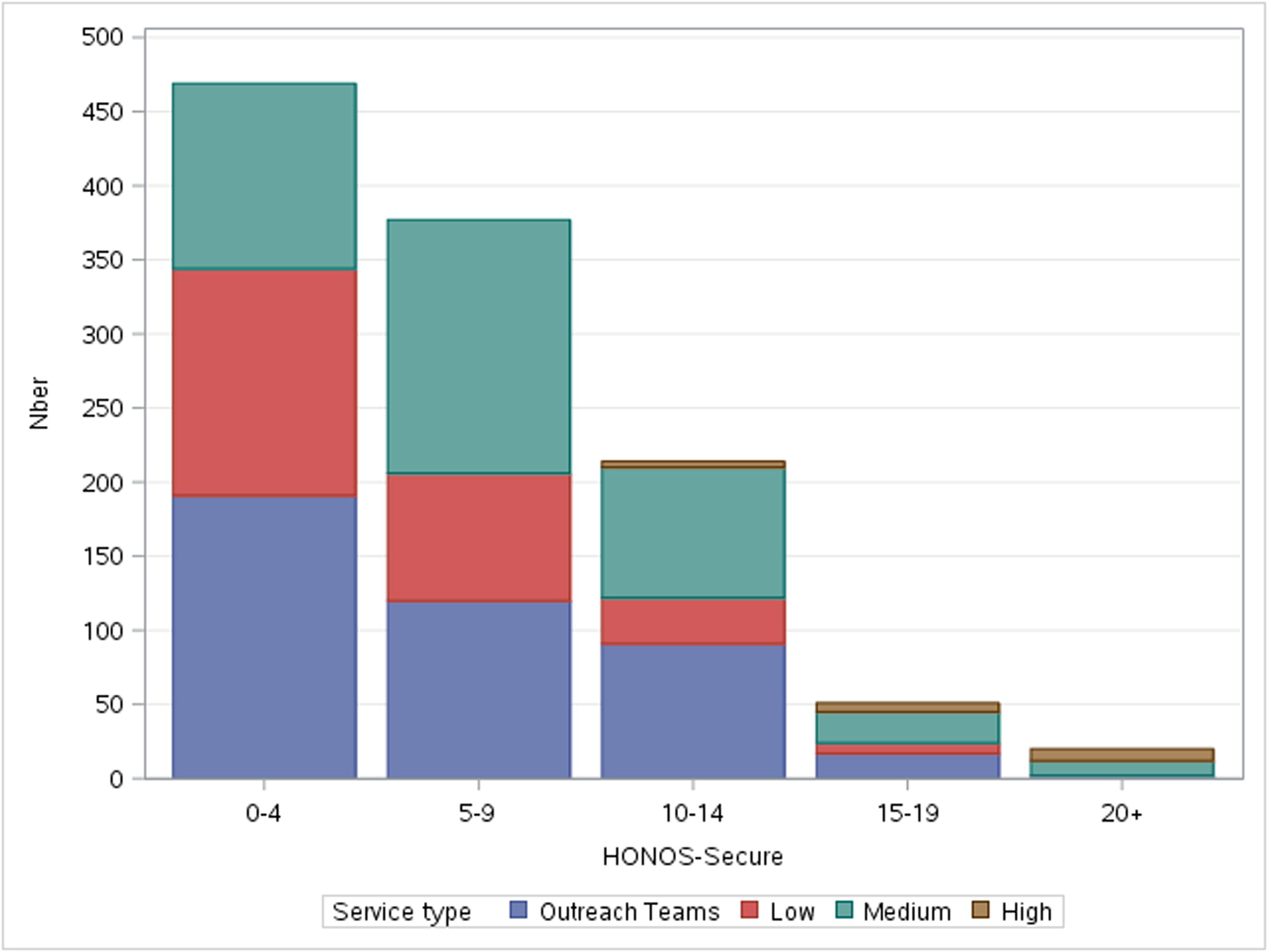
Needs for security within secure settings and outreach teams, 2017, Belgium (n = 1131).
Despite these disparities, the ROC curve analysis showed that the HoNOS-Secure security subscale had excellent predictive power for admissions to high-security settings (96%) with a Somers’ D score of 0.927. The average predictive power was lower for admissions to medium- (61%) and low-security (66%) settings. This result was consistent with the result of the odds ratios of admissions to settings with different security levels according to security needs calculated with logistic regressions controlling for MDOs’ characteristics: without additional factors, the odds ratio from low to medium-high security was 1.16 (CI 95%, 1.12–1.21, p < 0.001), and the odds ratio from low-medium to high security was 1.44 (CI 95%, 1.30–1.60, p < 0.001). The second odds ratio indicates a higher consistency of the HoNOS-Secure security subscale score with the security needs of MDOs in settings with higher security levels.
