
Abstract
Mg-based alloys as revolutionary implantable biomaterials have increasingly attracted considerable attention, owing to their biodegradability in vivo and beneficial effects on biological systems. The degradation process and products of Mg-based alloys have been reported to exhibit significant biological effects on host-tissue responses. However, these effects have not yet been fully understood. This review systemically summarizes and analyses the current understandings and recent research progress in this area. The primary focal points are the biological effects and related mechanisms associated with the degradation behaviour of Mg-based alloys. The biological impacts of the degradation products are elucidated and the arguable or controversial issues are also discussed, providing a pathway toward a greater understanding of the biological implications of Mg-based alloys. Furthermore, based on these biological implications, the restorative potential of Mg-based alloys for applications in tissue repair and regeneration is summarized. Finally, outlooks on biosafety evaluation and design strategies for Mg-based alloy implants are briefly discussed.
Introduction
Biodegradable magnesium (Mg) and Mg-based alloys have been proposed and developed for clinical applications since the late nineteenth century [1]. Owing to limitations such as fast degradation and low mechanical strength, Mg-based medical implants and devices failed to generate satisfactory clinical outcomes for decades and were even considered not appropriate for human applications. Since the late 1990s, advances in fabrication and processing techniques have led to significant improvements in the controls of the biodegradability, biocompatibility, and mechanical properties of Mg, and meanwhile, Mg-based alloys re-emerged as revolutionizing metallic biomaterials [2,3].
In the past two decades, potential applications of Mg-based alloys in various medical fields have been studied, including but not limited to orthopaedic implants, cardiovascular stents, sutures, surgical clips, and staples. Among these, orthopaedic implants and cardiovascular stents received more attention than other applications because Mg-based alloys have appropriate mechanical properties and biodegradability for these applications [4,5]. Recent human orthopaedic and cardiovascular clinical studies have shown the great translational potential of Mg-based alloys, and several commercial products have been produced in these fields. For example, a series of commercial Mg bone screws have been developed or approved for clinical use in China, Germany, and Korea. The clinical use of these bone screws has been extended to hundreds of patients in >50 countries/regions. For cardiovascular application, WE43 (a rare-earth-containing Mg alloy)-based Magmaris® sirolimus-eluting stents produced in Switzerland have reached >2000 clinical implantations in 356 hospitals across 45 countries in Europe, Asia, South America, Africa, and Oceania [6]. Importantly, the clinical needs for orthopaedic and cardiovascular implants are high and increasing rapidly. For example, approximately 2.8 million cases of bone repair are performed annually worldwide [7]. In 2015 coronary artery diseases cause approximately 18 million deaths globally [8]. Thus, the rapidly increasing healthcare demand and market potential have attracted the persistent efforts of materials scientists, biomedical engineers, clinicians, and industry for the development and translation of Mg-based alloys.
Different applications result in varying requirements for material development of Mg-based alloys. For example, relatively high strength is a primary requirement for load-bearing orthopaedic applications, while high ductility and fatigue resistance are more critical for cardiovascular applications in which the implant undergoes significant plastic deformation during implantation, as well as cyclic elastic deformation afterward. Specifically, biodegradable metals for a load-bearing bone implant application are suggested to be comparable to those of pure Ti (ultimate tensile strength: 400∼600 MPa; elongation to failure: 10%∼20% [9]), while biodegradable stent material should have a yield strength >200 MPa, ultimate tensile strength >300 MPa, elongation to failure > 15–18%, and resistance to cyclic fatigue >10–20 million cycles (under physiological-loading conditions) before failure [10].
In addition to mechanical properties, the degradation or corrosion rate of Mg-based alloys is often required to match the level of tissue-healing progress in order to maintain biological and biomechanical stability surrounding the implant. For example, uniform corrosion of Mg-based alloys is usually wanted for predicable degradation rate and mechanical performance, minimizing unexpected implant failure and adverse biological responses due to irregular degradation. This is why the content of impurities in Mg-based alloys (including Cu, Ni, Fe, etc.) should be tightly controlled since they can cause increased and localized corrosion (that corrosion is much faster in some places than in other regions) [11]. Meanwhile, the biological properties associated with the corrosion or biodegradation of an Mg-based alloy is of extremely importance and the biological effects of alloying elements should be carefully examined in alloy design and manufacturing.
To date, Mg-Al based, Mg-rare earth (RE) based, Mg-Zn based, Mg–Ca based, Mg-Sr based, Mg-Li based, Mg-Si based, Mg-Cu based, and Mg-Ag based binary, ternary and quaternary alloys have been proposed for biomedical applications [4,12,13]. Among the alloying elements, Zn, Ca, Sr, Si, and Li within proper concentration ranges are considered non-toxic or possess biological functions that may benefit tissue healing or growth [14–17]. Albeit Cu and Ag are also functional elements (both have antibacterial activity and Cu also has osteogenic/angiogenic capability), their contents in alloys must be strictly controlled to avoid severe toxic effects beyond the concentration threshold. Generally, Al and some RE elements (such as La and Ce [18]) need to be avoided or used with great caution due to their high toxicity.
Current research directions of Mg-based alloys for biomedical applications mainly focus on the exploration of commercially-available Mg-based alloys for clinical uses, development of novel Mg-based alloys or devices, surface modification of Mg-based alloys, and development of evaluation methodologies that meet the regulatory and clinical requirements. Behind these research directions, the understandings of biological implications, and the tissue restorative potential of Mg-based alloys are key foundations and challenges. This is largely because the degradation behaviour and products of Mg-based alloys, in contrast to those of the nondegradable metals, have unique biological effects on the host tissues, and equally important the host tissue responses also significantly affect the degradation behaviour of alloys.
Unfortunately, the biological effects of Mg-based alloy during and after degradation have still yet been thoroughly investigated and understood, especially considering the inconsistent or even contradictory results and notions reported by the existing literature [19–21]. Even for consistently observed biological phenomena associated with Mg-based alloys, few underlying biological mechanisms have been elucidated and widely accepted. For example, although the formation of pores within newly-formed bone has been frequently observed around different Mg-based alloys, the mechanism has not been fully revealed. In fact, this lack of understanding has impeded the rational design and development of Mg-based alloys for wider biomedical applications and has become a major hindrance to the clinical translation and commercialization of Mg-based-alloy medical implants. Even the aforementioned Mg-based alloy products that are ready for market launch demand a better understanding of the biological implications over the products’ lifetime.
This review aims to systemically summarize and analyse the current understandings of the biological effects and implications of Mg-based alloys, attempting to provide a clear and in-depth guide for future studies. In the first part of the review, the degradation behaviour and products of Mg-based alloys in the physiological environment are introduced, and the increasing demand for defining the biocompatibility of biodegradable metals is discussed. Second, the biological implications of Mg-based alloys owing to the dynamic releases of Mg2+ and other degradation products are summarized, focusing on the biological functions and their dose-dependence. Some critical but currently controversial issues (like the origin of pores in new bone) related to the biological effects of Mg-based alloys are also discussed. Third, the tissue restorative potential of Mg-based alloys based on the aforementioned biological implications is described. Finally, an outlook on the translational issues of Mg-based alloys is discussed, including the principal considerations for biocompatibility evaluation and implant design.
Biodegradation of Mg-based alloys
General degradation mechanisms
Mg is electrochemically active with a standard hydrogen potential of −2.7 V (Mg/Mg2+) [22], allowing it to potently react with water in aqueous environments via the following major reactions:


The primary degradation products are Mg2+ ions, OH− ions, and H2 gas. Secondary reactions between the primary degradation products and the biological environment subsequently occur, forming various insoluble deposits such as magnesium hydroxide, magnesium phosphates (Mg2(PO4)(OH)·3H2O) and magnesium carbonates (Mg5(CO3)4(OH)2·5H2O) [23]. The degradation of Mg alloys also releases alloy elements in the form of ions and insoluble deposits. Typically more stable than the α-Mg phase [24], the intermetallic compounds in Mg-based alloys could be released in the form of micro-particles after the degradation of α-Mg matrix. The degradation of Mg-based alloys can also markedly change the peri-implant microenvironment through the consumption of H2O or dissolved oxygen in the host tissue. For example, the degradation of Mg-based alloys can also involve the consumption of dissolved oxygen in the host tissue via an oxygen reduction reaction[25], causing a hypoxic microenvironment that interferes with the cells [26] or affects angiogenesis by upregulating multiple pro-angiogenic pathways [27]. A detailed description of degradation products of Mg-based alloys could be referred to a reference [28].
Electrochemical theory suggests that the degradation rate of Mg-based alloys is determined by both anodic and cathodic reactions. The intrinsic degradation resistance primarily depends on the electrode potential of Mg-based alloy, oxidation layer property, and galvanic-corrosion tendency, which are determined by the physicochemical properties including impurity contents [11] and alloying elements [29–32], microstructure (e.g. grain size and second phase, segregation, and intragranular misorientation) [22,33–39], plastic deformation [40], internal stress [41,42] and so on. Surface treatment or modification, which is common in medical implants [43], can also modulate the degradation rate of the Mg-based alloys by retarding [44] or accelerating [45] degradation reactions.
The in vivo degradation rates of Mg-based alloys, however, depend on both the intrinsic degradation resistance and implantation environment [46]. The effects of the local implantation environment on the degradation rate are so intricate that have not been well understood. This is primarily because in vivo degradation is site-specific and the water content, fluid dynamics, and circulation of body fluids adjacent to the implant site all significantly affect the reaction kinetics of Mg-based alloy during degradation [46–56]. For instance, the degradation rates of a rapidly solidified Mg-Zn-Y-Ce-Zr alloy in adult rabbits were calculated to be 1.65 mm/year in bone, 5.34 mm/year in muscle, and 5.70 mm/year in subcutaneous tissue [48]. The degradation rates of Mg-La-Nd-Zr alloy in rats were 0.28 mm/year for subcutaneous and intramuscular implantation, and 1.12 mm/year for intramedullary implantation [49]. Secondly, the Mg-based alloys prone to degrade faster in acidic environments than alkaline environment owing to the shift of cathodic reaction potential. The microenvironments in vivo have different physiological pH values depending on the anatomical location [57–59] and local host responses, such as an acidic environment induced by severe inflammation or activation of osteoclasts [60,61], or an alkaline environment induced by infection [59,62], indicating that Mg-based alloys can have different degradation rates in vivo. Thirdly, the dynamic change of ionic, molecular, and cellular microenvironments surrounding the Mg-based alloys can foster or destroy the formation of degradation layer and change the kinetics of the degradation reactions [63–69]. Fourthly, mechanical stimulation in load- or shear-bearing tissues (such as blood vessel and fractured bone) also alter the degradation process of Mg-based alloys [70–76]. For example, the degradation rate of pure Mg increased by up to two times under tensile stress [70], and that of AZ31 (Mg-Al-Zn) and AM60B-F (Mg-Al-Mn) alloys increased by one time under fluid shear stress [73,76], compared to the samples without loading.
Degradation products
The direct and primary products from the degradation of Mg-based alloys are Mg2+ ions, OH− ions, and H2 gas (Equation (1)) and they each have different biological effects.
Mg2+ ions: In general, Mg-based alloy degradation creates a Mg2+-enriched microenvironment in peri-implant tissue. It has been reported that excess Mg2+ species diffuse from tissue into blood vessels and are then transported by blood flow, before being excreted into urine via kidney filtration [77]. Mg2+ ions has long been known to regulate many physiological processes such as adenosine triphosphate (ATP) metabolism, muscle contraction and relaxation, neurological functions, and neurotransmitter release, vascular tone, heart rhythm, platelet-activated thrombosis, and bone formation [78]. At the cellular level, a Mg2+-enriched microenvironment has also been reported to affect the functions of stem cells [79], osteoblasts [80–82], osteoclasts [83], endothelial cells [84], and immune cells [85,86]. Mg2+-containing material enhances the binding affinities between the integrin family on the cell surface and their ligand proteins. However, the concentration dependence of this behaviour remains to be determined [87,88].
OH− ions: The release of OH− ions contributes to the formation of an alkaline microenvironment or the increase in the pH value, which affects various cell activities and tissue metabolism processes such as osteoblast and osteoclast activities, tissue oxygenation, vascular smooth-muscle toning, and inflammation response [58,89–94]. OH− ions also contribute to the bacterial inhibitory properties of the Mg-based alloys [95]. Theoretically, the pH value on the surface of pure Mg is >10 in a neutral solution [96], but OH− ions can readily be buffered in a physiological environment. For example, the pH value around pure-Mg screws varies from 7.8 to 8.9 when implanted in rabbit tibia [77].
H2 gas: H2 is a unique degradation product of Mg-based alloys and its biological effect has been increasingly studied in the past few years. H2 is considered nontoxic in breathing gas mixture even at high concentrations of up to 49% vol/vol [97] and its role in cellular function, cell signalling, and the tissue healing process via biochemical and biomechanical (owing to gas accumulation in the tissue) pathways has been gradually uncovered in some recent studies. H2 is a well-known reductive and therapeutic gas [98,99] that can efficiently decrease oxidative stress [100] and inflammation [101]. H2 attenuated lipopolysaccharide (LPS)-induced inflammation by reducing the cytotoxic reactive oxygen species (ROS) that are produced in the inflamed tissues [102]. Notably, it can selectively decrease the number of highly cytotoxic oxidative radicals (such as hydroxyl radical and peroxynitrite) in the diseased cells. Moreover, H2 does not affect the metabolic oxidation–reduction reactions in normal cells or disturbs the physiological ROS that participate in cell signalling [103]. H2 gas (via inhalation with air) can also markedly suppress brain injury by buffering the effects of oxidative stress [103] and H2-rich saline (via intravenous drip infusion) has therapeutic effects on myocardial and renal ischaemia and reperfusion (I/R) injury [101,104,105]. However, solubility of H2 in water is very low, up to only 0.8 mM (1.6 ppm, wt/vol) under atmospheric pressure [97], which means that the therapeutic effects of H2 released from Mg-based alloys on the surrounding tissues and cells remain questionable.
H2 gas accumulation has frequently been found in the tissue surrounding Mg-based implants (e.g. commonly in bone marrow cavity and soft tissues [106,107]). The accumulated H2 trapped in the tissue may induce gas pressure that disturbs tissue regeneration and remodelling processes. For instance, H2 gas cavities in the subcutaneous connective tissue developed a lining structure similar to that of the synovial membrane [108]. Significant gas formation interfering with the cortical bone healing process has also been reported [109]. Gas accumulation in bone marrow cavity may also lead to bone compartment syndrome with bone and marrow ischaemia and necrosis [110]. However, it should be mentioned that the biological effects of cavities in tissue formed H2 accumulation should be size-dependent. Only a gas cavity with a size larger than a critical value might compromise the tissue healing process. Therefore, the diffusion behaviour of H2 and bio-effects of H2 accumulation in different tissues worth further investigation in order to understand the biological implications of the degradation rate of Mg-based alloy.
