
Abstract
It has been suggested that psychopathy and borderline personality disorder (BPD) are associated and that they could be differently gendered variants of the same underlying phenotype. This study explored gender-specific perceptions of the Comprehensive Assessment of Psychopathic Personality (CAPP) and the Comprehensive Assessment of Borderline Personality (CABP). Correctional staff (n = 87) were asked to rate the prototypicality of these models for women and men with psychopathy. The results provide further support for the CAPP model as a promising conceptualization of psychopathy. Findings show few gender differences and lend support to psychopathy and BPD as overlapping constructs.
Introduction
Research on psychopathy in women is sparse and based on the assumption that psychopathic features manifest equally across gender (Forouzan & Cooke, 2005; Verona & Vitale, 2006). It has been suggested, however, that there might be gender differences in the behavioral expression of psychopathy, indicating that psychopathic women tend to show more emotional instability, verbal abuse, and manipulation as well as aggression in their family relations, while psychopathic men display more criminal behavior and instrumental violence (Cale & Lilienfeld, 2002b; de Vogel & Lancel, 2016; Forouzan & Cooke, 2005; Logan, 2009; Verona & Vitale, 2006).
Operationalizing and measuring the psychopathy construct
Psychopathy or psychopathic personality disorder (PPD) encompasses disturbances in affective and interpersonal functioning, often in combination with impulsive and antisocial behavior. A variant of the psychopathy construct is recognized in the diagnostic manual DSM-5, in which it is conceptualized as antisocial personality disorder (ASPD; American Psychiatric Association, 2013). However, this operationalization has met with criticism as it relies on antisocial and criminal behavior and does not adequately capture relevant personality traits (Skeem, Polaschek, Patrick, & Lilienfeld, 2011). Thus, in a forensic psychiatric context, clinicians and researchers generally advocate a more personality-based operationalization of psychopathy. Currently, the most widely used assessment method is the Psychopathy Checklist Revised (PCL-R; Hare, 2003). The PCL-R conceptualization of psychopathy has been criticized during recent years. This discussion began with Cooke and colleagues debating the relevance of antisocial and criminal behavior for the psychopathy construct (Cooke, Michie, Hart, & Clark, 2004; Skeem & Cooke, 2010), although this view has been retorted by Hare and colleagues (Hare & Neumann, 2010; Neumann, Vitacco, Hare, & Wupperman, 2005). Another criticism is that the PCL-R items are scored based on a life-time prevalence, thus making it a static measure not suitable for the capture of fluctuations or remission in symptom burden (Hart & Cook, 2012). Furthermore, concern has been raised as to how well suited the PCL-R is for the assessment of psychopathy in women (Forouzan & Cooke, 2005; Verona & Vitale, 2006).
Psychopathy in women
PCL-R assessed psychopathy has been demonstrated to have a lower prevalence in women (e.g., Beryl, Chou, & Völlm, 2014; Verona & Vitale, 2006; Wynn, Hoiseth, & Pettersen, 2012). It is currently unclear, however, whether this reflects an actual lower prevalence in women or merely that the PCL-R does not adequately measure psychopathy in women. Even though there is evidence that the PCL-R is a valid and reliable measure of psychopathy in women, the literature is not entirely conclusive (Skeem et al., 2011). Previous studies have indicated that PCL-R factor structure as well as item expression varies to some degree across gender (Beryl et al., 2014; Dolan & Völlm, 2009). More specifically, items that reflect antisocial behavior (i.e., “criminal versatility”, “juvenile delinquency”, “revocation of conditional release” and “failure to accept responsibility”) are argued to be less applicable to women with psychopathy, while other items (i.e., “promiscuity”) could be more strongly related to psychopathy in women than in men (Dolan & Völlm, 2009). This might be explained by women being less likely to commit crimes compared to men, thus expressing their deviant emotional and interpersonal traits in other areas, for example using their sexuality to exploit and manipulate others. As discussed by Forouzan and Cooke (2005), the claim that “The PCL-R functioned much the same […], with only small differences at the lower and upper levels of the psychopathy trait” (Hare, 2003, p. 74), is problematic, as it is indeed the individuals in the upper levels of the distribution that the instrument is primarily meant to identify. In summary, knowledge is needed on whether the same degree of psychopathic traits renders an equal PCL-R score across gender (Forouzan & Cooke, 2005). Some researchers have proposed that the PCL-R cut-off score needs to be adjusted for clinical use in women (de Vogel, de Vries Robbé, van Kalmthout, & Place, 2014). The proposed gender adjusted cut-off score for the PCL-R (30 for men and 23 for women; de Vogel et al., 2014) was recently used in a study in a secure setting (de Vogel & Lancel, 2016). Even though the prevalence rates were similar (19.3% for women, 20.8% for men), the results demonstrated gender differences in comorbid personality disorders. Psychopathic women were more often diagnosed with borderline personality disorder (BPD), while psychopathic men were more often diagnosed with ASPD (de Vogel & Lancel, 2016). This procedure, however, does not address the concern of metric variance across gender – more specifically the concern that the items might not be equally discriminative for psychopathy in women and that men and might not fit the same structure. From this research, it is therefore not possible to draw clear conclusions on whether the findings are due to a gender bias of the PCL-R, which a mere adjustment of the cut-off cannot accommodate, or whether it reflects meaningful gender differences in the behavioral expression of psychopathic traits.