Results on the HoNOS-Secure security subscale measures remained statistically significant after controlling for sociodemographic, clinical, and custodial individual characteristics in the bivariate and multivariate multinomial regressions presented in Table 3. As indicated in the table, the OR in the multivariate column were adjusted for all the variables displayed in the table.
Predictors of MDOs’ admission according to security levels, OR from bivariate and multivariate multinomial regressions, Belgium, 2017 (n = 575).
*p ≤ 0.05, **p ≤ 0.001, ***p < 0.0001.
aMultivariate models were controlled for all the variables displayed in the table.
Some MDOs’ individual, clinical, and custodial characteristics statistically predicted the level of security of admission. In the multinomial regression, a diagnosis of personality disorder (other than psychopathy) was a strong predictor of admission at a higher level of security (OR = 3.17, p < 0.0001), as was theft, but to a lesser extent (OR = 1.69, p ≤ 0.05). By contrast, other characteristics were negatively correlated with the level of security: having a higher HoNOS score on the clinical subscale (OR= 0.90, p < 0.0001), having a neurocognitive disorder (OR = 0.06, p ≤ 0.05), having a diagnosis of psychopathy (OR = 0.11, p ≤ 0.001), and having committed a substance-related offense (OR= 0.45, p ≤ 0.05) were all predictors of an admission at a lower level of security.
Discussion
Appropriateness of care access according to security needs
Overall, there was a positive association between the security needs of MDOs as measured with the HoNOS-Secure and the level of security of the settings to which they were admitted, despite the lack of formal guidelines and procedures for assessing MDOs’ security needs. MDO admissions to services according to security levels were, therefore, appropriate on average. In particular, the association was stronger for admissions to high-security settings. Medium-security settings, however, made up 46% of all admissions. These settings appeared to be catch-all services, covering a variety of MDOs’ security need profiles, including low and high levels of security needs. On the one hand, there was an overlap of the MDOs’ security need scores between the populations in low-, medium-security settings, and those in contact with liaison outreach teams. On the other hand, half the sample of MDOs with high security needs was found in low- and medium-security settings, while a significant proportion of MDOs with low security needs was found in medium-security settings. Some MDOs with moderate needs were also found in low-security settings. Low- and medium-security settings, therefore, seemed not to target their specific MDOs’ profiles with sufficient accuracy. Despite the overall trend, therefore, MDOs were not always admitted to services of the appropriate security level for their security needs.
Furthermore, the newly established liaison outreach teams were involved in 37% of the admissions, of which one third concerned MDOs in detention, and 10% concerned MDOs under a compulsory placement order. A substantial effort was, therefore, made by these teams to help detained MDOs and MDOs under a compulsory placement order to access care in lower-security settings. This kind of intervention is consistent with the declared objectives of those teams (SPF Santé Publique, 2014). Although the profile of MDOs addressed by outreach teams is similar to that of MDOs found in low- and medium-security settings, it is unclear whether outreach teams could and should also address the orientation of MDOs with higher security needs toward high-security settings. A clarification of their role in this respect would be welcomed.
The fact that MDOs’ access to care was globally appropriate according to security needs, despite the lack of formal procedures, suggests that the individual professionals involved have a good level of expertise. The results revealed, however, some inconsistencies, particularly regarding the gap between the profile of MDOs admitted to high-security settings and the profile of MDOs admitted to all other security levels. Professional expertise may prove to be insufficient for correctly identifying the security needs of MDOs with lower security need profiles. More fundamentally, however, this situation seemed to result from several organizational mechanisms that need to be refined and adapted, including the legal criteria used to allocate internment status, i.e., Belgian legal not criminally responsible MDO status, triage procedures (or lack thereof), and criteria for accessing to care services, such as the availability of places in services. As part of the reform policy, the legal conditions and procedures for internment were modified and efforts were made to improve the availability of places and services. Procedures relating to triage and access to services were, however, left unchanged. Within the framework of the ongoing reform policy, medium-security services were those receiving a financial upgrade for implementing the reform program (SPF Santé Publique, 2016) and, in the absence of formal guidelines for referral, may have appeared to be the only available solution for forensic psychiatric care in the view of many professionals, rather than considering the possibility of using generic, lower-security mental health services. This may have resulted in an increase of MDO admissions to medium-security facilities. Moreover, the lack of sufficient forensic psychiatry settings overall and, thus, the scarcity of available places for MDOs, may have determined the care orientation of MDOs to a greater extent than the assessment of their individual needs. This process is reinforced by the application procedure for accessing care services that is required of MDOs. With the exception of those detained or under a compulsory placement order, MDOs are requested to apply to access care services on their own; services are free to accept or refuse the application, and the application must then be approved by the court. This procedure slows down access to services further reduces the number of available places (De Pau et al., 2020). The fact that, within the Belgian healthcare system, services, including in forensic psychiatry, have extensive autonomy to decide and apply their own inclusion and exclusion criteria (Nicaise et al., 2014, 2020) makes the design of a consistent care trajectory more complex.