Other degradation products: In vivo degradation of Mg-based alloys also generates insoluble micro-particles including in situ formed inorganics (such as magnesium phosphate) and intermetallics (which exist in most alloys, such as Mg17Al12 in Mg-Al alloys). These insoluble degradation products have been reported to cause inflammatory responses owing to the reactive oxygen species (ROS) overproduction [111], or interfere with the differentiation process of mesenchymal stem cells (MSCs) and osteo-progenitor cells [112].
Degradation behaviour in specific tissues
Bone
Mg-based alloys exhibit tissue-specific degradation behaviour in vivo. Bone provides a complicated physiological environment where the water content, chemical composition, blood supply, cell type, and mechanical stress vary spatially, leading to an inhomogeneous degradation of the Mg-based alloy implant. These factors are crucial to the degradation behaviours of Mg-based alloys, and thus, should be further understood for the better design of implants. As shown in Figure 1, after a Mg-based alloy screw is transversely implanted in a long bone, the screw contacts with the cortical bone, trabecular bone, bone marrows, and muscle. Substantial variations in water content, vascular anatomy (related to circulation efficiency), cellular components, matrix diffusion coefficient, and mechanical deformation among these anatomical structures creates a highly heterogeneous environment for the screw and its subsequent degradation behaviour. Referring to Equation (1), the water content is a primary determinant of the implant degradation kinetics and varies substantially in the calcified bone (5 wt-%), muscle (76 wt-%), and bone marrows (∼44 wt-%) [113–115]. Moreover, there are several secondary factors affecting Mg-based alloy degradation in the bone. As a rule of thumb, Mg-based alloys tend to degrade faster in the tissue where more blood vessels exist, because the blood flow affects both the water content and transportation rates of the degradation products in the tissue nearby. In addition, existence and density of osteoclasts that create an acidic microenvironment during bone resorption also affect the degradation rates of Mg-based alloys since they degrade at a faster rate in an acidic microenvironment compared to that in a basic environment [61]. For example, Mg-based alloys degraded at comparatively faster rate in the bone marrow and trabecular bone where osteoclasts are abundant, while slower in the cortical bone containing less osteoclasts [116,117]. Furthermore, bone implants of Mg-based alloys often undertake dynamic loads or stresses in vivo, resulting in varied stress distribution depending on the implantation locations. For example, accelerated degradation was typically observed at the site with high mechanical stress like the portion exposed to the bone-fracture gap [72]. Schematic of the degradation environment of a Mg-based alloy screw in bone tissue.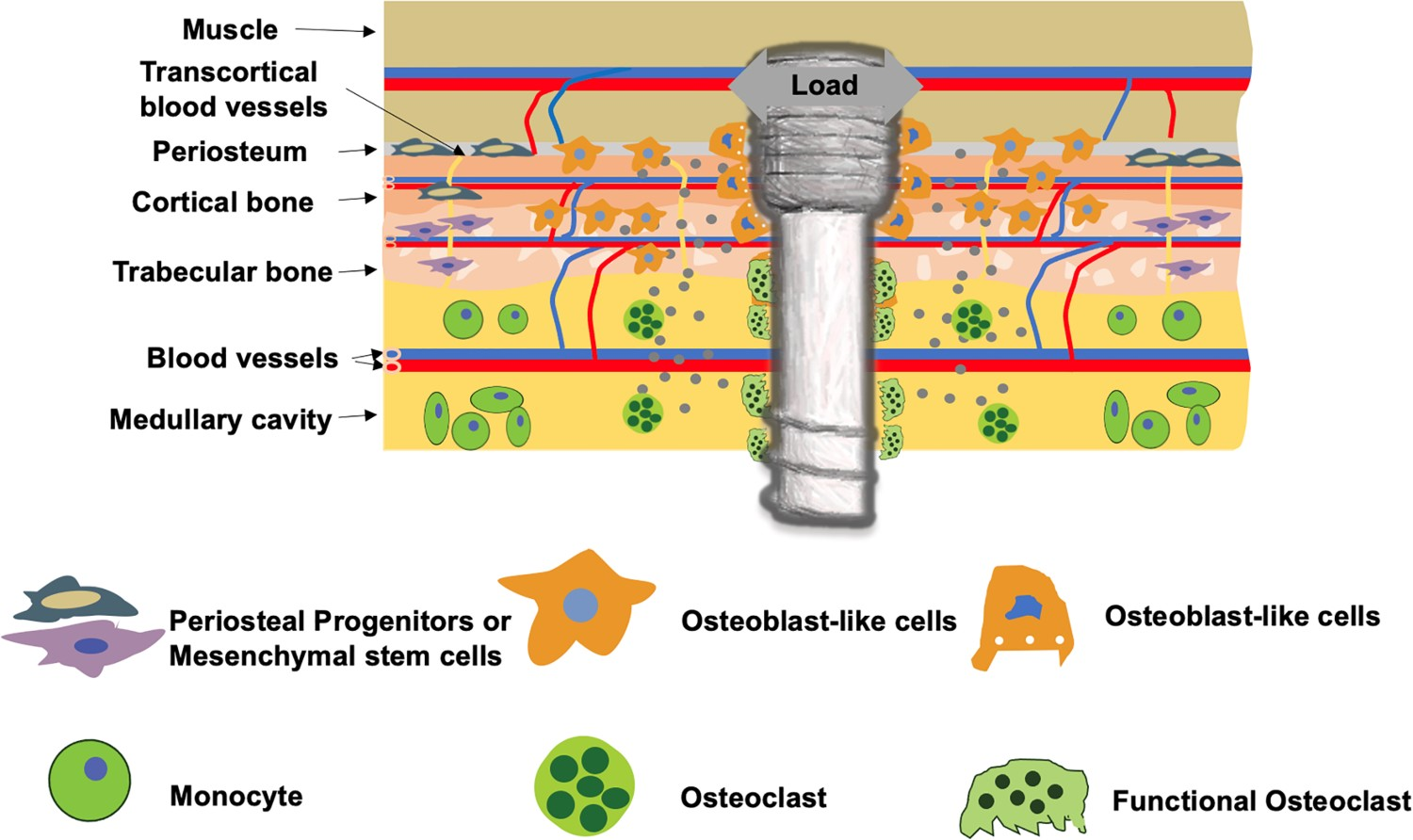
Blood vessel
Mg-based alloys have been studied for cardiovascular stent application. The effects of the biodegradability of Mg-based alloy vascular stent on surrounding tissues include the prevention of chronic inflammatory reactions, progressive neointima development, low risks of thrombosis, and side-branch blockage [118]. The degradation behaviour of Mg-based alloy in blood vessel differs drastically from that in the bone since the stent is immersed in water/blood. As shown in Figure 2, immediately after implantation in the vessels but before endothelialization on the surface, Mg-based alloy stent is directly exposed to blood flow with persistent shear stress and periodic loading of vascular pulsation. Fluid flow significantly affects the degradation mode (including localized, uniform, pitting and erosion modes) and rate of Mg-based stents, as well as the degradation products and local pH changes [73,76]. After endothelialization and the stent is covered by neointima, the degradation of Mg-based alloy stent changes to a vastly different regime where the interaction between the tissue and stent as well as diffusion of water molecules, hydrophilic solutes, and ions through the vascular tissue and arterial wall become dominant factors [119]. Schematic of the biomechanical environment of a stent in a blood vessel.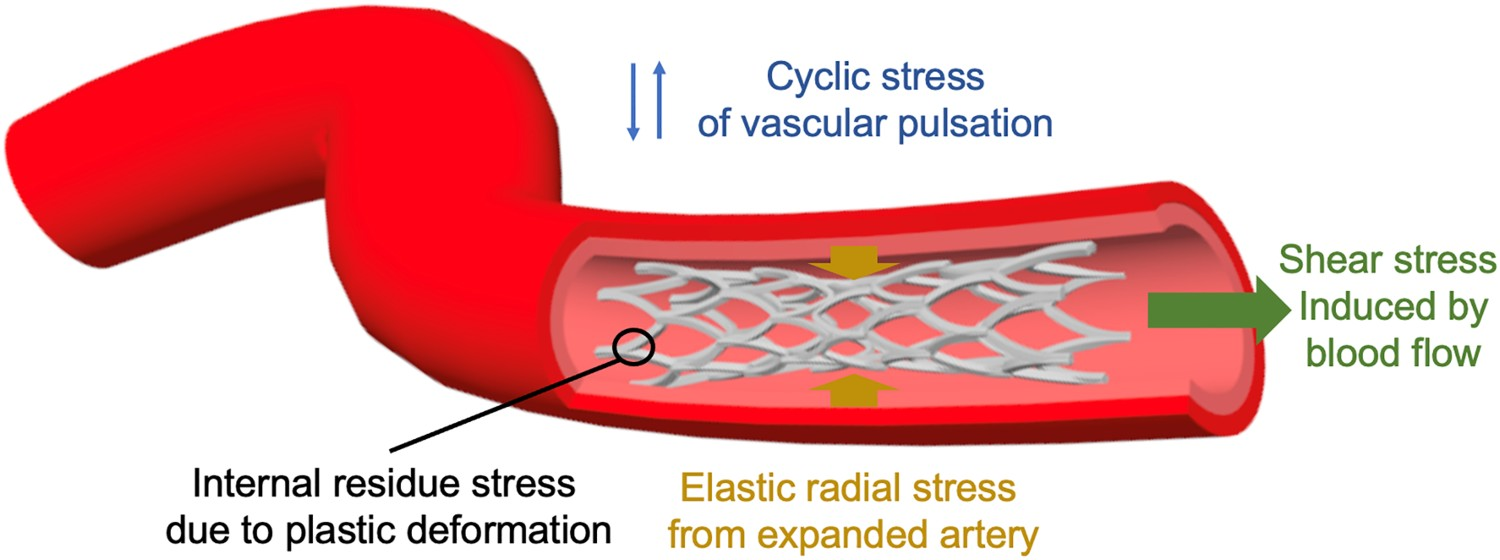
In general, the degradation behaviour of Mg-based alloys in blood vessels is determined by the following mechanisms. First, the biochemical environment of the blood vessel influences the formation of a protective layer on the metal surface. For example, provisional matrix formed by fibrin and activated platelets during the coagulation process, and the adsorption of albumin in the inflammation phase of the healing process of vascular injury may retard the degradation of Mg-based alloys [90]. CO2 in blood vessels (the contents in arterial and venous blood can be up to 4.1% and 5.3%, respectively [120]) can also alter the degradation behaviour of Mg-based alloys by influencing the formation of carbonated film [28]. In addition, acidic or basic environment is important for the formation and destruction of the protective layer on an Mg-based alloy [28]. In vascular systems, blood circulation maintains the microenvironmental pH at an optimal level and this stable condition is unique compared to that in other systems like bone or muscle.
Second, blood flow and vascular pulsation induce a periodic biomechanical environment that can also alter the degradation behaviour of the Mg-based alloy stent. It has been reported that the intensity and direction of fluid shear stress have strong effects on the degradation of Mg-based alloys [73,74,76], primarily by affecting the formation and destruction of the degradation products on the alloy surface. Fluid shear stress at a low level appears to protect the alloy surface from localized corrosion but enhance the rate of uniform corrosion, while high-level shear stress promotes localized corrosion [76]. Also, degradation product detachment and strut fracture occur in the areas facing the flow direction [73]. Specifically in the coronary arteries, the implanted stents can simultaneously experience large variations in the fluid shear stress and tensile stress in multiple directions, so the shear or tensile stress distributions of the stent is not uniform [74]. Meanwhile, the stent is designed to undergo large plastic deformation during implantation and withstand cyclic elastic deformations due to vascular pulsation. Therefore, the ductility and fatigue strength should be considered in stent design. And corrosion fatigue resistance of material is also important to prevent rapid decay of mechanical characteristics. To date, the effects of the biomechanical environment produced by vessel beating, particularly the combined effects of different mechanical conditions, on the degradation of the Mg-based alloy (e.g. WE43 alloy) remains unclear [75].
Third, the specific location where the Mg-based stent is implanted in the blood vessel may also affect the material degradation. The site-dependent degradation of pure-Mg wires (attempt to mimic the stents made of woven wires) has been investigated after implantation in different locations within an artery and results showed increased degradation when the wires were placed in the arterial wall but minimal degradation when they were exposed to blood in the arterial lumen for 3 weeks [121]. Understanding the degradation factors mentioned above can provide the necessary knowledge for expanding the applications of Mg-based implants in cardiovascular field.
Impact of tissue healing progression
Changes in water content, chemical composition, and mechanical conditions of various tissues create varying and complicated microenvironments for the degradation of Mg-based alloy implants. Tissue healing progression also imposes dynamic temporal and spatial variables to the degradation equations, adding more challenges to understand the degradation of Mg-based alloys in vivo.
Generally, bone-fracture healing process includes three stages of inflammation, repair, and remodelling [122]. Each stage involves different cellular responses (e.g. variations in cell type, density, phenotype, activity, and differentiation potential), blood vessel and nerve reconstruction (e.g. changes in type, density, configuration, and functions of vessels or nerves), bone extracellular matrix (ECM) rebuild (e.g. changes in the porosity, composition, molecular/crystal structure and alignment), and stress responses (e.g. the type, magnitude, and direction of stress on the bone implant varies). These complex variations dynamically affect the degradation of Mg-based alloys in different manners. For instance, inflammation may accelerate the degradation due to an acidic environment at this stage [60]. After inflammation, fibrosis tissue formation may kick in and subsequently inhibit the degradation of Mg-based alloys by decreasing blood flow and protecting the corrosion surfaces [70,123]. In the remodelling phase, the activation of osteoclasts may again accelerate the degradation by creating an acidic environment [61].
These understandings, however, are preliminary and based on individual test conditions, so need further investigation. But it is relatively clear that the degradation of Mg-based alloys and tissue host responses affect each other alternately. For example, the generation of degradation products involves chemical reactions on the surface of bone implant, creating a dynamic peri-implant microenvironment with changes in the pH value, Mg2+ ion concentration, and gas cavity in the bone marrow [77]. The subsequent inflammation or an osteolysis response caused by these changes or degradation debris in turn may accelerate the degradation process, as suggested by previous reports [124–126].
The wound-healing process of injured blood vessels is also composed of three overlapping phases of inflammation, granulation, and remodelling [127] which are key to the degradation behaviour of Mg-based alloy stent [128]. For example, in the remodelling phase, the Mg-based alloy stent contacts the vessel ECM, resulting in accelerated degradation [90]. While normal arterial wall ECM is reported to impede the formation of the protective phosphate layer on the alloy surface [121], fibrosis of vascular wall can change the alloy degradation behaviour compared to that in a normal healing process. In addition, the stiffness of vascular wall can be changed by host responses and remodelling process, causing a different mechanical environment for the Mg-based alloy stent. Also, when the degradation progresses, there are changes in the geometry and hemodynamics of the artery, which significantly alter the loading conditions and the stress distribution in the Mg-based alloy stent. All these factors affect further degradation of the stent.