Potential gender bias in the assessment of psychopathy and emotional instability
In line with the findings of higher prevalence rates for the PCL-R in men, it has previously been reported that ASPD is more prevalent in men, while BPD is more prevalent in women (APA, 2013). It has been proposed that the different gender prevalence rates could be explained to some degree by psychopathy and BPD being differently gendered variants of the same underlying phenotype, characterized by impulsivity, emotional disturbances and behavior problems (Sprague, Javdani, Sadeh, Newman, & Verona, 2012; Viljoen et al., 2015). There are however contradictory findings from epidemiological research indicating that BPD is equally common among men and women in the normal population, although the comorbidity rate of ASPD is higher in men with BPD (Grant et al., 2008). This finding might point to a gender bias in the clinical assessment of these diagnoses, that is that men are more likely to be identified as antisocial or psychopathic, and women are more likely to be identified as being emotionally unstable or histrionic (see Cale & Lilienfeld, 2002a for a review).
The CAPP model of psychopathy
In the wake of the criticism concerning assessment methods of psychopathy, the Comprehensive Assessment of Psychopathic Personality (CAPP; Cooke, Hart, Logan, & Michie, 2012) was formulated as an alternative conceptual model of psychopathy. The objective was to shift the focus from the assessment and diagnosis of psychopathy to the reevaluation of the core construct, thus revitalizing the research field of psychopathy. Furthermore, the CAPP was developed as a dynamic measure to be able to assess fluctuation and remission on psychopathic personality traits, which is prerequisite for the evaluation of treatment. The CAPP is developed from a bottom-up perspective based on a thorough review of clinical and research literature along with interviews with other experts in the field and it encompasses an inventory of symptoms indicative of psychopathy. The CAPP model is based on the lexical hypothesis of normal personality (Goldberg, 1993), implying that symptoms of personality, including personality disorders, can be described in words of common language as opposed to technical jargon. The developers further reasoned that symptoms of personality should reflect personality deviance rather than social or cultural deviance, meaning that it is not relevant to describe personality disorders through specific norm-breaking behaviors. In contrast to the PCL-R, the CAPP model places a greater emphasis on affective and interpersonal traits of psychopathy, without reliance on explicit deviant and antisocial behavior (Cooke et al., 2012). This conceptualization of psychopathy could facilitate more gender-neutral assessments that enable clinicians to identify problematic personality traits with various behavioral manifestations in men as well as in women. Several international studies have used prototypicality analysis to investigate to what extent CAPP symptoms and domains are perceived to be indicative of psychopathy and found support for the validity of the CAPP model across translations (Florez et al., 2015; Hoff et al., 2014; Hoff, Rypdal, Mykletun, & Cooke, 2012; Kreis, Cooke, Michie, Hoff, & Logan, 2012; Smith, Edens, Clark, & Rulseh, 2014; Sörman et al., 2014).
CAPP and gender
A previous study that investigated gender prototypicality of the CAPP model (Kreis & Cooke, 2011) showed that the majority of CAPP symptoms were perceived as more prototypical of men than women. The results indicated that participants perceived psychopathic women as more manipulative and emotionally unstable, whereas psychopathic men were perceived as more self-aggrandizing, disruptive, and aggressive. Nonetheless, the results indicated that the CAPP conceptualization of psychopathy reflects a similar personality profile in men and women, even though the symptoms might be more pronounced in men (Kreis & Cooke, 2011). In a more recent study, Sellbom and colleagues (Sellbom, Cooke, & Hart, 2015) investigated the internal structure of the CAPP model with self-reports. They found that even though men scored significantly higher on 32 of the 33 symptoms, the structure was generally invariant across genders.
Cook and colleagues formulated a corresponding model for BPD, the Comprehensive Assessment of Borderline Personality Disorder (CAPB), which was developed according to the same strategy as the CAPP with the intention to enable the investigation of the theoretical overlap of PPD and BPD and to assess the symptoms of BPD (Cook et al., 2013). Given that the CABP model is newly developed, there is limited empirical support for the model to date. To the best of our knowledge there is only one published study (Viljoen et al., 2015). In this prototypicality study that involved both the CAPP and the CABP models, participants perceived CAPP symptoms as more typical of men, while CABP symptoms were considered more typical of women, regardless of whether participants rated the symptoms vis-à-vis an individual with psychopathy or BPD. The results gave support for each disorder being gendered, but there was no clear support for psychopathy and BPD being differently gendered behavioral variants of a common underlying disorder (Viljoen et al., 2015).
Using prototypicality methodology to investigate the validity of psychological constructs
The investigation of content validity is a crucial first step when developing a new model or instrument to ensure that the model captures the construct of interest in a meaningful way. Failure to do so weakens the empirical basis of the instrument. As the CAPP is still under evaluation, the use of prototypicality methodology to identify stronger and weaker items is important to determine whether the model captures what is thought of as typical of psychopathy (see Kreis et al., 2012 for a thorough discussion). Previous prototypicality studies of the CAPP model have used mental health professionals, forensic experts, jurors as well as community members in general (Florez et al., 2015; Hoff et al., 2014, 2012; Kreis & Cooke, 2011; Kreis et al., 2012; Smith et al., 2014; Sörman et al., 2014; Viljoen et al., 2015), to investigate how the psychopathy construct is perceived by participants with varying degrees of training and experience with psychopathy. As the CAPP model is based on the assumption that personality disorders reflect deviance from basic-level personality features that are encoded in natural language (Cooke et al., 2012), it is of special value to examine the perceptions of the psychopathy construct in different samples, for example, forensic experts as well as lay persons (Hoff et al., 2012).