Individual determinants of MDOs’ access to care
In some respects, the social, clinical, and legal characteristics of MDOs reflect a certain continuum of profiles across security levels. MDOs admitted to high-security settings had more comorbidities and concomitant offenses than MDOs in lower-security settings. In the multinomial regression, some predictors of admission at a higher level of security were detected: having a diagnosis of personality disorder (though not a psychopathic personality disorder), and, to a lesser extent, theft, predicted admission at a higher level of security. By contrast, having a neurocognitive disorder or having committed a substance-related offense were predictors of admission at a lower level of security, as was having a psychopathic personality disorder. Being male was also a significant predictor of admission to lower-security settings. Some of these predictors, particularly the two last-named findings, might appear counterintuitive or inconsistent with the literature. Regarding the unexpected inverted associations found between psychopathic personality or substance-related offenses and high-security settings, the explanation is probably to be found in the exclusion criteria of one specific high-security setting, which explicitly excludes patients with such characteristics (Jeandarme et al., 2015). The effect of one service is considerable given the small sample size of MDO admissions in high-security settings. Likewise, the effect of gender is probably related to a sampling bias; the vast majority of MDOs are male, but there is one specific high-security unit dedicated to female MDOs. That unit has probably provoked an overrepresentation of female MDOs in the high-security subgroup. It was not within the scope of our study to examine the inclusion or exclusion criteria of individual services. Our findings may suggest, however, that criteria should be set at the level of care systems in order to ensure comprehensive care supply for all MDO profiles.
There have been few large international studies that would allow us to compare the characteristics of Belgian MDOs with an international benchmark (Nicholls & Goossens, 2017). This first national description of MDOs in Belgium seems, however, to be consistent with what is found in other Western countries. Indeed, the most common diagnoses found in MDOs are psychotic spectrum disorders, personality disorders, substance-misuse disorders, and dual diagnoses (Crocker et al., 2015; Nicholls & Goossens, 2017). Similarly, the most common offenses registered are related to harm to persons and assaults and property offenses, while far fewer relate to extremely violent behaviors such as murders and sexual offenses (Crocker et al., 2015). With the exception of the unexpected effects of gender, psychopathic personality disorders, and substance-related offenses, the remaining predictors of admission are consistent with the literature. For instance, personality disorders are a predictor of admission at a higher security level. The risk of violent behavior and re-offending is up to three times higher for individuals with such disorders than individuals without such disorders (Bonta et al., 2014; Völlm et al., 2018a). Theft, however, which is not a major offense, predicted admission to a higher-security setting.
Several clinical and custodial characteristics were significantly associated with security levels in univariate regressions. Those characteristics, however, were no more significant in the multivariate regression. This finding implies that some predictors are linked to each other and, therefore, that the predictors that remain significant in the multinomial regression have a greater effect on MDO admissions. Globally, in the univariate regressions, clinical predictors (e.g., having a personality or developmental disorder), have a stronger effect on the security level of admission then legal predictors (e.g., index offense and legal status), security needs, and severity of symptoms. Despite the fact that care admissions are driven more by clinical than by legal considerations, one may still wonder whether professionals, in particular clinicians, are sufficiently aware and trained for assessing security needs.
Limitations
The services classified as highest security, i.e., the psychiatric annexes of prisons and the newly established Forensic Psychiatric Centers, did not participate in the registration system; this means that some MDOs were not included in the sample. The sample included 73.5% to 87.9% of the 3424 MDOs who were legally registered in 2017 (Chambre des Représentants de Belgique, 2018). Precise figures were difficult to obtain, but estimates indicate that there were about 700 MDOs detained in 2017 and the capacity of the highest-security services organized by the Justice department was about 470 places. It is likely, therefore, that about 60% of the MDOs not included in our study were in prison, while the remaining 40% were in the services organized by the Justice department. It is probable that the MDOs in settings of the highest-security level had committed the most serious offenses and had high security needs, although it is unclear how those needs were assessed. It is likely that individual confounding factors (e.g., social situation or behavior) and organizational factors (e.g. the region or the availability of services) played a role. As a consequence, it is likely that, overall, the security needs might be underestimated, and that some predictors lack accuracy, in particular for MDOs in high-security settings.