It is worthy to emphasize that the tissue healing effects on the degradation of Mg-based alloy are highly dependent on the alloying elements of the material. First, the alloying element in Mg-based alloys plays a significant role in modulating host tissue responses [17,129–131], which in turn affects the degradation behaviour of the Mg-based alloy as discussed above. For instance, yttrium (∼4 wt-%) and rare earth element (∼3 wt-%) in Mg-based alloy showed strong inhibition of smooth muscle cell (SMC) proliferation but moderate reduction of SMC viability [129]. In contrast, the endothelial cells were viable and showed proliferation in the alloy extracts [129]. Second, the alloying element of Mg-based alloys influences their susceptibility to stress corrosion cracking and resistance to corrosion fatigue [132–134], which largely determines the adaption-ability of implant to biomechanical changes during tissue healing. Third, the alloying elements affect the degradation behaviour of Mg-based alloy, such as the tendency to chemicals-induced local corrosion and the ability to form a protective layer [18,29–32,135,136].
Degradation and biocompatibility of Mg-based alloys
Prior to human applications, medical products require a series of preclinical and clinical evaluations for the assurance of their safety and efficacies. In these evaluations, biocompatibility is one of the core indicators throughout all evaluation processes. Biocompatibility, by one of the accepted definitions, is the ability of a material to serve in a specific biomedical application with an appropriate host response [137]. The concept of biocompatibility is initially formed for non-degradable materials and consists of many convoluted factors that become complicated even confusing in the case of biodegradable materials. The biocompatibility requirements make the materials design of degradable materials different from that of the non-degradable counterparts. For example, some alloying elements allowed to be used in nondegradable metallic biomaterials may not be suitable for the preparation of biodegradable metals, such as Ni, Cr, Mo, and Co, considering their toxic and allergic effects associated with the ion release during material degradation. However, there is a lack of consensus so far on the biocompatibility of Mg-based alloys and its evaluation methods, as the degradation behaviour dynamically alters the host responses to the material, and the conventional criterion and evaluation methodology for the nondegradable materials do not fit to these scenarios.
At the cellular level, the cellular reactions to soluble degradation products (i.e. OH− and Mg2+ ions) are concentration dependent [17,79–82,112,138–141]. Comparative studies directly demonstrate the varied cellular responses (such as the myotube formation of myoblasts, proliferation of fibroblasts, and proliferation and alkaline phosphatase (ALP) activity of osteoblastic cells [35,52,142,143]) to the extracts of Mg-based alloys with different degradation kinetics. At the tissue level, the degradation kinetics and mode of Mg-based alloys have been demonstrated to cause vastly different host tissue responses. For example, it was found in diverse animal bone-defect models that the peri-implant bone response is typically mild with good osseointegration when the Mg-based alloy degrades slowly [53,77,109,144–149]. However, the formation of cavities in bone, which are described as ‘lysis’, ‘shading’, ‘bone resorption’, or ‘bone damage’, frequently occur near the fast-degrading Mg-based alloys, including pure Mg, LAE442 (a Mg-Li��Al-RE alloy), Mg-Gd, Mg-Zn-Ca, and Mg-Zn-Zr alloys [144,145,150–156]. Degradation rate-dependent bone reactions have also been reported in comparative studies [30,109,131,144–146,157–168]. These studies collectively demonstrate that the formation of temporary cavities is a function of corrosion rate, which means that the corrosion rate is too high when cavities can be observed around the implants. A better understanding of the relationship between the host response and degradation behaviours of the Mg-based alloys and a more rational description of the various host responses are the basis for defining the in vivo biocompatibility of the Mg-based alloy. For example, if the aforementioned temporary cavities do not impair the mechanical function of bone, there should be no adverse effects on long-term healing. However, the degradation rate-dependence of tissue responses to Mg-based alloy is hard to elucidate, and also has individual variance. Filling the gap between the in vivo and in vitro degradation behaviours and a better description of the cellular responses to Mg-based alloys (or their degradation products) are important prerequisites to define the biocompatibility of a Mg-based alloy.
Due to the reason mentioned above, there is an urgent need to establish the biocompatibility evaluation methodology for biodegradable materials like Mg-based alloys. Although ISO 10993 sets up a series of methods to evaluate the biocompatibilities of biomaterials that are applicable to the traditional nondegradable metallic biomaterials, some of them are apparently not appropriate for biodegradable metals, as also suggested in previous reports [13,169]. In fact, most of the evaluation methods described in ISO 10993 lack in the consideration of material degradation and the inconsistency in the degradation behaviour between in vitro and in vivo.
Modification of some ISO 10993 articles to evaluate potential health risks of Mg-based alloys have been proposed recently. For example, the modification of the in vitro cytotoxicity testing standard (ISO 10993 part 5) has been recently justified by fully considering the differences in the sensitivities of the cells to Mg2+ ions in vitro and in vivo, and the capability of the in vivo circulation system to dilute the local degradation products [169]. It is recommended a minimum 6 times to a maximum 10 times dilution of the extracts for the in vitro cytotoxicity evaluation of pure Mg as orthopaedic implant based on specifically designed experiments. Several criteria regarding the biocompatibility evaluation of biodegradable metals at the cellular, tissue, and organ levels have also been proposed [13], including IC50 (50% inhibitory concentration) and LD50 (50% lethal dose) data of the metallic ions, inflammatory reactions, and element aggregation in the tissues and organs. Although these modifications are reasonable adjustments to the current biocompatibility evaluation methods, they are still not adequate to complete the jigsaw puzzles of biocompatibility of a specific Mg-based alloy. Therefore, there is still an urgent need to establish the biocompatibility evaluation methods and in vitro/in vivo models specifically for Mg-based alloys based on certain application scenarios (including orthopaedic, cardiovascular, and neural applications).
Recently, biological evaluation of medical devices within a risk management process was suggested in ISO 10993-01-2018, in order to minimize the number and exposure of test animals. Accordingly, in vitro evaluation methods are preferred ‘in situations where these methods yield equally relevant information to that obtained from in vivo models’. Meanwhile, it is suggested that ‘biological testing is usually not necessary, if material characterization (e.g. physical and chemical) demonstrates equivalence to a previously assessed medical device or material with established safety’, and that ‘for device extractables and leachable that have sufficient toxicological data relevant to the expected exposure (quantity, route and frequency), further testing need not be required.’ For Mg-based-alloy-comprising devices, a reliable description or prediction of in vivo degradation behaviour is critical to their biocompatibility evaluation. An effective approach is to develop in vitro degradation experimental models that can resemble application scenarios in vivo and reflect the degradation mechanisms, progression and outcomes. This should provide necessary information for predicting the in vivo degradation behaviour of an Mg-based alloy in comparison to that of a material that has been safely applied in the intended clinical use. This information includes but not limited to degradation rates and modes, release of degradation products and their physicochemical nature (e.g. size distribution and shape of particulate degradation products, etc.). Thus, the establishment of an in vitro evaluation methodological system of degradation behaviour, especially one that closely mimicks the in vivo microenvironment, is of great value [76,170]. In addition to the experimental approaches, bio-physical theories, mathematical models, and mechanical simulation strategies [171–174] of Mg-based alloy degradation are also important supplements to the evaluation methodological system.
Biological implications of Mg-based alloys
Summary of biological processes at cellular and tissue levels that can be mediated by the degradation products of Mg-based alloys.
Implications for bone homeostasis
Modulation of osteoblast and osteoclast activities
Bone continuously undergoes remodelling including reversed activities of bone resorption and bone formation and its homeostasis largely depends on the balance between the activities of the osteoblasts (bone forming cells) and osteoclasts (bone resorbing cells). The bone marrow stromal stem cells (BMSCs) also play an essential role in bone homeostasis since they can potently differentiate into osteoblasts. Mg2+ ions have been found to regulate BMSC functions in a dose-dependent manner. For example, BMSCs cultured in medium with 2.5–10 mM Mg2+ ions showed significantly increased proliferation and enhanced expressions of ALP and integrins α2 and α3 [79]. Cell culture medium containing 10 mM Mg2+ ions also resulted in the up-regulation of collagen type 10A1 and vascular endothelial growth factor (VEGF, critical to vessel formation in bone [236]) expression in the BMSCs and enhanced ECM mineralization [138]. The mRNA expression levels of Collagen I and ALP in the BMSCs cultivated in solutions with 5 and 10 mM Mg2+ ions were significantly higher than those in 0.8 mM solution [139]. Stimulated osteogenic differentiation of the BMSCs has been found to involve magnesium transporter 1 (MagT1)-dependent Mg2+ ion influx [20,183]. However, high Mg2+ ion concentration (5 mM) was also reported to cause disordered differentiation osteoblasts [80]. Besides Mg2+ ions, H2 gas released by Mg degradation was also reported to decrease the ultraviolet radiation-induced BMSC apoptosis by increasing the Bcl-2/Bax ratio, elevating the mitochondrial membrane potential, and blocking cytochrome release [237].
The degradation of a Mg-based alloy generally forms a basic environment surrounding the implantation site. There is evidence suggesting that bone formation can occur in a relatively higher pH environment compared to neutral physiological pH environment (7.35–7.45 for blood and the interstitial fluid) [59,140,218]. ALP activity, collagen gene expression, and collagen synthesis of the BMSCs were significantly increased at pH 7.5 compared to those in the cells cultured at pH 6.6 [219]. The growth and mineralization of human BMSCs at a pH range of 6.3–8.5 were investigated and the optimal activity of BMSCs were found at pH 8.0 [220]. Differentiation of the osteoporotic rat BMSCs was enhanced at pH 7.57∼7.73 compared to that at pH 7.40 [221]. Similarly, collagen synthesis, ALP activity, and thymidine incorporation in human osteoblasts were enhanced when the pH is increased from 7.0 to 7.6 [222]. Moreover, the activity and ALP expression of the osteoblasts improved at pH 8∼8.5 compared to those at pH 7.3 [223,224].
As reported, the Mg2+/OH−-induced activation of the BMSCs and osteoblasts might be via specific signalling pathways, including hypoxia-inducible factor [138], canonical Wnt signalling [238], MAPK/ERK [183], and PI3K/Akt signalling pathways [239], as well as integrin-mediated mechanisms such as modulation of the orientation of adsorbed fibronectin to exhibit enhanced receptor binding affinity and upregulate integrin α5β1 expression of the BMSCs [88].
Osteoclasts are end-differentiated multinucleated cells of monocyte/macrophage lineage and are key players in bone remodelling [240] and periosteal bone formation [241]. Osteoclasts are typically extremely rare cells in the bone with only two to three per cubic micrometer [116]. Osteoclast numbers increase at the sites of active bone turnover such as in the metaphysis of growing bone [116]. When culturing bone marrow cells in a medium containing different concentrations of Mg2+ ions (0.8, 0.4, 0.08, and 0 mM), it was found that osteoclastogenesis increased, while the activity of osteoclasts deceased at low Mg2+ ion concentrations [184]. When less than 25 mM of Mg2+ ions were supplemented in the cell culture medium, low concentrations enhanced while high concentrations inhibited the proliferation and differentiation of the osteoclasts (peaking between 10 and 15 mM) [83]. A recent study showed that high extracellular Mg2+ ion levels (3∼10 mM) promoted vitamin D3-induced osteoclastic differentiation [185]. Insoluble degradation products from Mg-based alloys may also activate osteoclasts [124,125].
The formation of osteoclasts from RAW 264.7 cells (a mouse leukemic monocyte macrophage cell line) was suppressed when the pH was increased from 7.4 to 8.0 [221]. Also, osteoclastic beta-glucuronidase release was suppressed when the osteoclasts were cultured at pH 7.6 compared to those at pH 7.4, which potentially decreased osteoclastic resorption [91]. In addition, H2 gas likely inhibits osteoclast formation as reported by a few studies. For example, 50 vol.% H2 (50 vol. % H2, 20 vol. % O2, 5 vol. % CO2, balance air) decreased proliferation, promoted apoptosis, and inhibited the expression of osteoclast-related proteins of the bone marrow mononuclear cells (BMMCs) in the presence of an osteoclast-inducing medium [235].
Mediation of bone remodelling and quality
At tissue level, bone homeostasis and quality (including porosity and mechanical properties) can be significantly affected by the degradation behaviours of the Mg-based implant. First, a tight control of serum Mg level is beneficial for bone health. Both extremely low or high Mg levels have harmful effects on bone homeostasis [175]. Mg deficiency induces the uncoupling of bone formation and bone resorption, increases osteoclast density at the endosteal bone surface, and decreases the bone mass and osteoblast number [176], trabecular thickness [177], bone mineral content and bone volume (BV) [178], and growth plate width [242]. In contrast, abnormally high serum- and bone-Mg levels also cause mineralization defects and contribute to bone disorders like osteomalacia, renal osteodystrophy and abnormalities [179,180]. Second, Mg-based alloys with proper degradation behaviour can stimulate new bone formation around the implant and the mechanism at cellular level will be discussed later. But numerous studies [21,131,139,157,243–251] have also demonstrated that Mg-based alloys can also simultaneously activate the surrounding osteoclasts, which might lead to bone resorption. Third, Mg-based alloy-induced bone remodelling is also regulated by the immune, vascular, and nervous systems, whose interplays together contribute to bone homeostasis [252–256]. For example, Mg-element-containing biomaterials promoted macrophage polarization to the M2 phase, which supports osteoblast mineralization [86,190,191] and enhances the osteogenic capacity of BMSCs [192]. Mg2+-ion-induced local secretion of neuronal calcitonin gene-related polypeptide-α (CGRP) from the sensory nerve fibres has been shown to improve bone-fracture healing [20]. Meanwhile, degradation products of pure Mg could modulate osteoclastogenesis and platelet-derived growth factor-BB (PDGF-BB) secretion [139,257], which affect bone angiogenesis and H-type vessel formation [254,258,259]. H-type vessels have been recently found to couple with angiogenesis and osteogenesis [260,261]. Angiogenesis is also coupled with the bone modelling and remodelling processes for appropriate bone homeostasis [262]. For example, a Mg5Ca1Zn alloy accelerated bone healing by releasing anabolic metallic ions into the surrounding tissues to promote the angiogenesis-coupled osteogenesis via vascular-mediated pro-osteogenic mechanism [263]. In addition, a Mg-enriched microenvironment (e.g. local Mg2+ ion concentration of 5 mM) has been found to promote neovascularization [84,183].