Research with prototype methodology has demonstrated the usefulness of correctional professionals, lay persons, and inmates, for the identification of core features of ASPD and psychopathy (Cruise, Colwell, Lyons, & Baker, 2003; Rogers, Dion, & Lynett, 1992; Rogers, Salekin, Sewell, & Cruise, 2000). As discussed in these studies, the use of non-experts (i.e., correctional professionals or inmates) with extensive first-hand experience of offenders with psychopathy can be a useful complement to the use of mental health experts for several reasons. First, mental health experts risk being theory-bound in their perceptions (e.g., adhere to the PCL-R model). The use of non-experts is a way to counterbalance this problem, thus broadening the evidence base of the construct (Rogers et al., 1992). Additionally, correctional professionals have more close-up contact with psychopathic individuals and more opportunity to observe and interact with them in a different manner than mental health experts (Cruise et al., 2003).
Objectives
In the current study, we chose to use correctional officers as participants since they have vast experience in interacting with offenders with varying degrees of psychopathy. The aim of the study was to investigate whether correctional staff perceived the symptoms of the CAPP to be indicative of psychopathy in men and women. An additional aim was to investigate whether there are gender differences in what is considered typical of psychopathy. The CABP model was included in the survey to further elucidate the validity of the CAPP model by investigating whether the models could be clearly distinguished from each other. Furthermore, we wanted to investigate whether the CAPP and the CABP models are conceptually overlapping. Our main hypothesis was that CAPP symptoms would be perceived as indicative of psychopathy in both women and men. Second, we hypothesized that the CAPP symptoms would be perceived as more typical of psychopathy in men in comparison to women. Third, we hypothesized that the results would indicate that the CAPP and the CABP are conceptually overlapping models, but that there are unique symptoms in the CABP model that will not be considered indicative of psychopathy in women and men. Last, we hypothesized that the CABP symptoms would be perceived as more typical of psychopathy in women.
Method
Participants
Correctional officers were recruited from two facilities: a high security prison with male inmates and a medium security prison with female inmates (there are no high security facilities with female inmates in Sweden). Potential respondents were informed about the study and invited to participate by the administrative staff at each unit. They were informed that participation in the study was voluntary, that it would not affect their work and that their responses would be kept confidential. In agreement with prison management, study participation occurred during work hours.
At each facility, 70 correctional officers (i.e., 140 participants in total) were invited to participate in the study. In total, 90 questionnaires were returned, out of which 3 were excluded; 2 were returned blank with the comment of not wanting to participate, and 1 additional questionnaire was excluded for not being completed according to the instructions. The final sample consisted of 87 participants; 25 female officers and 12 male officers (n = 37) from the facility for women who rated female psychopathy, and 25 female officers and 25 male officers (n = 50) from the facility for men who rated male psychopathy. Background demographics about the participants included the following: gender, workplace, occupation, level of education, and years of work experience in the Swedish Prison and Probation Services. The participants were between 22 and 65 years old (M = 40.27, SD = 12.04) and had worked in the Swedish Prison and Probation Services between half a year and 39 years (M = 8.35, SD = 8.19). There were no significant differences between the two participant groups regarding gender, age, educational level or work experience.
Measures and procedure
The study questionnaire was based on an international study protocol used in several previous prototypicality studies of the CAPP (Kreis, 2008). The Swedish translation was used (see the Appendix), which was conducted for clinical use by two of the authors (MP and JL) in collaboration with the developers of the CAPP model. The CAPB symptoms and foils were translated by the same authors, but for this translation, the authors did not have the opportunity to consult the model developers.
Prototypicality ratings of symptoms according to symptom group; CAPP Only, Overlap, CABP Only, and Foils as well as by domain; Attachment, Behavioral, Cognitive, Dominance, Emotional, and Self.
Note. Symptoms rated as significantly different (p value ≤ .05) are shown in boldface.
n varies between 84-87 due to missing cases.
n varies between 47–50 due to missing cases.
Equal variances not assumed.
Participants were asked to complete a questionnaire individually, rating to what degree they considered each symptom to be typical of psychopathy in men or women. Each symptom was rated on a 7-point Likert scale, from 1 (not typical) to 7 (highly typical). The participants were asked to underline symptoms and keywords that they did not understand. One symptom, Unreliable (CAPP Only), was underlined by three participants. Three symptoms were underlined by two participants: Lacks pleasure (CAPP Only) in addition to Strange and Restrained (Foils). No keywords were underlined. Respondents were instructed not to discuss the content of the questionnaire prior to the end of the study.
The study was approved by the Regional Ethical Review Board of Stockholm (#2014/1192-31/1).