We also indicated that some counterintuitive results might be related to some specific high-security services. This is, however, the first global description of almost the entire population of MDOs in Belgium, across regions and service types. Furthermore, due to the registration system being experimental, HoNOS-Secure scores were only provided for about one third of the sample. This study was part of a larger evaluation program, so we performed some additional analyses to assess data quality and the feasibility of the registration system. The subsample of MDOs for whom the HoNOS scores were available were compared with the subsample of MDOs for whom they were not available (see Table S1 in the supplementary material). There were a few significant differences: the proportion of admissions for MDOs with mood or sexual disorders was higher in the sample with an available HoNOS assessment, and the proportion of admissions for MDOs with developmental disorders was lower. There were also fewer MDOs who had committed theft, and more female MDOs in the sample with an available HoNOS assessment. No other variables were significantly different. Furthermore, there were more missing HoNOS scores in medium-security settings than in low- and high-security settings. It is likely, therefore, that mood and sexual disorders are somewhat overrepresented and that developmental disorders are slightly underrepresented in the study sample. We also assessed the internal consistency of the HoNOS clinical and security subscales. The Cronbach’s alpha of the two scales were 0.86 and 0.88 respectively, indicating excellent consistency. Furthermore, the HoNOS clinical score was available twice (two admissions to different services for one single individual at two moments in time) for 254 MDOs, while the HoNOS security score was available twice for 293 MDOs. The correlation between clinical scores was 0.91 (p < 0.0001) and the correlation between security scores was 0.88 (p < 0.0001). All these elements indicate the high level of reliability of the measurements. Further longitudinal research would nonetheless be needed to assess the capacity of HoNOS-Secure to measure changes in security needs over the course of an MDO’s care pathway. It must also be noted that this was a retrospective study and professionals who provided the HoNOS scores were not blinded to security level allocation. Authorities should, therefore, support an evaluation to ensure robust, prospective triage and the allocation of MDOs to different security levels.
Finally, the definition and criteria to determine security levels were based on an experimental design that had not been validated by the authorities. There was no formal definition of security levels in Belgian policy and legislation. The adequacy of care admission to services according to security needs must, therefore, be interpreted with caution. The definition of security levels should be refined and validated (De Pau et al., 2021). In particular, further research should address the longitudinal component of the care trajectory of MDOs, i.e., the capacity of the care system to decrease the MDO’s security needs and, consequently, the consistency of the MDO’s care trajectory across services with different security levels. That kind of assessment could not be carried out within the experimental registration system designed as part of the reform policy. Authorities were recommended, however, to proceed with the development of the registration system, i.e., its refinement and implementation in routine practice, so that a longitudinal study on the care trajectories of MDOs might be carried out in the future.
Conclusion
The analysis of MDO admissions to services is an opportunity to guide authorities toward optimal service planning and organization (Crichton, 2009). The diversity of MDO profiles found in medium-security settings indicates that guidelines for the inclusion of MDOs and the therapeutic input of these services need to be refined by authorities. Likewise, guidelines and procedures for referrals between services are needed. Those guidelines should take into account the security needs of MDOs as well as their experience and expectations in relation to their care pathway and social reintegration (De Pau et al., 2020). The definition of objectives and the process of a full care trajectory oriented toward person-centered care in forensic psychiatry still need to be developed (Völlm et al., 2018a).
Footnotes
Acknowledgement
This study was part of the interuniversity research project: “For-Care, a realist evaluation of the Belgian policy reform program for mentally-ill offenders”. The study was funded by a grant from the Belgian Federal Public Service on Health, Food Chain Safety, and Environment (2016-2019), Grant No. [PSY/VL/03/2016/256117]. This study was carried out by the Vrije Universiteit Brussel (Pr. Mark Leys), the Institute of Health and Society (IRSS) of the Université catholique de Louvain (Pr. Vincent Lorant, Dr. Pablo Nicaise, Delphine Bourmorck), the Institute for International Research on Criminal Policy (IRCP) of the Universiteit Gent (Pr. Freya Vander Laenen, Pr. Wouter Vanderplaaschen, Marjolein De Pau, Sara Rowaert, Anouk Mertens), and the Université de Liège (Pr. Frédéric Schoenaers, Coralie Darcis, Sophie Thunus). We are grateful to the members of the Strategic Committee on Internment and Interment Center, who collaborated and supported the study and designed the experimental routine registration system. Data were provided by professionals across all the services. Their contribution was greatly appreciated.
Data availability statement
The dataset used for this study is property of the Strategic Committee on Internment and Interment Center, Belgian Federal Public Service on Health, Food Chain Safety, and Environment. Requests to access the datasets should be directed to Vincent Lefebvre (
Declaration of interest
The authors report no conflict of interest.