Dynamic variations in bone remodelling and bone homeostasis unavoidably change the bone quality, which is a generalized description of several concepts such as bone mass, porosity, mineralization content or bone mineral density, and biomechanical properties. However, the effect of Mg-based alloys on the bone quality remains to be determined because of controversial issues regarding the clinical implications of Mg-based alloys. First, although most of the in vivo studies report the increase in overall bone mass around the Mg-based alloys [21,52,148,243,264–267], local osteolysis or bone resorption has also been reported in several Mg-based alloys such as ZEK100, AX30, and MgYREZr alloy [144,150–155,249,268], indicating a possible risk of specific alloys. Balancing bone formation and resorption by the implanted Mg-based alloys is challenging to control the bone mass and quality on demand.
Second, an increase in bone porosity near the bone-implant interface or in the newly-formed bone has been observed in a large number of studies (representative images shown in Figure 3(a,b), but origin of the increased porosity or cavities has not been comprehensively investigated [21,55,72,77,150,155,243,248,249,269–273]. There is a debate regarding the origin of cavities, which have been speculated to be a result from H2 formation [35,72,77,150,155,243,248,272] or increased bone resorption by osteoclasts [21,81,144,150–154,274,275], but neither has been systematically investigated. The emergence of cavities or pores in newly formed bone tissue with sizes greater than a specific value can compromise the mechanical properties of the host bone and therefore should be better understood, particularly for a rational implant design. Our preliminary animal studies showed that a large number of osteoclasts existed at the cavities in bone tissue around Mg implant (Figure 3(c)), indicating that the cavities were more likely induced by the activation of osteoclasts. Representative images showing the formation of porosity in the bone near Mg-based alloy implants. (a) Ex vivo micro-CT 2-D images of bone implant complexes after implantation of LAE442 alloy in NZW rabbit tibia for 12 months [21]. T: tibia; F: fibula; E: endosteal bone formation; C: cavities. (b) Micro-CT images of rat femora implanted with pure Mg or SS rod for 2 weeks [20]. (c) Tartrate-resistant acid phosphatase (TRAP)-stained histological slices of mouse femora cortical bone on the 14th days after implantation with Mg or Ti rods.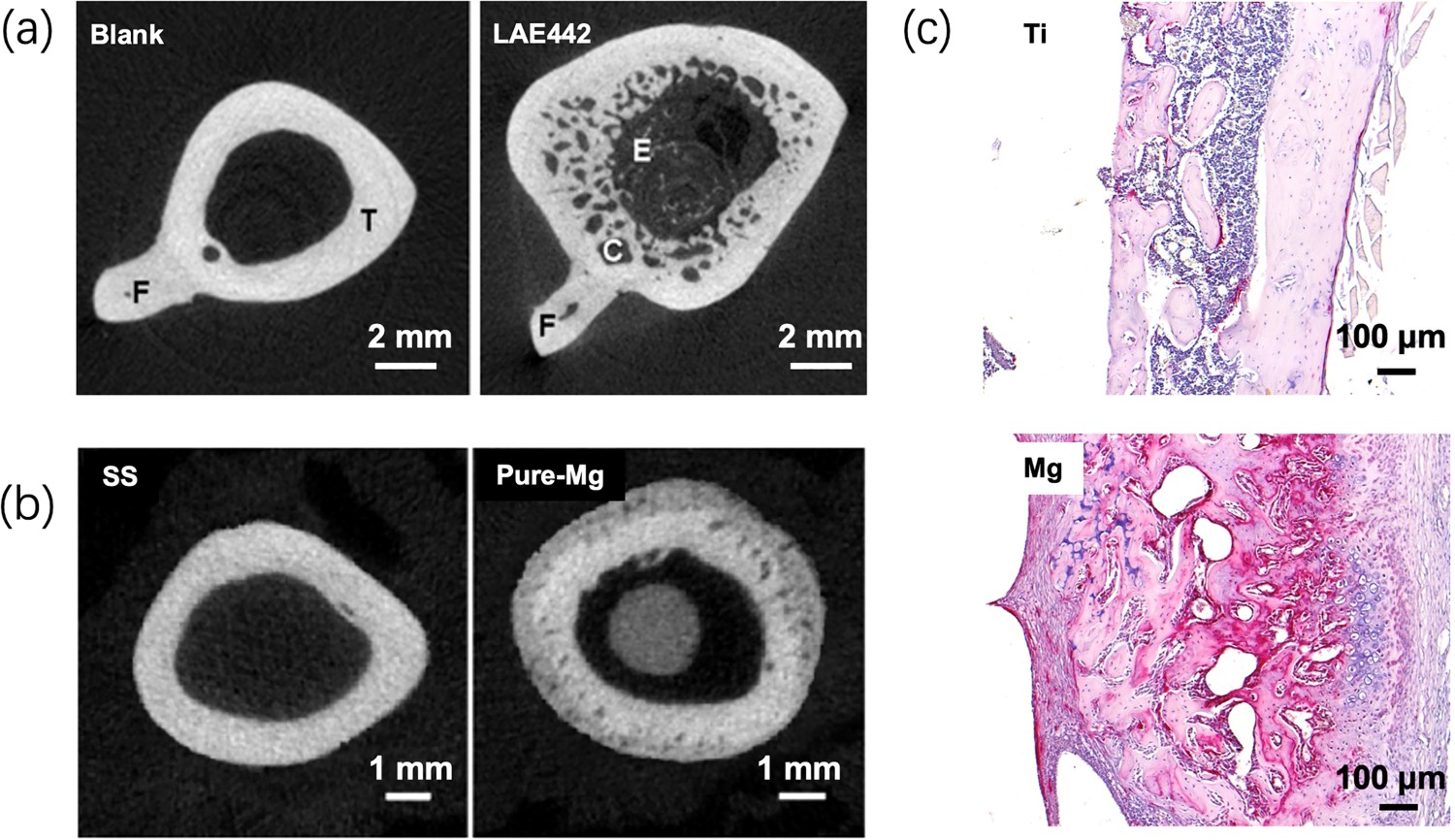
Third, although many studies have demonstrated that bone mineralization surrounding the implants could be enhanced after the implantation of Mg-based alloys [19,51,131,139,157,244–246,249,276–282], decreased mineralization has been reported near pure Mg and MgYREZr alloy [267,271]. The mineral apposition rate varies among different Mg-based alloys and appears to be positively correlated to alloy degradation rate [51,249,276]. The varying mineralization rate can be correlated to Mg2+ ion concentration released into the surrounding tissue, since an appropriate amount of Mg2+ ions can promote bone mineralization [138], while a high concentration of Mg2+ ions may inhibit the mineralization process [80–82,179,180]. Furthermore, degradation of Mg-based alloys can affect the alignment and orientation of the nanosized bone mineral platelets, as well as the crystallite structure, crystal size, lattice spacing, and crystalline order of hydroxyapatite in the bone matrix[159,160,283,284].
It is important to point out that Mg-based alloy-induced changes in the bone biomechanical properties remains unclear. At the microscale level, bone stiffness and hardness can be altered by Mg-based alloys [146,159,160]. However, considering the aforementioned Mg-induced bone porosity, the mechanical properties at the microscale could not reflect the overall bone mechanical properties, which remains to be determined [84]. Importantly, the effect of the porosity or cavities on bone mechanics and its dependence on cavity-size should be investigated through experimental and/or simulation approaches in order to determine the critical cavity size for biomechanical robustness. If the temporary cavities do not hamper the mechanical function of the bone, there may be no adverse effects on long-term healing.
Impact on vascular endothelialization and remodelling
Ideally, vascular regeneration and remodelling mediated by a biodegradable stent like Mg-based or PLGA-based stent should afford a complete re-endothelialization, elimination of permanent irritation to the blood vessel and blood flow, positive vessel remodelling, and restoration of vasomotor function to prevent the development of neointimal hyperplasia and restenosis [285]. The increased Mg2+ ion content, pH value and formation of hydrogen gas resulted from the degradation of the Mg-based stent contribute to the dynamic microenvironment surrounding vascular tissue, which is important for promoting healing response and preventing neointimal hyperplasia and restenosis. At the cellular level, fibroblasts, endothelial cells, and SMCs are involved in vessel endothelialization and vascular remodelling. Poor endothelialization and overproliferation of the fibroblasts and SMCs around the stent should be avoided after stent implantation. After the degradation of stent, the endothelialization by the endothelial cells must take precedence over the fibroblast-involved fibrosis tissue formation.
Extracellular pH and Mg2+ ions can regulate the responses of these cells and subsequent vascular endothelialization and remodelling via several mechanisms. First, both extracellular Mg2+ ions and pH can regulate the fibroblast migration rate by affecting the function of integrin (such as α2β1) and E-cadherin [181,182,225]. For example, cell migration rate and DNA synthesis of fibroblasts decreased almost linearly with an increase in pH values between 7.2 and 8.4 [225]. Second, Mg2+ ions play a significant role in regulating the homeostasis and function of endothelial cells. A low Mg2+ ion concentration (e.g. 0.1–0.5 mM) resulted in the senescent features and dysfunction of the endothelial cells, further causing atherosclerosis, inflammation, arterial stiffening, and thrombosis [186–189,286,287]. It was observed that an extracellular Mg2+ ion concentration of approximately 10 mM promoted endothelial cell proliferation and migration, and further upregulated angiogenesis-related gene expression [17]. An additional study reported that Mg2+ ion concentration of 10 mM stimulated endothelial cell proliferation and enhanced the mitogenic response to angiogenic factors and nitric oxide synthesis compared to that of 1 mM [288]. A Mg2+ ion concentration of 1 mM also promoted the spreading of endothelial cells on multiple ECM substrata compared to that of Mg-free medium [289]. Mg2+ ions induced both the chemokinetic and chemotactic migration of endothelial cells peaking at 0.1 and 10 mM [289], respectively, while the viability and proliferation of human-coronary-artery endothelial cells increased at MgCl2 concentrations from 1.6 mM to 25 mM [198]. Mg also plays a key role in preventing calcification in vascular SMCs [199,290–294]. Extracellular alkalization from pH 7.4 to pH 7.8–8.0 induced a rapid and large vasoconstriction of the SMCs [215]. The intracellular pH and nitric oxide concentration of the endothelial cells and vascular SMCs increased at an extracellular pH of 8.5 [216]. The intracellular pH regulates the intracellular Ca of the vascular SMCs and vascular smooth muscle tone [217]. Third, SMC proliferation was found to be restrained by relatively high concentrations of Mg2+ ions [141,198,200]. A possible explanation is that endothelial cells have a higher tolerance to metallic ions compared to that of the SMCs. For example, SMCs were studied to reveal an upper tolerance limit of approximately 20 mM Mg2+ ions, which was significantly lower than that of the endothelial cells (approximately 40 mM) [17,141,295]. Also, the degradation of Mg-based alloys can cause a shift of the contractile vascular SMCs to an inflammatory phenotype. Vascular SMCs became more proliferative and migratory but undergo apoptosis when exposed to the degradation products of pure Mg, while the AZ31 extracts caused less division and more apoptosis of the vascular SMCs, thus decelerating cell movement and growth [201].
Effect on inflammation
Mg2+ ions have also exhibited anti-inflammatory effect [189,193,194,210,296]. Mg2+ ions (including solution extracts of Mg-based alloys [297]) have been reported to decrease pro-inflammatory markers (CCR7, CD86, CD11c, and iNOS) and pro-inflammatory cytokines (TNF-α, IL-6 and IL-1β), and increase anti-inflammatory molecules (CD163 and CD206) of macrophages under non-stimulated or LPS-stimulated conditions [190,195–197,298,299], indicating that Mg2+ ions could switch the macrophage phenotype from M1 to M2. Besides the Mg2+-enriched ionic environment, Mg-based alloys could modulate inflammation reaction by regulating the physiological pH environment, since many cytokines and proteases that are associated with extracellular alkalosis are involved in the activation of inflammatory cells[92,93]. For example, the inflammation-related p38-MAPK signalling pathway was activated at pH 8.5∼9.5 [94]. Furthermore, H2, being a unique degradation product of Mg-based alloys, is considered a therapeutic medical gas with anti-inflammatory effect [102,232,300] and its effectiveness against several inflammatory disorders has been demonstrated in animal models [232–234].
The modulatory effects of Mg-based alloys on tissue inflammation response are important for tissue lesion repair and regeneration [85,301]. For instance, degradation products of pure Mg showed beneficial effects on promoting MSC proliferation and osteogenic differentiation at appropriate concentrations (e.g., Mg2+ ion concentration of approximately 5 mM) [302]. Mg-2Ag and Mg-10Gd extracts (5 mM Mg2+ ions), pure-Mg scaffold, and Mg-doped titanium showed alteration of macrophage polarization to the M2 phase, which supports osteoblast mineralization [86,190,191]. Additionally, Mg2+ doped in calcium phosphate cement affected the crosstalk between immune cells and osteogenesis-related cells that facilitates bone healing [192]. Most recently, the central role of immunomodulation in Mg2+-induced bone regeneration was revealed [303]. During the early inflammation phase, Mg2+ ions lead to the formation of a pro-osteogenic immune microenvironment. In the later remodelling phase, however, the continued exposure of Mg2+ ions not only causes the overactivation of NF-κB signalling in macrophages and increased number of osteoclastic-like cells but also decelerates bone maturation through the suppression of hydroxyapatite precipitation [303]. Besides bone repair, the immunomodulation effect is essential for successful healing of muscle [304–306]. In the past few years, several strategies have been proposed to modulate the inflammatory response to enhance skeletal muscle repair [307,308], particularly through promoting a M2-balanced response [309]. Therefore, the potential of Mg-based alloys in muscle repair is worth being investigated. Most recently, Mg-based alloys were proposed for skeletal muscle repair in a Chinese patent (application number: CN202110860093.5) based on the observed healing effect of Mg2+ ions on skeletal muscle loss.
Microbial inhibitory effect
The microbial inhibitory effect of Mg-based alloys has been revealed recently [310], which is probably related to the release of OH− and Mg2+ ions that have anti-bacterial effects. A microenvironment with a pH > 9.0 inhibited the growth of most bacteria [226] because abundant OH− species continuously react with H+ from the bacterial ECM and decrease the ATP level of the bacteria [227]. Consumption of H+ around the biomaterial surface can effectively restrain or even kill bacteria [311]. Although Mg2+ ions are well-tolerated by bacteria [95], the synergetic effects of alkalinity and Mg2+ ions contribute to a better bacterial killing capability compared to that with only alkalinity [312]. Recently, hydrogen gas has also shown efficacy in antibacterial and antibiofilm applications [231], and a mechanistic study has revealed that the diffusion of active hydrogen into bacteria upregulated bacterial metabolism genes, which encode a high expression of oxidative metabolic enzymes to generate substantial ROS and cause severe DNA damage. Moreover, Mg(OH)2 and MgO nanoparticles, which are the products of Mg-based alloy degradation, have been reported to exhibit antibacterial activities against Escherichia coli, Staphylococcus epidermidis, Pseudomonas aeruginosa, and Streptococcus mutans [313–316]. Mechanistically, nano-MgO exhibits antimicrobial activity through acid–base reaction between the MgO surface and bacterial wall [313,315], while nano-Mg(OH)2 destroys the integrity of the cell walls after adsorption on bacteria [314].