Analyses
In line with previous prototypicality studies (Florez et al., 2015; Hoff et al., 2012; Kreis & Cooke, 2011; Kreis et al., 2012; Smith et al., 2014; Sörman et al., 2014; Viljoen et al., 2015), the results regarding the ratings of the CAPP and CABP items are presented using mean values and standard deviations, with the following benchmarks for the degree of prototypicality: over five—highly typical, between four and five—moderately typical, and three or lower—not typical. Differences in mean prototypicality ratings comparing female and male psychopathy as target gender were analyzed with independent samples t tests. The analyses of statistical significance were not corrected for multiple comparisons. Instead, the exact p values are presented to ease comparisons with previous research. Effect sizes were calculated with Cohen's d.
Levels of prototypicality were investigated with a two-way repeated measurement ANOVA. Mauchly's test indicated that the assumption of sphericity was violated, χ2 (5) = 70.12, p ≤ .001, therefore the Greenhouse-Geisser corrected tests are reported (ϵ = .67). Assumptions of normality did not hold for male psychopathy for CAPP Only. We rectified this problem by excluding one outlier from subsequent analyses. Assumptions of equal variance were not met for the variable CABP Only, F(1, 84) = 5.58, p = .021. As the variance was largest in the smaller sample (n = 37, M = 3.40, SD = 0.73, respectively, n = 49, M = 3.54, SD = 0.49), we judged the procedure to hold for further analyses.
All analyses were conducted in SPSS (Version 22).
Results
Prototypicality ratings of the CAPP symptoms
Prototypicality ratings (mean values and standard deviations) of the CAPP symptoms are presented in Table 1, where they are ordered by symptom groups and domains, and in Figure 1, where mean symptom ratings are ranked from highest to lowest. Mean symptom ratings for female (n = 37) and male (n = 50) psychopathy presented in order of mean value for the total sample (n = 87). For each symptom, symptom groups are presented by: P (CAPP Only), O (Overlap), B (CABP Only), and F (Foils) and domains are presented by: A (Attachment), B (Behavior), C (Cognitive), D (Dominance), E (Emotional), and S (Self). Results with p values < .05 are marked with *.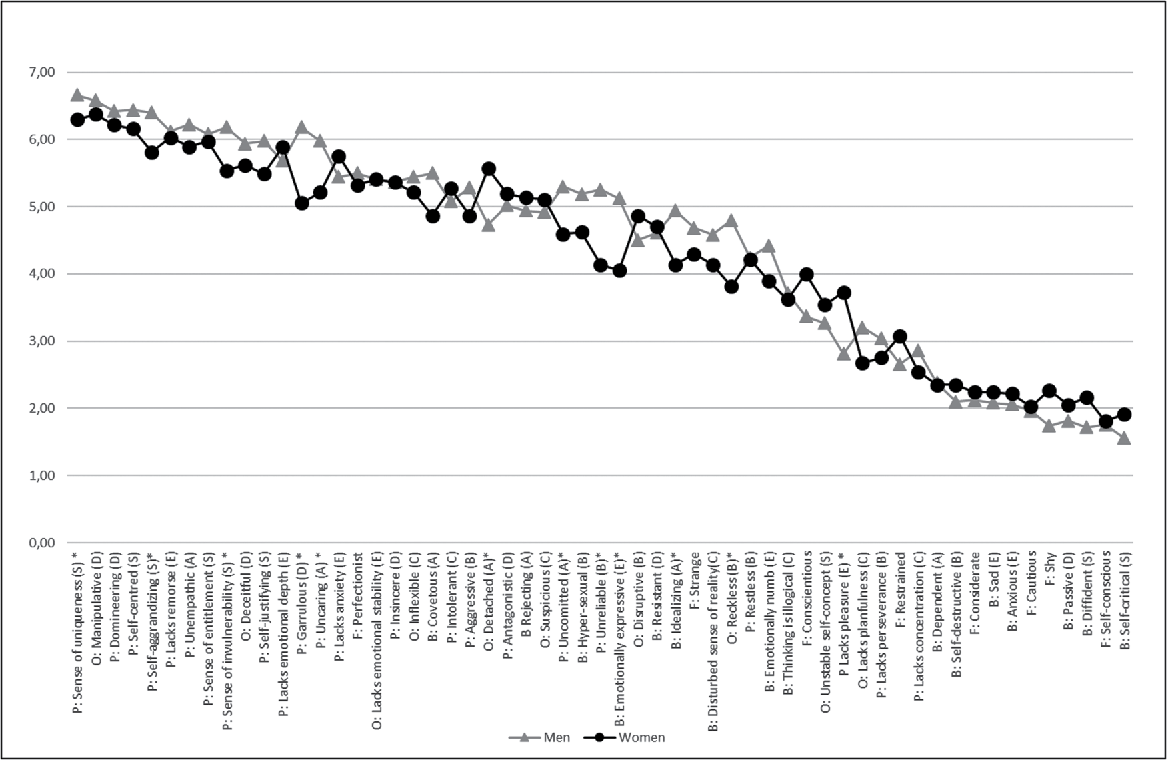
A majority of the CAPP symptoms (28/33) were rated as highly typical (18 CAPP Only symptoms and six Overlap symptoms) or moderately typical of psychopathy (two CAPP Only and two Overlap). Five symptoms were not rated as typical of psychopathy: Lacks Pleasure, Lacks Perseverance, and Lacks Concentration (CAPP Only symptoms) as well as Unstable Self-Concept and Lacks Planfulness (Overlap symptoms).
Out of the eight control symptoms (Foils), Perfectionistic was rated as highly typical and Strange was rated as moderately typical of psychopathy.
Gender differences in prototypicality ratings
When the mean prototypicality ratings were compared according to target gender (female, n = 37, and male, n = 50, psychopathy), the mean values of 12 symptoms differed significantly: Garrulous, Uncaring, Unreliable, Self-Aggrandizing, Sense of Invulnerability, Sense of Uniqueness, Uncommitted, and Lacks Pleasure (CAPP Only symptoms); Reckless and Detached (Overlap symptoms); and Emotionally Expressive and Idealizing (CABP Only symptoms). All of these symptoms, except Lacks Pleasure and Detached, were rated as significantly more typical of male psychopathy. The results are presented in Table 1.
To investigate whether the participant's gender had any impact on their perceptions of psychopathy, the ratings of female and male participants were compared. Female respondents (25 rating female and 25 rating male psychopathy) rated Domineering (CAPP Only symptom) as well as Hyper-Sexual and Emotionally Expressive (CABP Only symptoms) as significantly more typical of psychopathy than did the men. Male respondents (12 rating female and 25 rating male psychopathy) rated Self-Critical (CABP Only) and Self-Conscious (Foils) as significantly more typical of psychopathy than did the women. None of these symptoms corresponded to the symptoms rated significantly different across target gender.
Differences in level of prototypicality in the CAPP and CABP models
To further investigate the validity of the CAPP model, we also evaluated whether symptoms of psychopathy, as defined by the CAPP, were differentiated from symptoms of BPD, as defined by the CABP. Two CABP Only symptoms were rated as highly typical, and six were rated as moderately typical of psychopathy (see Table 1). For each of the four symptom groups, an index variable was constructed that reflected the mean prototypicality value. The mean value was, as expected, highest for CAPP Only and lowest for Foils: CAPP Only, M = 5.29, SD = 0.59; Overlap, M = 4.86, SD = 0.65; CABP Only, M = 3.48, SD = 0.60 and Foils, M = 3.03, SD = 0.8. The mean values of the prototypicality ratings for each symptom group are presented in Figure 2. Mean values of prototypicality ratings for each symptom group for female (n = 37) and male (n = 49) psychopathy.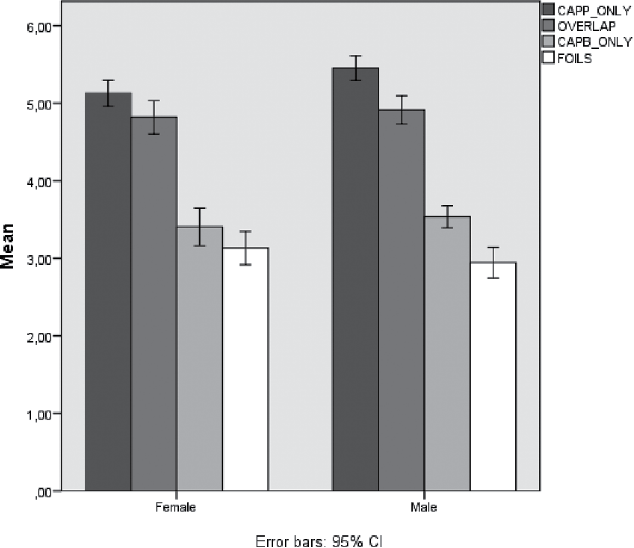
Levels of prototypicality differed significantly by symptom group (F [2.00, 168.27] = 304.55, p ≤ .001). Specifically, the differences between symptom groups were significant at each level: Foils to CABP Only, F [1, 84] = 25.77, p ≤ .001; CABP Only to Overlap, F [1, 84] = 331.20, p ≤ .001; Overlap to CAPP Only, F [1, 84] = 70.37, p ≤ .001. There was no significant effect of target gender on the level of prototypicality (F [2.00, 168.27] = 2.91, p = .057). However, there was a significant effect of target gender when specifically comparing CAPP Only symptoms and Overlap symptoms; that is, CAPP Only symptoms were rated as significantly more typical of male psychopathy (F [1, 84] = 5.16, p = .026). We did not find any significant effect of target gender regarding the other symptom groups. The symptom group confidence intervals of female psychopathy overlapped (CAPP Only CI 4.94–5.26 vs. Overlap CI 4.58–5.01 and CABP Only CI 3.17–3.66 vs. Foils CI 2.93–3.37). This was not the case with male psychopathy (see Figure 2).
Gender differences in prototypicality ratings of unique CABP symptoms
When the prototypicality ratings of male and female psychopathy for unique borderline symptoms (CABP Only) were compared, the mean values of Emotionally Expressive and Idealizing were rated significantly higher for male psychopathy. The results are presented in Table 1.