Pure Mg showed antibacterial effects against Escherichia coli, Pseudomonas aeruginosa, and Streptococcus aureus, with efficacies similar to those of fluoroquinolone antibiotics [317]. The therapeutic effect of pure Mg on osteomyelitis caused by Streptococcus aureus was also been described [318]. Similarly, pure Mg was reported to have the capability to prevent methicillin-resistant Streptococcus aureus (MRSA)-associated osteomyelitis [281]. Furthermore, Mg-based alloys containing well-known antibacterial elements (such as Ag, Cu, and Zn) exhibited better antibacterial activities compared to those of pure Mg [319–322]. For example, a Mg-Nd-Zn-Zr alloy (JDBM) deceased a higher number of bacteria in the MC, prevented abscess-lesions, and supported new bone formation compared to the results with pure Mg in the Streptococcus aureus-induced rat femoral osteomyelitis model [323]. A Mg-Cu alloy intramedullary nail (IMN) repaired bone defect caused by infection in a MRSA-induced rabbit osteomyelitis model [324].
Despite encouraging results, inconsistencies in the antibacterial efficacies of Mg-based alloys have been reported between the in vitro and in vivo studies. For example, an AZ91 alloy exhibited no antimicrobial properties in vivo but showed clear effects in vitro [325]. Similar findings have been reported for pure Mg [95,326]. The inconsistencies may be due to the variations in animal experimental protocols, uneven dispersion of bacteria in the surrounding tissue and so on. Meanwhile, the possible lower degradation rate of the Mg-based alloy in vivo compared to that in the in vitro antibacterial test, and buffering capacity of the living tissue can decrease Mg2+ ion concentration and pH environment near the implant, compromising the antibacterial efficacy. Therefore, filling the gap between the in vivo and in vitro antibacterial properties of Mg-based alloys is important for the development and application of anti-infectiousMg-based alloys. Another challenge in this direction is to develop Mg-based alloys simultaneously with antibacterial and pro-regenerative capabilities. Improved materials research, mechanistic understanding of tissue cell and bacterial functions, and effective evaluation methods are basis to resolve the two challenges of Mg-based alloys for simultaneously promoting tissue repair and inhibiting infection.
Impact on nerve regeneration
Mg supplements have been widely used to treat the nervous system injuries. Successful repair of the nervous system requires either the replacement of neurons that have been damaged by injury or the promotion of axon growth to the original targets. Prior studies, including those by our research groups, have shown that Mg-based alloys show good biocompatibility with the dorsal root ganglion sensory neurons (Mg-10Li and ZN20 alloys) [327] and Schwann cells (Mg70Zn26Ca4 metallic glass) [328]. Recently, it has been reported that the addition of Mg2+ ions in the cultures of neonatal murine neural progenitor cells (NPCs) resulted in increased cell survival [202]. Additionally, the increase in Mg2+ ions by adding magnesium sulfate or magnesium chloride to the culture medium also significantly promoted the differentiation of NPCs into postmitotic neurons and suppression of glial cell differentiation [203].
Mg-based alloy wires/filaments coupled with polymeric conduits have been demonstrated to promote the repair of peripheral nervous system injuries in vivo [329–331]. For example, pure-Mg filament that was placed inside the poly (caprolactone) conduits was used to repair the segmental sciatic nerve defects [329]. Numerous regenerating axons were observed after the complete degradation of pure Mg with only a mild inflammation response in the surrounding tissues. Functionally, in comparison to the control, better recovery of the gastrocnemius muscle was observed in the Mg-treated group. Another study also demonstrated that the pure-Mg filaments placed inside hollow nerve conduits supported long distance axonal regeneration [330].
Rats treated with magnesium L-threonate (MgT) revealed the enhancement of synaptic plasticity and memory by increasing the Mg2+ ion level in rat brains [204]. The application of MgT also reduced Aβ-plaque and prevented synapse loss and memory decline in Alzheimer's disease model mice through elevating brain magnesium [205]. In summary, the biological functions of Mg2+ ions in the nervous system have demonstrated the therapeutic potential of Mg-based alloys for the treatment of nervous system diseases [332,333].
Prevention of cartilage degeneration
Degradation products of Mg-based alloys exhibited clear beneficial effects on cartilage regeneration and protection of cartilage from degeneration [193]. High concentrations of Mg2+ ions (10∼20 mM) supported chondrocyte proliferation (peaking at 10 mM), redifferentiation, and glycosaminoglycan (GAG) production (peaking at 20 mM) [206]. An in vivo study also confirmed that an intra-articular injection of magnesium chloride (20 nM in 20 μl saline) protected knee cartilage by inhibiting autophagy formation [334]. Mg2+ ions promoted chondrogenesis of human synovial MSCs (5 mM) in vitro, ex vivo (human osteochondral defects filled with synovial MSCs in 8 ml PBS with 10 mM Mg2+ ions) and in vivo (rabbit knee osteochondral defects filled with synovial MSC suspension in 30 ml of PBS with 5 mM Mg2+ ions) synthesis of cartilage matrix by the possible mechanism of enhanced adherence of synovial MSCs through integrins [335]. Importantly, Mg microspheres with fine-tuned degradation rate (Mg2+ ion of solution extracts reached 10 mM at day 3) showed the potential to facilitate the formation of layered structures of articular cartilage [207].
H2 and Mg2+ ions also exhibit anti-inflammatory and anti-oxidative effects that can potentially mitigate tissue inflammation and prevent cartilage destruction [193,232,234]. Mg2+ ions (2.2 mM) enhanced the chondrogenic differentiation of mesenchymal stem cells by inhibiting activated macrophage-induced inflammation [197]. In addition to the aforementioned anti-inflammatory effects, Mg2+ ions can inhibit Ca2+-stimulated mitochondrial ROS generation and permeability transition (nonspecific inner mitochondrial membrane permeabilization) [210]. H2 can also efficiently reduce oxidative stress [100] and restore cell death and transcriptional alterations induced by the selective removal of ONOO- derived from NO• in chondrocytes [234]. Notably, Mg-based alloys may potentially prevent osteoarthritis (OA) by mitigating tissue inflammation. For example, poly(lactic-co-glycolic acid) microparticles containing pure-Mg powder, which were intra-muscularly injected to the OA knee as an in situ depot for continuously evolving H2 gas, could effectively mitigate tissue inflammation and prevent cartilage from destruction, thereby arresting the progression of OA [336].
Furthermore, the antagonism effect of Mg2+ ions and pH on Ca2+ ions involves many physiological processes including blood coagulation [337], inflammation response [338–341], collagen accumulation [342], muscle contraction [343], probably through competing for the same binding sites on protein molecules [211,344] or regulating the intracellular Ca2+ concentration and binding to the internal anionic sites [345,346]. Recent studies suggest that the pathological calcification of articular cartilage plays a critical role in OA pathology as a disease initiator of OA progression [347,348]. Therefore, it is highly possible that high extracellular Mg2+ ion concentration and high pH resulted from Mg-based alloy degradation are expected to have an antagonistic effect against Ca2+, which may be beneficial in treating OA induced by the pathological calcification of articular cartilage. Specifically, an imbalance in Ca homeostasis is the underlying cause of calcification in OA, and calcium phosphate crystal deposition is a hallmark of OA, and directly contributes to joint degeneration [349]. The inhibition of pathological crystallite deposition within the joint tissues therefore represents a potential therapeutic target in the management of OA. Mineralization in the matrix vesicles and mitochondria of chondrocytes stems from single mitochondrial granules generated by the combination of Ca and phosphorus in the mitochondria [350]. Mg2+ ion as an antagonist of Ca2+ ion can inhibit spontaneous ATP release as well as the frequency and amplitude of Ca oscillations, to ultimately inhibit mineralization [212]. Meanwhile, the cytosolic Mg2+ ions may attenuate mitochondrial Ca2+ ion uptake [351], which can also possibly prevent pathological crystallite deposition.
Antagonizing effect against calcium-induced cell death
Ca2+ ions are a powerful ‘death trigger’ to cells that cellular Ca2+ overload, or perturbation of intracellular Ca2+ compartmentalization, can cause cytotoxicity and trigger either apoptotic or necrotic cell death [352]. In contrast, Mg is anti-apoptotic in mitochondrial permeability transition and antagonizes Ca-overload-triggered apoptosis [210,211,213]. For instance, Mg2+ ions can inhibit Ca2+-stimulated mitochondrial ROS generation and permeability transition [210]. This potential antagonizing effect against Ca-induced cell death is of considerable values for tissue repair.
For instance, a traumatic injury to skeletal muscle leads to the rupture of sarcolemma, which results in Ca influx, thereby triggering the activation of Ca-dependent proteases and initiation of myofiber necrosis [353,354]. Owing to the antagonizing effect against Ca, a high Mg2+ ion concentration and high pH of the microenvironment surrounding the degraded Mg-based alloy are expected to alleviate Ca-induced myofiber necrosis. This is supported by a recent finding that Mg depletion caused structural damage to the muscle cells due to disrupted Ca homeostasis and oxidative stress [214]. In turn, free-radical-induced membrane damage that results in Ca overload may be the origin of skeletal muscle lesions that occur when Mg is deficient [355]. A recent Chinese patent (application number: CN202110860093.5) proposed to use Mg2+ ions for the treatment of Ca-induced skeletal muscle necrosis.
Similarly for cartilage, the overstimulation of N-methyl-d-aspartate (NMDA) receptors results in a high Ca2+ influx leading to Ca overload, which is an important cause of mitochondrial ROS generation, decrease in ATP, and shortage of cellular energy [356,357]. Ca2+ overload also causes cytomembrane injury by hydrolyzing phospholipids and subsequent cell death. The inhibition of NMDA receptor by Mg2+ ions sequentially decreased the Ca2+ influx, leading to the prevention of chondrocyte damage in OA [208,209].
Anti-tumour activity
Mg2+ ion is a beneficial supplement for the prevention and treatment of osteosarcoma [358], and an increase in the local pH value has been found to damage cytoskeletal F-actin of the bone cancer cells [359,360]. Recently, the tumour inhibitory effect of H2 has been revealed [228,229,361], which could be correlated to the effect of hydrogen on intratumoural ROS levels owing to its anti-oxidation property[362,363]. For instance, H2 scavenged free radicals in bone cancer cells with an efficacy proportional to the rate of H2 release [230].
Recent studies have confirmed the antitumour effects of Mg-based alloys on cancer cells, demonstrating their potential use in clinical oncology as biodegradable implants with antitumour activities [230,364–367]. In a mice transplantable tumour model [364], surface-treated pure Mg inhibited tumour growth, and the anti-tumour property was associated with the H2 release rate. Pure-Mg wires significantly inhibited the growth of SKOV3 cells (human ovarian cancer cell line) in an ovarian tumour model created by the subcutaneous injection of SKOV3 cells in nude mice, indicating their potential for the treatment of ovarian tumours [366]. In vitro tests of this study showed that the inhibitory effect could be due to the degradation products such as Mg2+ ions and H2, which induced SKOV3 cell apoptosis. In another study, pure Mg and Mg–1Ag–1Y alloy both exhibited inhibitory effects against local tumour growth and pulmonary metastasis in nude mice (BALB/c), probably due to the changes in the extracellular acidosis microenvironment, increase in Mg concentration, suppression of C-X-C chemokine receptor type 4 (CXCR4) levels, and increase in prostacyclin (PGI2) synthesis [368]. A WE43 alloy (Mg-3.56%Y-2.20%Nd-0.47%Zr, composition provided in weight percent) also showed inhibitory activity against tumour cells, indicating that the WE43 alloy could be a promising candidate with local antitumour activity for application in orthopaedic implants in clinical oncology [365]. Several studies have revealed that the alloy composition, surface treatment, and degradation rate of Mg-based alloys can affect their antitumour activities [230,368–372], but the efficacy and mechanism of antitumour activity and their correlation to these material properties remain unclear.
Restorative opportunities and applications of Mg-based alloys
Orthopaedic implants and fixation devices
Mg-based alloys have an elastic modulus (∼45 GPa) that more comparable to that of bone tissues than do nondegradable bio-metals, and simultaneously have a relatively high ultimate tensile strength (100∼400 MPa [13]), which enables their applications in biodegradable orthopaedic implants [154,373,374]. Recent studies have reported that Mg-based alloys can accelerate bone-fracture healing [19,72,239,277,375–379]. For example, pure-Mg plates and screws induced peri-implant bone formation with mature osteocytes and active osteoid at the ulna fracture gap (Figure 4(a)) [375,376]. Pure-Mg screws increased bone growth and bone mineral density at the femoral intracondylar fracture gap compared to those observed with the poly L-lactic acid (PLLA) control (Figure 4(b)) [72,277]. WE43 plate and screw systems also promoted fracture healing in a porcine craniomaxillofacial osteotomy fixation model [377]. A SrHPO4-coated Mg-Nd-Zn-Zr alloy IMN induced substantial bone formation in the femoral fracture sites (Figure 4(c)) [239]. Mg-Nd-Zn-Zr IMN solely enhanced osteoporotic fracture (OPF) repair by promoting callus formation in comparison to that of stainless steel (SS) IMN [251]. A Mg2Ag IMN augmented callus formation with accelerated mineralization at the beginning of femur fracture healing and enhanced cartilage turnover at the end of the remodelling phase [19]. Examples of Mg-alloy-based bone-fixation implants. (a) Mg plate and screws for fractured ulna fixation. μCT and toluidine-blue staining of cortical bone after 8 and 16 weeks [376]. (b) Pure-Mg and PLLA screws for femoral intracondylar fracture fixation. μCT scanning of rabbit femur with screws after 4 weeks (red arrows: fracture gap) [277]; (c) SrHPO4-coated JDBM (a Mg–Nd–Zn–Zr alloy) IMNs. Undecalcified sections with Von Gieson staining and μCT 3D reconstruction of rat femurs with IMNs after 8 weeks (red boxes: fracture gap region) [239]; (d) Pure-Mg screw for goat femoral neck fracture fixation, and preoperative and 48-week postoperative μCT 3D reconstruction [380]; (e) Ti/Mg hybrid plate screw system for the fractured tibia fixation (red or blue arrows: Mg screw with PLA coating) [278]; (f) SS/Mg hybrid IMN made by inserting a Mg rod into a hollow stainless steel needle with drilled holes [20].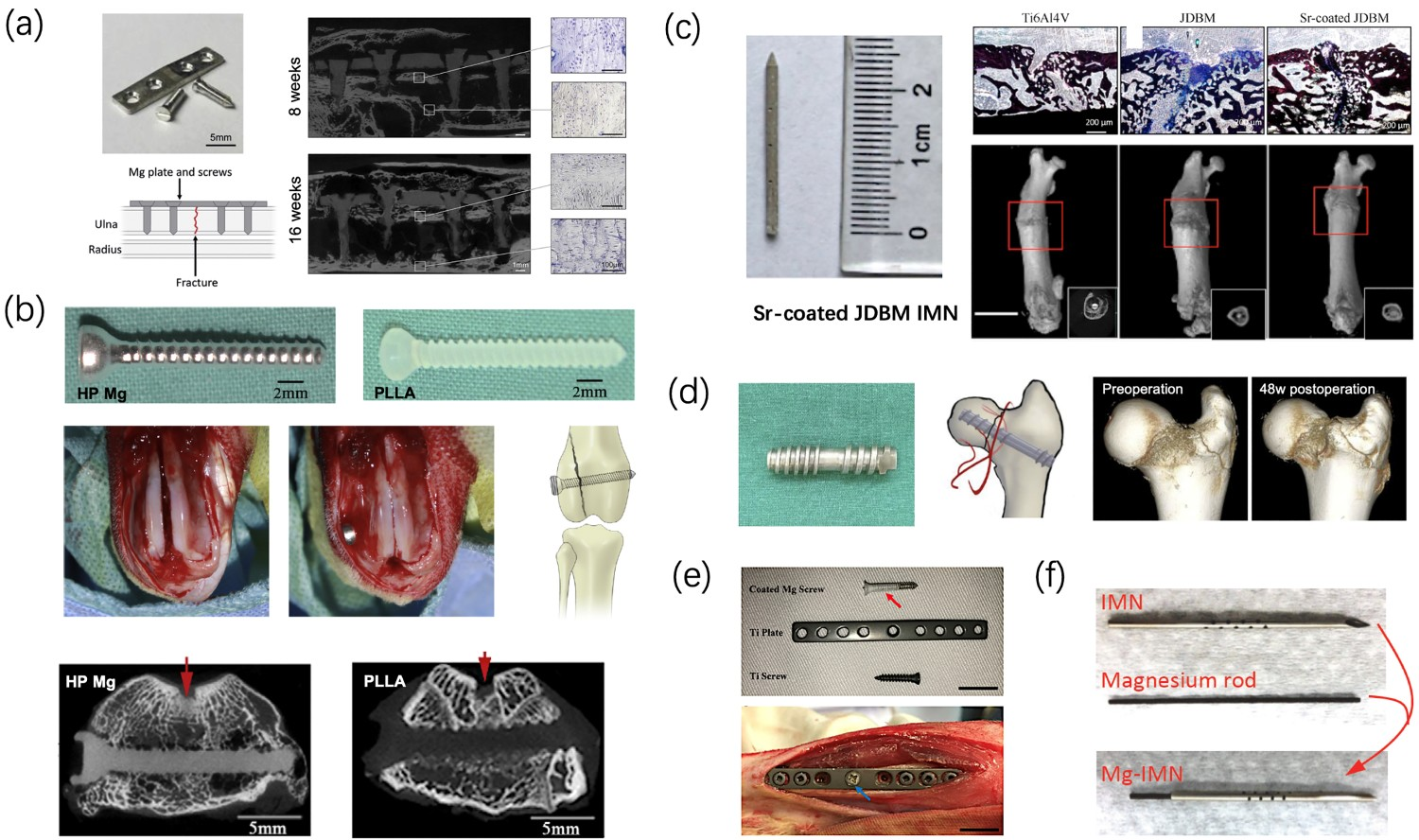
Mg-based load-bearing fixation devices showed acceptable mechanical stability for applications such as bone-fracture fixation and osteosynthesis [380–382]. A standard-sized Mg-Zn-Ca alloy plate screw afforded considerable stability for fixating facial bone fractures of beagle dogs in the early bone-healing process [381]. Similarly, the mechanical strength of an extruded WE43 alloy plate screw was sufficient for repairing LeFort I osteotomy in beagle dogs [382]. Large pure-Mg screws had sufficient mechanical strength for repairing femoral neck fractures in goats (Figure 4(d)) [380]. Despite these results, the mechanical strength of Mg-based alloys remains a major concern in load-bearing applications as degradation proceeds, especially when Mg-based alloys degrade quickly [272]. One solution to this problem is to develop Mg-based hybrid implants with partial or decelerated degradability and accelerated bone-healing ability, such as a Mg-Ti plate-screw system (Figure 4(e)) [278] and a Mg-SS IMN (Figure 4(f)) [20]. For instance, a Mg-SS IMN accelerated the bone-healing process of rat OPF in comparison to that with SS IMN by increasing callus- and endochondral-tissue formation [20]. Most recently, a Mg-containing IMN has demonstrated the ability to rescue bisphosphonates-impaired fracture healing via elevating CGRP synthesis and release [383]. Fast osseointegration is critical to the success of bone-fixation devices by establishing bone/implant interfacial mechanical stability. Surface coating is an effective strategy to improve the osseointegration ability of Mg-based alloys [154,273]. In addition, porous screws afford improved osteointegration due to enhanced mineralization and vascularization [384].
Mg-based alloys have also shown promising results in anterior cruciate ligament reconstruction [139,250,279,385–388]. For example, as-extruded pure-Mg hollow interference screws increased the levels of secreted PDGF-BB in the bone marrow, the formation of osteoid at the tendon graft/bone interface, bone mineralization and the hardness of the interface, and improved the migration of BMSCs towards the peri-implant tissues [139]. The authors also revealed that Mg-6Zn-0.5Sr screws enhanced bone formation in the peri-tunnel region and the mechanical stability of the femur-tendon graft-tibia complex, as well as the preservation of peri-tunnel bone mass compared to those observed with poly-lactic acid (PLA) screws [250]. Similarly, in the rabbit anterior cruciate ligament reconstruction model, it was revealed that the tendon-bone healing, the relative area of fibrocartilage at the interface, and the fibrocartilage transition zones in the pure Mg group were superior to those of the Ti group [385].
Nevertheless, it is important to mention that bone union was inhibited by WE43 alloys compared to those with the Ti controls in some animal studies [154,273]. Thus, the detailed mechanisms of Mg-based alloy-mediated bone-fracture healing, including endochondral and intramembranous ossification, should be further investigated. For example, the interaction of Mg-based alloys with periosteal stem cells should be further explored, since it is essential for the repair of atrophic nonunion fractures that are caused by severe damage to periosteal mesenchymal progenitors [389,390].
Fusion cages and bone cement are widely used in spinal surgery for intervertebral and vertebral augmentation. The potential of Mg-based alloy cages for intervertebral fusion has recently been explored. However, the feasibility of Mg-based alloys in spinal fusion remains unclear due to negative results in several preliminary studies. For example, a hybrid cage with AZ31 alloy skeleton which was covered and infiltrated by poly-ϵ-caprolactone (PCL) (Figure 5(a)) showed no signs of fusion, but progressive encapsulation over time in a sheep cervical spine interbody fusion model [391]. The authors speculated that the PCL prevented excessively fast degradation of the AZ31 alloy, and hindered bony growth through or around the cage. Similarly, spine fusion was not achieved when using a Mg–Zn alloy (Figure 5(b) [392]) or AZ31 alloy cages (Figure 5(c) [393]). The authors suggested that intervertebral excessive-Mg accumulation could be responsible for the failure of interbody fusion [393]. Because of these unsatisfactory results, more rational design of Mg-based cages to ensure suitable biological functions and mechanical stability becomes critical. Mg-based alloys have also been used in the fabrication of novel bone cement. To avoid fast degradation and excessive Mg accumulation, surface-degradable bone cement (SdBC) was developed for spinal surgery by incorporating pure-Mg particles into clinically-used poly(-methylmethacrylate) (PMMA) bone cement [394,395]. The SdBCs maintain mechanical robustness of the PMMA bone cement, while possessing enhanced osseointegrative, angiogenic, and anti-infection properties that are lacking in the PMMA cements. Animal studies reveal this new bone cement may improve the treatment outcomes of various orthopaedic surgeries from kyphoplasty to joint arthroplasty.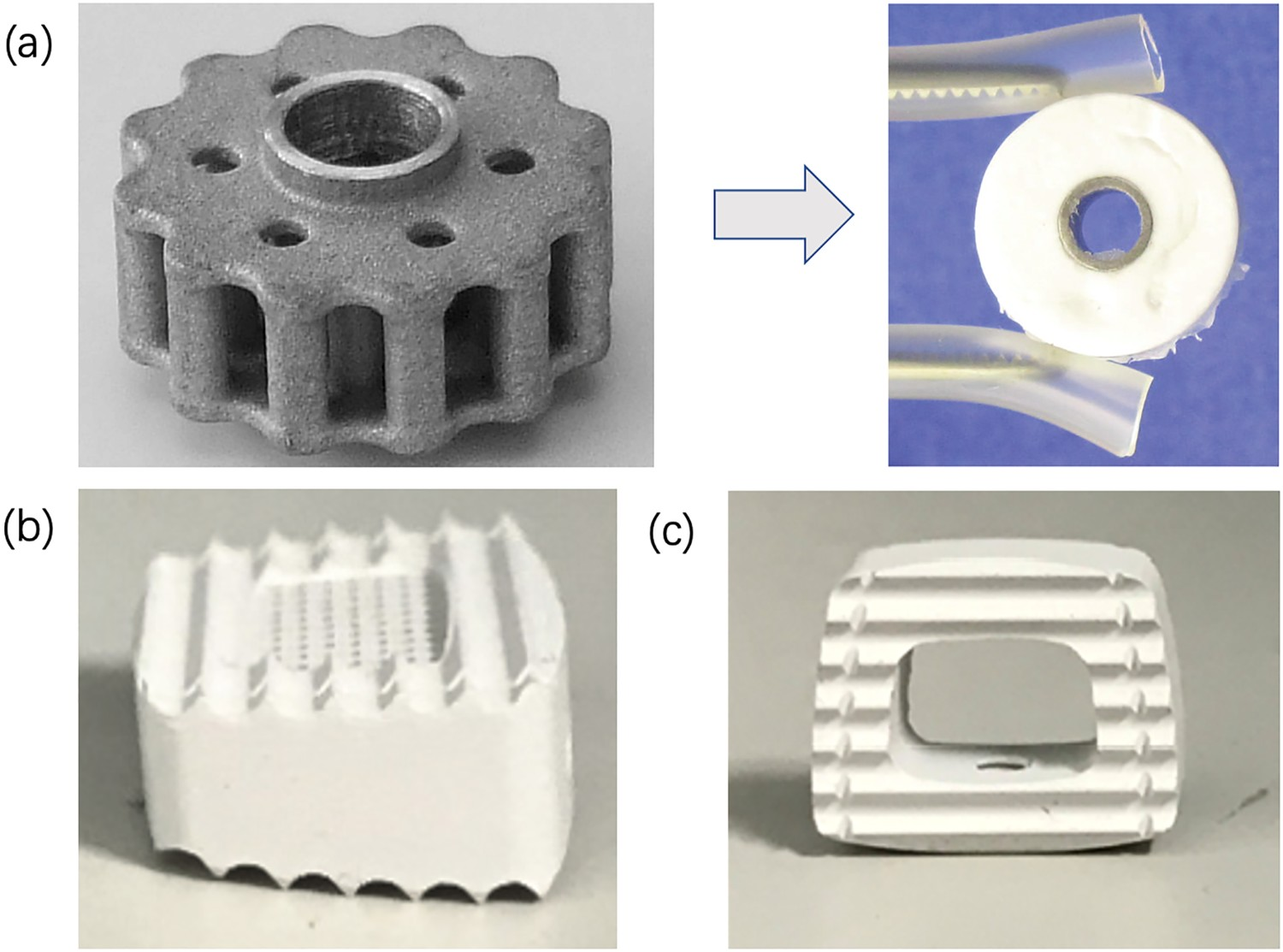
Although there are concerns about the efficacy and safety of Mg-based alloys, clinical studies have been conducted to validate the feasibility of Mg-based alloy fixation devices in the treatment of bone deformities and fractures, including mild hallux valgus deformities [268,396–398], distal radius fractures [156], lateral malleolus fractures [399], medial malleolar fractures [400], tibial spine avulsion fractures [401], osteochondral lesions of the talus [402], and mandibular condyle fractures [403]. The feasibility of pure-Mg screw-fixed bone flap transplantation for the treatment of femoral head osteonecrosis was also investigated [280,404]. Notably, MgYReZr screws (Syntellix AG, Germany) were approved with the Communauté Européenne (CE) mark in 2013. MgCaZn screws (U & I company, Korea) were approved for clinical use by the Korea Ministry of Food and Drug Safety in April 2015. Pure-Mg screws (Eontec, China) were officially approved for multicenter clinical trials for the treatment of steroid-induced osteonecrosis by the China National Medical Products Administration in July 2019 and were approved with the CE mark in May 2020.