Discussion
This study aimed to investigate whether correctional staff perceived the symptoms of the CAPP to be indicative of their perceptions of psychopathy, in women and men. Additional aims were to investigate whether there are differences in what is considered typical of women and men who manifest psychopathy and whether the CAPP and the CABP models overlap conceptually. The key findings are that, overall, the CAPP symptoms were perceived to be indicative of psychopathy in both men and women, even though there were some gender differences. There was no overall effect of target gender on how typical the symptom groups were perceived. However, there was an effect of target gender for the unique psychopathy symptoms, indicating that core features of psychopathy are perceived as more indicative of male psychopathy. Furthermore, participants distinguished between symptoms of psychopathy and BPD, but the prototypicality ratings in each symptom group varied, and several borderline symptoms were perceived to be typical of psychopathy. We did not find any support for psychopathic women being regarded as more emotionally unstable compared to men.
Do correctional staff perceive CAPP symptoms to be indicative of psychopathy?
Most of the CAPP symptoms were rated as highly or moderately typical of psychopathy in both women and men. Only two CAPP symptoms (Unreliable and Lacks Pleasure) were marked as not understood by two or three of participants, which indicates that the symptoms and keywords are indeed formulated in common language according to the intention of the developers. In line with previous prototypicality studies, Lacks Pleasure, Lacks Concentration, Unstable Self-Concept, and Lacks Planfulness were not considered typical of psychopathy (Florez et al., 2015; Hoff et al., 2012; Kreis et al., 2012; Sörman et al., 2014). This is not entirely unexpected given that the CAPP model was constructed to be broad and comprehensive (Cooke et al., 2012). In line with previous studies, our results suggest that some CAPP symptoms may be superfluous to the psychopathy construct. From a clinical point of view, it is also notable that Lacks Perseverance, Lacks Concentration and Lacks Planfulness (considered not prototypical), in addition to Restless (which was considered moderately prototypical), are symptoms that can be linked to disturbances in cognitive functioning and hyperactivity, specifically symptoms of Attention Deficit Hyperactivity Disorder (ADHD; APA, 2013). On the one hand, this could indicate an overlap between ADHD and psychopathy in terms of deficient impulse control, but it could also point to a confounding of two constructs.
More intriguing is that two of the control symptoms, Perfectionistic and Strange, were rated as representative of psychopathy – a result that is in line with the findings in one previous prototypicality study (Hoff et al., 2012). Hoff et al. (2012) argued that the relatively high ratings for Perfectionistic might be explained by differing linguistic connotations of the word in Norwegian compared to English, given that none of the control symptoms received high ratings in a prototypicality study conducted with the original English version (Kreis et al., 2012). However, it is not our view that the word “perfectionistic” in Swedish differs in connotation from the corresponding word in English. Furthermore, Florez and colleagues (2015) found that the symptoms Perfectionistic and Strange were rated as prototypical of psychopathy in the community and health professional samples but not in the expert sample. Additionally, in the previous prototypicality study of the CAPP model conducted in Sweden, only one study group (i.e., ward staff working at forensic treatment units) rated Perfectionistic and Strange as moderately typical of psychopathy (Sörman et al., 2014). The divergent results for these control symptoms may therefore reflect differences in study samples. Even though it is of clear interest to investigate the validity of the CAPP model in different samples, to broaden the validity evidence, lay persons are likely to be more susceptible to popular opinions on psychopathy. One explanation for this result could be that compared to clinicians, correctional, and ward staff as well as community members are more affected by media portrayals of psychopathy (e.g., Dexter or Hannibal Lecter), who are portrayed as rigid and perfectionistic. Indeed, a previous prototypicality study that used non-expert respondents showed that movies/TV shows were the most common source of influence on their perceptions of psychopathy (Smith et al., 2014). Nonetheless, despite the potential effects of popular opinion of psychopathy in the current sample, the prototypicality ratings overall were similar to previous studies, which is evidence for the validity of the CAPP model.
How does gender affect perceptions of psychopathy?
We expected to find differences in ratings depending on target gender. The results indicated that few symptoms were perceived differently depending on the target gender. Even though most symptoms were rated as typical of both female and male psychopathy, some divergences occurred: psychopathic men were described as more garrulous, unreliable, reckless, uncaring, self-aggrandizing, and emotionally expressive with a greater sense of invulnerability, while psychopathic women were described as being more detached and lacking pleasure.
Interestingly, previous studies of gender prototypicality of the CAPP model (Kreis & Cooke, 2011; Viljoen et al., 2015) found a majority of the symptoms to be more prototypical of psychopathy in men (25 and 29 symptoms, respectively). In these studies, participants were asked to rate whether they considered each symptom as equally typical for both genders or more typical of either men or women. In contrast, we specifically instructed respondents to rate the symptoms with either a woman or a man with psychopathy in mind. Participants were therefore not asked to compare men and women but rather to describe what they considered to be typical of psychopathy for each gender. This study design might tap more directly into the gender based perception of psychopathy, which could have affected the results. That is, asking participants to actively compare women and men might lead them to emphasize potential differences.
Conceptual overlap of the CAPP and the CABP model
As previously stated, it has been proposed that psychopathy and BPD could be variants of the same underlying spectrum of problematic behavior related to a lack of impulse control and emotional dysregulation. In line with this idea, we expected to find evidence for the conceptual overlap of the CAPP and CABP models but with each condition displaying unique features.
The results supported the models to be differentiated on a symptom group level. Hence, unique CAPP symptoms were perceived to be the most typical of psychopathy, followed by symptoms included in both models. The unique CABP symptoms were perceived as less typical than the overlapping symptoms, followed by the control symptoms, which were rated as the least typical, indicating that the CAPP and CABP models capture distinguishable constructs. Within symptom groups, however, there was a considerable variance in mean values. More specifically, some symptoms that are not included in the CAPP model as representative of psychopathy were rated as such, and vice versa. Most notably, eight of the unique CABP symptoms were rated as highly or moderately typical of psychopathy. These findings lend support to the theory that psychopathy and BPD are overlapping constructs. The CABP Only symptom rated as most typical of psychopathy, Covetous (key words: jealous, possessive, clingy), was not easily translated into Swedish. This could have led to some of the intended meaning of the symptom being lost in the translation process. The second most highly rated symptom, Rejecting (key words disparaging, deprecating, denigrating), could have been interpreted as linked to the antagonistic features of psychopathic personality and possibly to a lesser degree perceived as a typical symptom of BPD. Unfortunately, there are no published studies of general prototypicality ratings of the CABP model, which could have shed some light on this issue. Nonetheless, the results might also be explained by the individual experiences of the respondents. Even though they were not instructed to rate the symptoms with a specific inmate in mind, participants were specifically recruited from correctional facilities because they have experience in working with psychopathic individuals. However, the inmates they come into contact with might display other psychiatric problems in addition to various degrees of psychopathic traits, which could influence the ratings. Furthermore, as mentioned earlier our participants were not clinical experts. This could also affect their perception of the CABP symptoms. For future studies, it would be interesting to investigate the conceptual overlap of the CAPP and the CABP model in a clinical setting in subgroups of psychopathic individuals.
Are CAPP symptoms perceived as more typical of psychopathy in men and CABP symptoms as more typical of psychopathy in women?
The results gave some support for the idea of a man as the prototypical psychopath; symptoms unique to psychopathy were rated as more typical for men. By contrast, the hypothesis that CABP symptoms would be rated as more typical of psychopathy in women was not supported by the results. There were few gender differences, and none of the symptoms were rated as more typical of female psychopathy. Furthermore, two unique CABP symptoms, Idealizing and Emotionally expressive, were rated as more typical of psychopathy in men. Consequently, we did not find any clear support for psychopathy and BPD as differently gendered variants of the same disorder. The results are in contrast to previous research, in which borderline symptoms were found to be perceived as more typical of psychopathy in women (Viljoen et al., 2015). A recent Swedish study among male probationers and parolees, revealed a 19.8% prevalence of BPD (Wetterborg, Långström, Andersson, & Enebrink, 2015). Additionally, the authors found the comorbidity of BPD and ASPD to be 91%. Their findings indicate that psychopathy and BPD are overlapping constructs, but also indicate that BPD in men might be overlooked. The finding that borderline symptoms were not perceived as more typical of psychopathy in women in the current study might indicate that the construct of emotional instability is not adequately captured by the CABP model. However, because we used only psychopathy as a target disorder, the evidence for this conclusion is limited. Another explanation might be that the Swedish gender-egalitarian culture, in which the expression of gender might be less marked in Swedish women and men, and in which it can be seen as politically incorrect to interpret behavior in terms of gender, could lead participants to be less attentive to gender differences in behavior or to soften their opinions.
Limitations
This study has some limitations. The sample was limited to correctional officers, the sample size was relatively small and multiple comparisons were performed. The results, especially regarding the conceptual overlap of psychopathy and BPD, would gain further support if complemented by a sample of forensic mental health experts. Additionally, the prison for women has medium security, while the prison for men has maximum security. As these facilities have different security levels, they probably differ in terms of work culture and attitudes toward inmates, which could affect participants' attitudes toward psychopathy. The type of facility could also affect the makeup of inmates, such that there is a larger proportion of inmates at the high security facility who display pronounced psychopathic personality traits and specific problems of impulse control, emotional instability and disruptive behavior, thus making them difficult to handle at a lower security level. It is plausible that working at a medium security prison would therefore affect one's view of psychopathy, and that this work environment, rather than target gender, explains why symptoms of psychopathy were rated as less typical at the prison for women. Working with female inmates might also entail that participants have less experience with psychopathy due to the lower prevalence of psychopathy in women, possibly leading to the perception that psychopathy is less relevant to women. However, as this is the most secure prison for women in Sweden, we assume that officers working there have extensive experience of psychopathy in women. Further, we had fewer respondents and a larger dropout rate at the facility for women. This could be explained by the small size of this facility, rendering participant recruitment more difficult. We did not have access to any data on individuals who declined to participate. There were, however, no significant differences between participants regarding gender, age, education level or work experience across the two facilities.
Given that we used a slightly different methodology than previous studies (Kreis & Cooke, 2011; Viljoen et al., 2015), comparing the findings across studies is not entirely straightforward. As our main focus was the gender-based perception of psychopathy, we used only psychopathy as target disorder. Borderline symptoms were primarily included as an extra set of “foil” or discriminative items, with the aim of investigating the validity of the CAPP model by examining whether the models could be clearly distinguished from each other, with attention to gender issues. The use of a methodology that would allow for direct comparisons of psychopathy and BPD would facilitate the study of construct overlap and could also provide clearer answers to gender as a key to understanding differences in behavioral expressions of impulsivity and emotional dysregulation in men and women, respectively. As we did not include BPD as a target disorder, the current study provides limited evidence for the validity of the CABP model as such. The less rigorous translation (the lack of contact with the developers) of the unique CABP symptoms further limits the possibility of drawing firm conclusions about the validity of the CABP model.