Cardiovascular stent
The limitations of permanent metallic cardiovascular stents include long-term endothelial dysfunction, delayed re-endothelialization, thrombogenicity, permanent physical irritation, and chronic inflammatory local reactions [405]. Besides, the mismatch in the mechanical behaviours of the stented and non-stented vessel areas, inability to adapt to growth in young patients, and non-permissive characteristics for later surgical revascularization are also potential problems [405]. In 2000, the possibility of using Mg-based alloys for cardiovascular stents was investigated for the first time [2,128], revealing that neointima formation was decreased significantly when the stent started to degrade. However, complete degradation of the stent occurred after 89 days, which is much faster than expected. After implantation into the coronary artery of minipigs [406], the WE43-alloy-based ‘Lekton Magic Coronary Stent’ resulted in a larger minimum luminal diameter (MLD) compared to that observed for the 316 L SS stent-treated group within 12 weeks, indicating less neointima formation and positive remodelling [406]. Recently, a comparative study demonstrated that use of a WE43 wire resulted in a minimal inflammation response in the arterial wall until its complete degradation, while both the Zn- and SS-treated groups experienced similar and persistent inflammation responses which induced the formation of fibrotic capsules and necrosis [141]. Despite these positive results, the long-term degradation mechanism of Mg-based stents in arterial walls is still unclear and remains a major concern in terms of their biosafety. The degradation mechanism of a bare Mg–Nd–Zn–Zr stent prototype in the common carotid artery of New Zealand white (NZW) rabbits was studied during a 20-month implantation (Figure 6(a)) [407]. The stent had good safety and efficacy with a complete re-endothelialization within 28 days. The stent struts were mostly replaced in situ by degradation products in 4 months, during which the volume and Ca concentration decreased gradually without observation of enrichment of the alloying elements Mg and Zn in any of the main organs [407]. Based on the positive results, the authors developed a shape-optimized Mg–Nd–Zn–Zr alloy stent with a rapamycin-eluting polymer coating [408], and evaluated it in the iliac artery of NZW rabbits. The coated stent resulted in neither thrombus nor early restenosis, supported the vessel effectively until degradation after 5 months, and allowed arterial healing [408]. Animal studies and clinical case analysis of Mg-based alloy vascular stents. (a) Haematoxylin-eosin (H&E) staining images and μCT 3D reconstructed images of JDBM (a Mg–Nd–Zn–Zr alloy) stents in rabbit common carotid artery at different time points [407]; (b) Optical coherence tomography 2D images of Magmaris® WE43-alloy-based stent in human coronary artery demonstrated excellent strut apposition with some struts covering the side branch post-implantation; no visible strut remnants exist; and struts initially covering the side branch being resorbed after 12 months [6].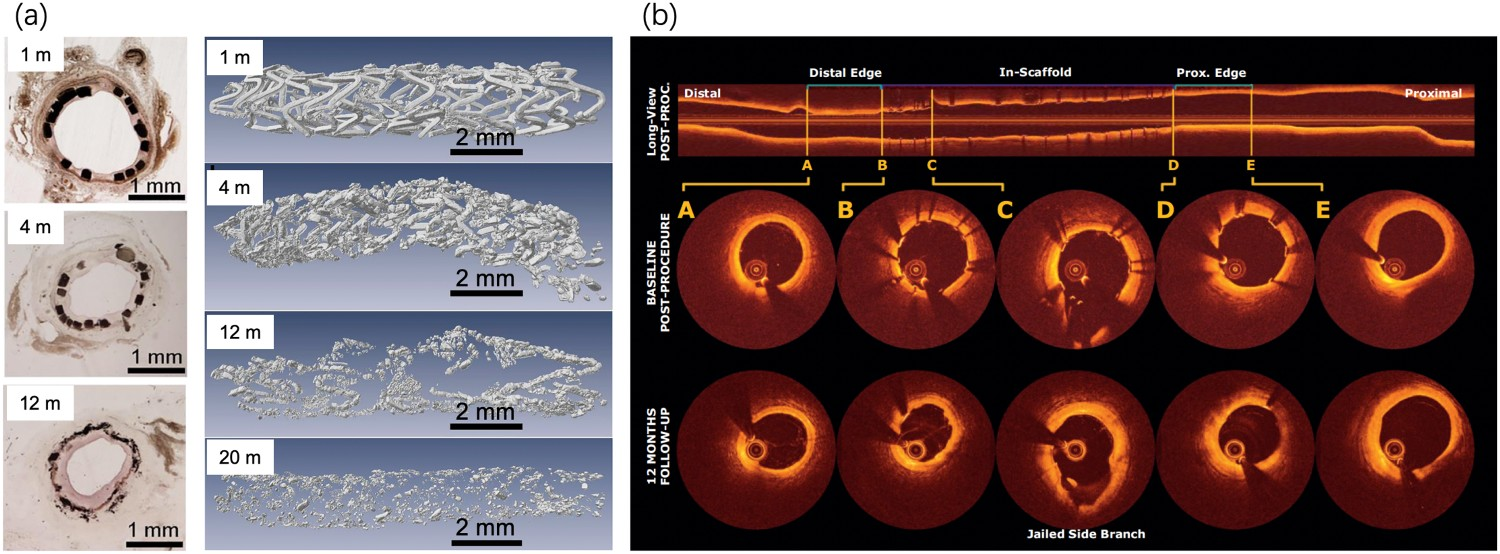
The first successful implantation of an Mg-based stent in a human was performed in the left pulmonary artery of a preterm baby suffering from a congenital heart disease [409]. A follow-up study showed its complete degradation after 5 months and no in-stent obstruction or neointimal hypertrophy was observed. This clinical trial showed that Mg-based stents may be widely applicable in clinics. Subsequent clinical studies have been performed in both peripheral and coronary vessels using the WE43-alloy-based ‘Lekton Magic Coronary Stent’ [406,410,411] and the stents were completely degraded during the 4-month follow-up, with an overall performance comparable to that of SS stents. However, a short follow-up does not allow any conclusions to be made regarding late, low-incidence events such as thrombosis. Modifications of the stent characteristics with prolonged degradation and drug elution are still required. The BIOSOLVE-I clinical trials confirmed the safety of a drug-eluting WE43 stent (DREAMS), affording promising results [412]. The subsequent BIOSOLVE-II trial showed that the DREAMS 2G stent had comparable target lesion failure and target lesion revascularization rates to those of the degradable polymer-based stents and permanent drug-eluting stents after 6–12 months, which led to CE approval of the WE43-alloy-based Magmaris® sirolimus-eluting stent (Biotronik AG, Bülach, Switzerland) in June 2016 [413]. One particularly encouraging finding of the clinical premarket studies on the WE43-alloy-based stents is that no definite or probable scaffold thrombosis was observed [406,410,411]. In a Magmaris® postmarket program, the intraprocedural data of over 2000 patients was reviewed (Figure 6(b)) [6]. Generally, the theoretical advantages of Mg-based stents (compared to polymeric stents) in terms of deliverability and conformability have translated into practice with good intraprocedural performance outcomes.
Despite of the promising results of clinical applications of Mg-based stents, there is a consensus that a better understanding of the interaction mechanism of the local vessel tissue and circulation system with the degradable stent is necessary for the further improvement of stent safety and efficacy. In addition to the alteration of mechanical properties of stents during degradation, the overall biomechanical properties of blood vessels also change during tissue remodelling/growth after stent implantation due to the changes in wall thickness, fibre stretching, maximum wall stress, and material properties (stiffness, anisotropy, and viscoelastic characteristics) [414–416]. Biomechanical changes in the stent and blood vessels during stent degradation and vascular remodelling/growth are yet to be understood [416]. This knowledge is essential to determine the optimal supporting stress for different sites and remodelling stages of blood vessels and prevent side effects by mechanical disturbance. The long-term effects of degradation of Mg-based alloys on vessel repair and remodelling is also unclear, although it is well accepted that a better understanding of the long-term degradation mechanism (including loss of biomechanical function and metabolism of the degradation products) is the prerequisite for answering the above questions.
Surgical instruments for hemostasis and anastomosis
Biodegradable Mg-based alloy clips, staples, and rings have been developed for soft-tissue anastomosis such as skin wound closure and hemostasis, which can potentially reduce the risk of postoperative bleeding due to device shift and persistent inflammation, compared to traditional nondegradable counterparts. The secondary surgery to remove the devices from dense tissues after recovery, which may result in secondary injuries and pain to the patient, can also be avoided. On the canine cholecystectomy, the Mg-0.2Zn-0.1Ca hemostasis clip showed a sufficient sealing capability and excellent biocompatibility, and also prevented the formation of artefacts in the CT scan [417]. The Mg–Zn–Ca and Mg–Zn–Ca–Y alloy clips successfully ligated the carotid artery without blood leakage after surgery [56,418]. Histological analysis and biochemical parameters of blood showed no tissue inflammation around the clips. The Mg–Zn–Ca–Y clip degraded completely after eight months. Coated Mg-2.8Zn-0.8Ca clips exhibited good biocompatibility when applied on rabbit uterine tubes for five weeks (Figure 7(a)) [419,420]. Notably, a pure-Mg clip was recognized as an innovative medical device by CFDA in 2018 (https://www.cmde.org.cn/xwdt/shpgzgg/cxyxgsh/20180308143746124.html). Animal studies of Mg-based surgical instruments for hemostasis and anastomosis. (a) Mg-Zn-Ca-Y alloy clip occluded the proximal and telecentric stump of rat carotid blood vessels (i), and cuts the blood vessel from the middle of the two hemostatic clips (ii) [420]; (b) Pure-Mg staples for anastomose small intestine (i), and no bleeding and intestinal fluid exudation after anastomosis (ii) [421]; (c) Mg–Zn–Sr intestinal anastomosis ring (i) and surgical procedure of intestinal anastomosis(ii) [422].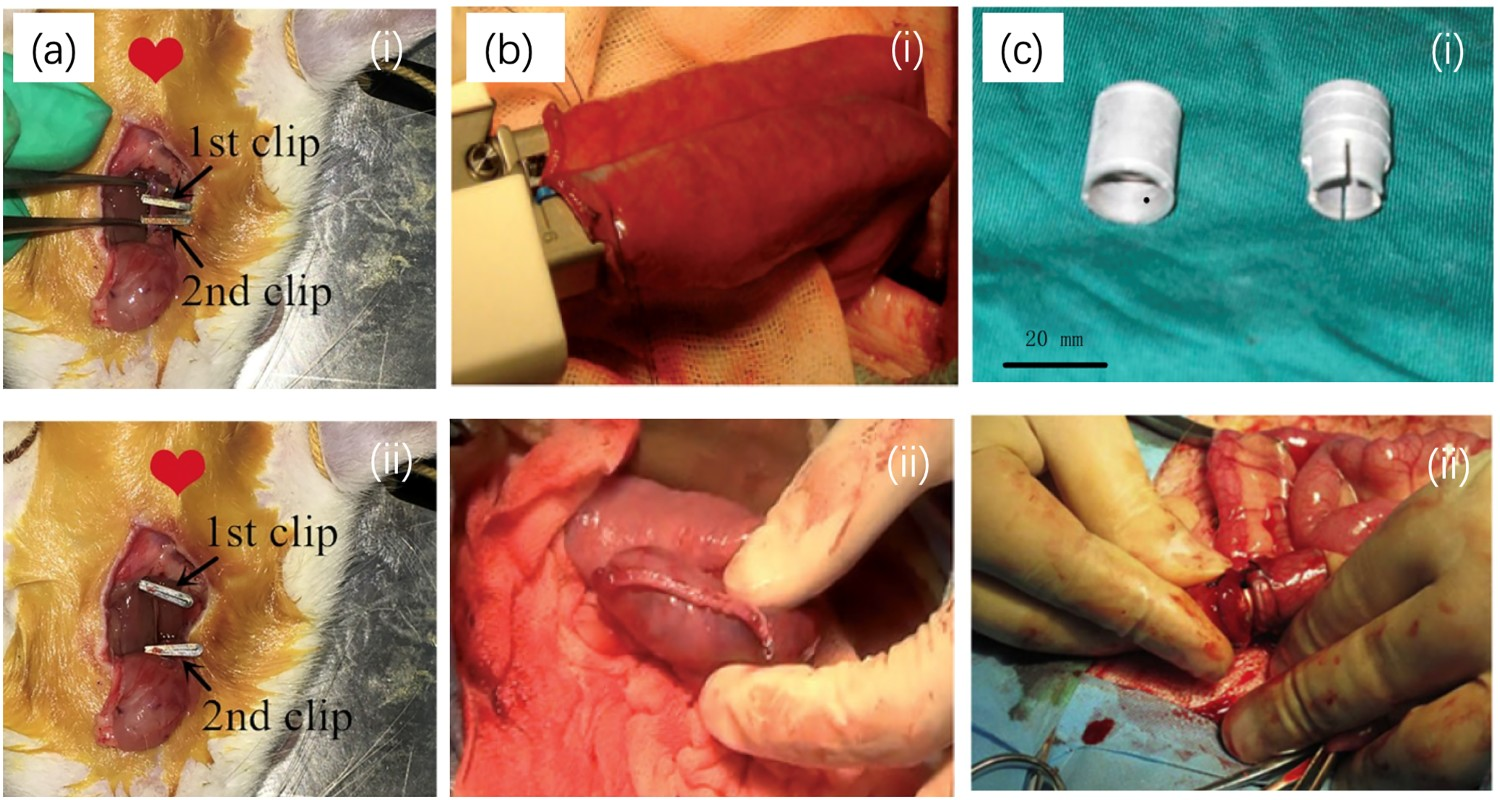
Mg-based alloy staples also showed high efficacy and biocompatibility for soft tissue closure. For example, porcine stomach was successfully closed using the pure-Mg staples (Figure 7(b)) [421,423]. These staples kept good closure of the anastomosis site without leakage and obvious inflammatory response. The staples also exhibited no fracture or severe corrosion cracks during degradation. In the porcine intestinal anastomoses, Mg–Nd–Y alloy staples did not cause any severe complications such as anastomotic leakage, haematoma, adhesion, necrosis, and serious inflammation reactions [424]. Similar findings were obtained with Mg–6Zn staples in intestinal anastomosis [425]. Pure-Mg staples inhibited the inflammatory response in rectal anastomoses through TLR4/NF-κB and VEGF signalling [426], providing a biological basis for prospective applications in soft tissue repair. Additionally, Mg-based alloys are promising candidates for the fabrication of biodegradable intestinal anastomosis rings [422,427]. For example, after being implanted into the intestinal tracts of Bama miniature pigs (Figure 7(c)) [422], Mg–Zn–Sr alloy anastomosis rings induced only a mild inflammatory response, mediated the healing of intestinal muscular and mucosal layers similar to their healthy counterparts, and did not cause pathological changes to important organs.
The investigation of Mg-based alloys for hemostasis and anastomosis of soft tissues is still at an early stage, and device optimization remains a challenge. Biological effects of Mg-based alloys on soft-tissue healing processes remain to be determined [143,426], and are highly dependent on the alloy composition and degradation nature [143]. Moreover, the degradation behaviour should be optimized to match the requirements of soft tissue repair [419].
Tissue engineering scaffolds
Repair of segmental bone defects greater than critical sizes is a significant challenge in orthopaedics [429]. Porous Mg-based alloys are promising materials for fabricating bone tissue engineering scaffolds [429,430]. The potential of Mg-based alloys scaffolds has been evaluated in large bone defect models. Porous Mg-based alloys assist bone defect repair by facilitating bone and vascular ingrowth. A porous Mg–Nd–Zn–Zr alloy scaffold coated with brushite perfectly repaired large bone defects in rat and rabbit models by effectively stimulating angiogenesis, osteogenesis, and bone remodelling (Figure 8(a)) [431]. Open-porous pure-Mg scaffolds induced high levels of bone and blood vessel formation, as well as collagen type I and OPN expression in the lateral epicondyle defect of NZW rabbits (Figure 8(b)) [167]. Porous pure Mg promoted vascularization in the critical-size murine calvarial bone defects [432]. Tubular Mg–Zn–Ca and Mg–Sr alloy scaffolds showed potential in the repair of ulna segmental defects (Figure 8(c)) [433,434]. Structurally biomimetic Mg-based alloy scaffolds have been evaluated for simultaneous repair of cortical and cancellous bone. A biomimetic porous pure Mg improved the bone formation in a rabbit femoropatellar bone defect model (Figure 8(d)) [435]. A biomimetic Mg3Zn1Mn alloy implant with an open-cell porous interior and an outer solid wall expedited the healing process in a segmental defect model of the NZW rabbit (Figure 8(e)) [436]. Mg-based tissue engineering scaffolds for bone defect repair. (a) Digital and scanning electron microscope (SEM) images of Mg/JDBM-MgF2 scaffold without and with brushite (DCPD) coating. μCT images showing the new bone and vascular formation in the defect area after 4 and 8 weeks (red or white line: bone defect area) [431]; (b) SEM and 2D μCT images of Mg scaffolds; 2D μCT images (red arrows: new bone) and alizarin red S and calcein sequential labels of new bone after 16 weeks [167]; (c) MAO-coated tubular Mg–Zn–Ca scaffold for ulna bone defect repair and X-ray observation after 2, 4, 8 and 12 weeks [433]; (d) A biomimetic-porous Mg material coated with HA/(PEI-SiO2) hybrid layer for femoropatellar defect repair, and a μCT image of femoropatellar bone and the porous Mg [435]; (e) A biomimetic-Mg scaffold for humerus defect repair and X-ray images at various periods [436]; (f) μCT and SEM images of porous alginate/gelatin hydrogel with Mg powder. μCT images, sequential fluorescence staining, H&E staining, and OSX/CD31 immunofluorescence staining of bone formation in defects after 3 weeks, and μCT images of 3D vasculature in defects after 2 weeks, in Blank, Mg free (−Mg) and Mg containing (+Mg) hydrogel groups [437].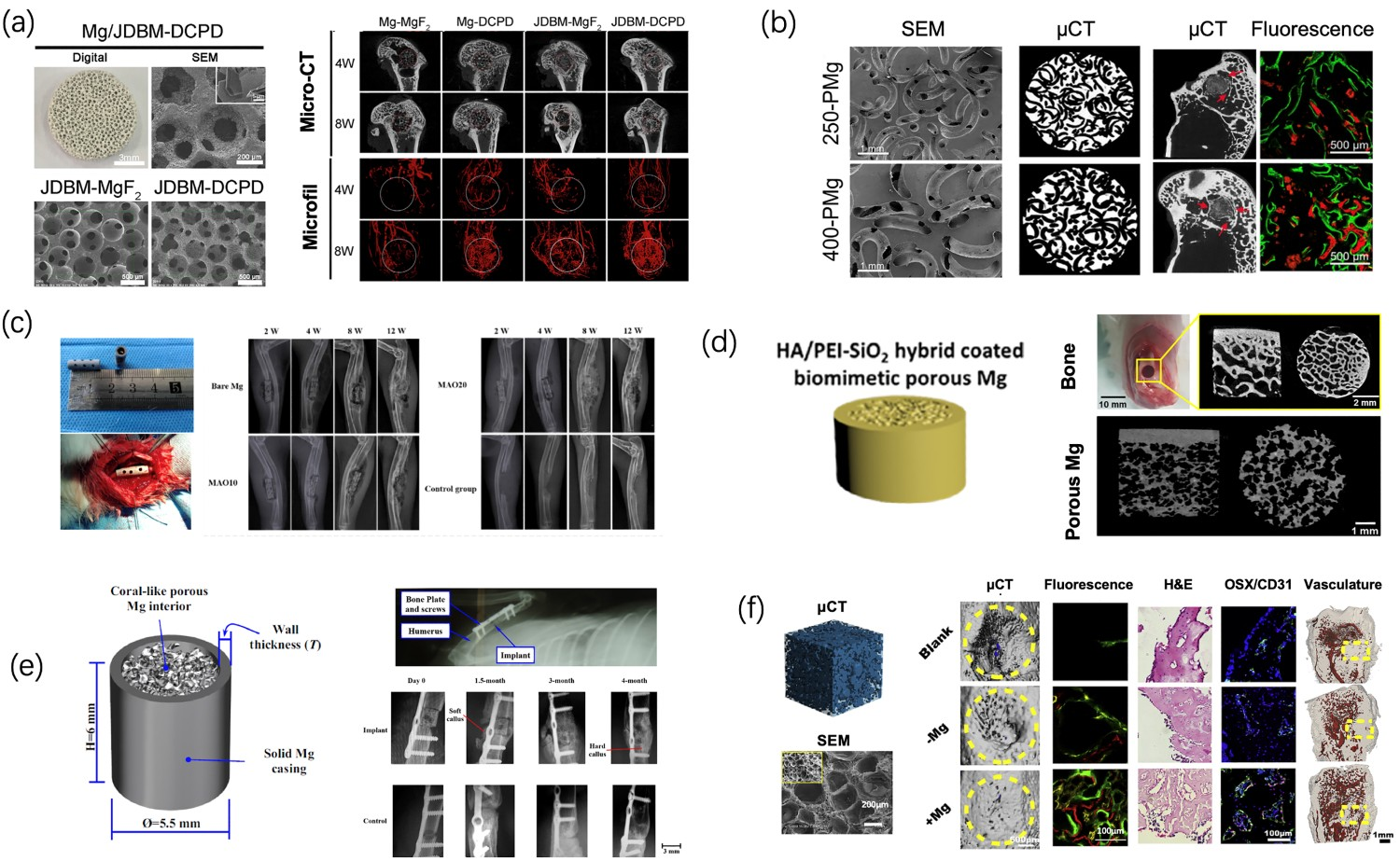
Mg-based-alloy-comprising composite scaffolds reveals well-controled release profile of degradation products [438]. Poly (lactide-coglycolide) (PLGA)/tricalcium phosphate (TCP)/pure Mg porous scaffolds induced more newly mineralized bone than PLGA/TCP scaffolds in 15 mm rabbit radii bone defects [439]. Additionally, the PLGA/TCP/pure Mg porous scaffold showed synergistic osteogenic and angiogenic effects, which enhanced new bone formation and strengthened the newly formed bone quality in a rabbit steroid-associated osteonecrosis (SAON) model [84]. The effects could be due to Mg2+-enhanced blood perfusion after SAON [440]. Notably, this novel scaffold was approved for clinical study as an innovative medical device by CFDA in 2018 (https://www.cmde.org.cn/xwdt/shpgzgg/cxyxgsh/20180613133900434.html). Although the mechanism remains to be revealed, Mg-containing materials can induce vascularized bone regeneration [84,183,263,437,438]. For instance, pure-Mg-particle-modified hydrogel scaffolds induced extensive vascularized bone regeneration in femoral-defect repair in rats (Figure 8(f)) [437].
Owing to their robust mechanical properties and osteogenic capability, Mg-based alloys have been widely used in the engineering of bone tissue. However, the biological implications of Mg-based alloys in inflammation modulation, angiogenesis, microbial inhibition, and Ca antagonism afford potential applications in soft and connective tissue engineering for the treatment of challenging conditions such as diabetic wounds, volumetric muscle loss, and cartilage damage. For example, Mg-Cu-alloy-particle-containing hydrogel demonstrated great potential in the treatment of severe skin wounds by accelerating wound contraction and improving tissue-repair quality [174]. Composite techniques simultaneously benefit the development of a scaffold with soft-tissue-biomimetic structural and biomechanical properties, as well as optimized degradation rate and degradation product release behaviour, to allow effective tissue repair by restoring biological/mechanical homeostasis at the defect and optimizing the tissue regeneration paradigm.
Summary and outlooks
Biosafety evaluation of Mg-based alloys
As discussed in the previous sections, ideal Mg-based implants are expected to degrade at an optimal rate in vivo with appropriate host responses and eventually degrade completely or partially upon fulfilling their mission to assist with tissue healing. Meanwhile, the released degradation products or implant residues should be metabolized or assimilated by human or animal body. The biocompatibility requirements of Mg-based alloys in a specific application include: (1) complete dissolution with the passage of corrosion products or metabolization/assimilation by the cells and/or tissues, and (2) induction of an appropriate host response during degradation period toward fully degradation. Also as mentioned above, the biocompatibility of Mg-based alloys is more complex than that of traditional nondegradable metals. There is evidence supporting the fulfilment of the first requirement, but achieving the ‘appropriate host response’ is a great challenge currently faced by researchers. First, host responses to Mg-based alloys are complicated and intertwined. Second, the host responses during the degradation process of Mg-based alloys change dynamically depending on at least degradation rate, metabolic rate of degradation products, and the concentration-dependent tissue/cellular reaction to the degradation products. These factors all vary with the material composition and structure, and implantation site-specific conditions. Third, the biological mechanisms underlying some host responses specific to Mg-based alloys remain unclear.
Therefore, one of the key issues for re-defining the biocompatibility concept of Mg-based alloys is the identification of the ‘appropriate host response’. Degradation of Mg-based alloys and its host responses exhibit spatial–temporal dynamic changes in vivo. Thus, the biocompatibility evaluation methodology should also be re-considered together with the following dynamic characteristics. Biological impacts of Mg-based alloy degradation process and products. The progressive degradation of Mg-based alloys causes temporary or permanent changes in the microenvironment of surrounding tissues, causing constantly changing biological effects (either beneficial or adverse). The definition of adverse effects (mainly including pain, mechanical weakness and dysfunction of tissue, bone lysis, and H2 gas accumulation [441]) and their severity levels are critical to the biocompatibility evaluation and clinical translation of Mg-based alloys. However, the definition of adverse side effects varies significantly among scientists. For example, in an animal study, ZEK100 (0.96 wt.% zinc, 0.21 wt. % zirconium, 0.3 wt. % RE, Mg in balance) alloy induced temporary changes in the bone mass and microstructure, but there was no pathological alteration in important organs (liver, spleen and kidney) or serum Mg concentration [21]. The authors suggested excluding ZEK100 from further biomedical investigation because of the severe bone morphological changes. In a clinical study, the MgYREZr alloy-based screw showed signs of radiolucency, screw loosening, osteolysis, and bone resorption or demineralization in 40% of the cases. However, none of patients exhibited obvious clinical symptoms like pain [268]. Therefore, there is an arguable opinion that surgeons, radiologists, and patients should not be concerned about these mild side effects, as they are an inherent part of the Mg degradation process. The metabolism process and pathways of degradation products. The decomposition, delivery assimilation and excretion mechanisms of degradation products are related to the temporary alteration of element concentration in local tissue and blood serum, as well as the temporary element accumulation and potential pathological alteration in important organs [442,443]. Meanwhile, metabolic mechanism of degradation products is very different from those from oral-administration analogues [443]. The metabolic process and pathway, which determine the biosafety of Mg-based alloys in specific tissues, varies with the implantation site and species [77,407,443] due to the differences in the anatomical and physical properties of tissue (such as H2 permeability [444,445]). Although the metabolic mechanism of implant Mg has received attention, studies rarely reveal the metabolic pathway and efficiency of alloy elements, which are substantially different from those of Mg element [442,443]. Generation of H2 and OH− are unique for Mg-based alloys, for which the metabolism in specific tissues requires more investigation because of the risk to damage physiological system when they overburden the organism’s regulating mechanisms [443]. The long-term effects on tissues/organs during and after the degradation of Mg-based alloys. There are numerous studies showing that major organs have a high tolerance to the degradation products of Mg-based alloys, without permanent Mg2+ ion accumulation, damage or dysfunction [21,77,84,147,272,280,407,446–450], even for the rapidly corroding Mg-based alloys or in a renal failure model [451]. In addition, there are animal and clinical studies reporting the recovery of bones [145,156,401,446] and blood vessels [407] after the complete degradation of several Mg-based alloys. Nevertheless, both short- and long-term studies on animals and humans are required, particularly on rapidly corroding Mg-based alloys [168]. In addition, the biological consequence of accumulated alloying elements of Mg-based alloys in organs require further investigations [145,272,447,452].
Based on current understandings, the ‘appropriate host responses’ refers to at least three aspects. First, the tissue repair process is not inhibited or compromised by the use of Mg-based alloys. Second, the temporal tissue responses during Mg-based alloy degradation do not cause adverse effects with clinical manifestation or significantly increase the risk of tissue/organ damage and implant failure. Third, the tissue/organ can fully recover or return to a homeostatic state after the degradation of Mg-based alloys. There are reports revealing that Mg-based alloys (and their insoluble degradation products) are not completely degraded or absorbed in vivo for up to 1 year [21,77,149,448]. Also, severe inflammation and osteolysis are likely to occur at the later stages of degradation [124–126]. Therefore, it is suggested that the host responses of a Mg-based alloy should be evaluated over the entire life cycle of the degradable medical device if possible, or at least for a reasonably prolonged period after degradation.
Implant design based on the biological implications of Mg-based alloys
The biological implications of Mg-based alloys indicate their rich restorative opportunities for biomedical applications. Thanks to great advances in material fabrication and processing techniques, Mg-based alloys with tailored composition, geometry, mechanical properties, and 3-D structure have been developed. Further understanding of the biological implications of Mg-based alloys is becoming an important guide for more rational designs of Mg-based alloy comprising implants such as hybrid orthopedic fixation systems, neural conduit, and tissue engineering scaffolds.
However, the degradation- and implantation-site-dependent biological responses, multifaceted effects of Mg-based alloys on tissue quality (including volume, chemical composition, micro/nanostructures, and mechanical properties), and limited understanding of underlying mechanisms clearly indicate that it is still challenging to take the advantages of Mg-based alloys for extensive human applications. Obviously, understanding the biological implications of Mg-based alloys in therapeutic contexts is one of the key prerequisites for exploring the potential applications of Mg-based alloys and optimizing the implant design accordingly.
In a rational design of Mg-based implants, the material composition, intrinsic degradation behaviour including degradation products, and physicochemical properties (e.g. volume, morphology, surface chemistry and topography, porosity, residue stress, etc.) should be first considered. The selection criteria of the material parameters mentioned above depend on the characteristics of the implantation site and target applications, such as the cause and severity of tissue lesion, the tissue intrinsic-repair capacity and mechanism, the tolerance and metabolic capacity of local tissue to the degradation products, as well as the local blood circulation and mechanical conditions. The Mg-based alloys can also incorporate with other biodegradable or non-degradable materials (i.e. to form composite or hybrid materials) to achieve suitable mechanical and biological properties or to control the spatio-temporal release profile of degradation products. But new problems may arise from the biological interference between degradation products from different types of materials. For example, a study on hyaluronic acid/polygalacturonic acid hydrogel containing Mg–Ca alloy cannulated screws reported thatthe inappropriate elution kinetics of Ca and HA from the hydrogel may inhibit the positive effect of the alloys on osteoblast differentiation and proliferation [453].
In summary, unique biological implications of Mg-based alloys provide both opportunities and challenges for clinical applications and have attracted significant interest from both material engineers and clinicians. Material development and device optimization based on these biological implications can provide more possibilities for tissue repair and regeneration. Great efforts are required to deepen the understanding of the biological implications of Mg-based alloys. Meanwhile, a more rational biocompatibility evaluation method and criteria based on these biological implications are in urgent need. Advances in these aspects would significantly promote further translation of Mg-based alloys from bench to bed.