There are general limitations in the use of prototypicality methodology to investigate the validity of a construct. This methodology does not allow for any control over who the participants had in mind when rating the symptoms. Thus, we do not know how their experiences of specific psychopathic individuals might influence their ratings. To be able to control for other factors that influence the functioning of psychopathic individuals (e.g., psychiatric comorbidity), a crucial next step for future studies is to investigate the CAPP model directly in clinical samples of target individuals. Even so, as clinical studies are resource demanding, there is a clear interest in performing these types of evaluations of construct validity as a first step when developing new conceptual models.
With these limitations in mind, we consider it a methodological strength to allow participants to provide ratings based on one explicit gender, rather than asking them to compare men and women. Moreover, this study was conducted in a correctional context, ensuring that participants had ample experience with psychopathic individuals, but, as the participants were not clinicians, they might therefore not be as heavily influenced by the PCL-R model as experts in the forensic psychiatric field. Last, the use of non-expert samples is an important addition to previous prototypicality studies and contributes further support for the CAPP model.
Conclusions
The current study provides further support for the CAPP model as a promising conceptualization of psychopathy, and it provides support for the validity of the Swedish translation. The results show that few symptoms differed in prototypicality ratings, depending on target gender, indicating that the CAPP symptoms are relatively gender-neutral. The findings lend some support to psychopathy and BPD being overlapping constructs. However, we did not find any support for psychopathic women being perceived as more emotionally unstable than men. The next step in the validation process would be to proceed to a clinical setting, investigating CAPP symptoms in female and male clients and exploring the associations with theoretically relevant criterion variables (e.g., ADHD symptoms, impulsivity, and emotional regulation).
Footnotes
Acknowledgment
Preliminary data were presented at the 11th Nordic symposium on Forensic Psychiatry (August 2015), the annual meeting of the International Association of 815 Forensic Mental Health Services (June 2016), and the 4th. Bergen International Conference on Forensic Psychiatry (October 2016). We thank the Swedish Prison and Probation services for facilitating and supporting the study. We also thank Mette K. F. Kreis for her helpful suggestions for improving the manuscript.
CAPP and CABP models original English version and Swedish translation.
Symptom group/Domain
English
Swedish
CAPP Only
Attachment Domain
Uncommitted
Saknar engagemang i andra
Unempathic
Oempatisk
Uncaring
Bristande omtanke
Behavioral Domain
Lacks perseverance
Saknar uthållighet
Unreliable
Opålitlig
Restless
Rastlös
Aggressive
Aggressiv
Cognitive Domain
Lacks concentration
Okoncentrerad
Intolerant
Intolerant
Dominance Domain
Antagonistic
Fientlig
Domineering
Dominant
Insincere
Förställd
Garrulous
Talför
Emotional Domain
Lacks anxiety
Saknar ångest
Lacks pleasure
Saknar känsla av välbefinnande
Lacks emotional depth
Saknar känslomässigt djup
Lacks remorse
Saknar ånger
Self Domain
Self-centered
Självcentrerad
Self-aggrandizing
Självupphöjande
Sense of uniqueness
Ser på sig själv som unik
Sense of entitlement
Ser på sig själv som särskilt berättigad
Sense of invulnerability
Ser på sig själv som osårbar
Self-justifying
Självrättfärdigande
Overlap
Attachment Domain
Detached
Distanserad
Behavioral Domain
Reckless
Vårdslös
Disruptive
Besvärlig
Cognitive Domain
Suspicious
Misstänksam
Inflexible
Oflexibel
Lacks planfulness
Bristande planeringsförmåga
Dominance Domain
Deceitful
Bedräglig
Manipulative
Manipulativ
Emotional Domain
Lacks emotional stability
Saknar känslomässig stabilitet
Self Domain
Unstable self-concept
Instabil självuppfattning
CAPB Only
Attachment Domain
Rejecting
Avvisande
Dependent
Beroende
Idealizing
Idealiserande
Covetous
Krävande
Behavioral Domain
Self-destructive
Självdestruktiv
Hyper-sexual
Översexualiserad
Cognitive Domain
Disturbed sense of reality
Störd verklighetsuppfattning
Thinking is illogical
Ologiskt tänkande
Emotional Domain
Emotionally numb
Avtrubbad
Anxious
Ångestfylld
Sad
Ledsen
Emotionally expressive
Känslomässigt uttrycksfull
Dominance Domain
Resistant
Omedgörlig
Passive
Passiv
Self Domain
Self-critical
Självkritisk
Diffident
Bristande självförtroende
Foils
Perfectionistic
Perfektionistisk
Conscientious
Plikttrogen
Considerate
Hänsynsfull
Strange
Egendomlig
Restrained
Återhållsam
Shy
Blyg
Self-conscious
Självmedveten
Cautious
Försiktig