
Abstract
The aim of this study was to compare results of transtibial amputations performed using the Burgess or Modified Burgess techniques with those performed using the Bruckner technique. Transtibial amputation (TTA) was performed in 117 patients with Fontaine phase IV chronic arterial occlusion. Fifty-six patients with a mean age of 51.4 years were amputated by the Burgess technique between March 2000 and January 2003; and 61 patients with a mean age of 47.8 years were amputated by Modified Burgess technique between February 2003 and March 2006. In the Burgess technique, all muscles in the amputation region were preserved and the stump was closed by a long posterior flap; whereas the entire tibialis anterior muscle and part of the soleus muscle distal to the amputation level were removed in the modified Burgess procedure. Stump revision was performed in nine cases (17.3%) amputated by the Burgess technique due to necrosis at the incision site and drainage caused by the peroneal and tibialis anterior muscles; however, two cases (3.6%) of the modified Burgess procedure required stump revision. The prosthesis caused skin maceration at the lateral side of the stump in five cases (9.6%) operated with the Burgess technique and in eight cases (14.5%) operated with the modified Burgess procedure. After the rehabilitation period, 43 patients (82.6%) in the Burgess group were mobilized without crutches in an average of 162.5 days; on the other hand 51 patients (% 92.7) in the modified Burgess group were similarly mobilized in an average of 101.5 days. Our retrospective study showed that the modified Burgess technique, with its advantages and disadvantages forms an alternative to the Burgess and Brückner techniques regarding TTAs.
Introduction
Transtibial amputation (TTA) is most commonly performed in peripheral vascular disease and diabetes mellitus and in more than 50% of the cases diabetic foot infection forms the sole indication of lower extremity amputation.1-7
Level of amputation plays a major role in determining the postoperative mortality.8 Studies have shown show that TTA provides better results and superior prognosis compared to transfemoral amputations.9-12 Long posterior flap technique of Burgess for TTA (Figure 1) has been commonly used since 1960s, but numerous studies on sagittal flap technique, modification of long posterior flap technique of Burgess, medial-lateral sagittal flap technique, medial dominant sagittal flap technique also exist in the literature.12-18 However, none of these techniques have proven to be superior to long posterior flap technique of Burgess.8 But in the Burgess technique, assessment of viability of the crural muscles relies upon the experience of the surgeon, thus problems of wound healing and secondary procedures due to muscle necrosis are frequently encountered.19-21 Because of these disadvantages, Lutz Brückner has modified the Burgess technique and described his own modification where muscles of anterior and lateral compartments, together with the soleus muscle and if necessary the fibula, are removed to avoid secondary procedures due to muscle necrosis and tension in the stump (Figure 2).
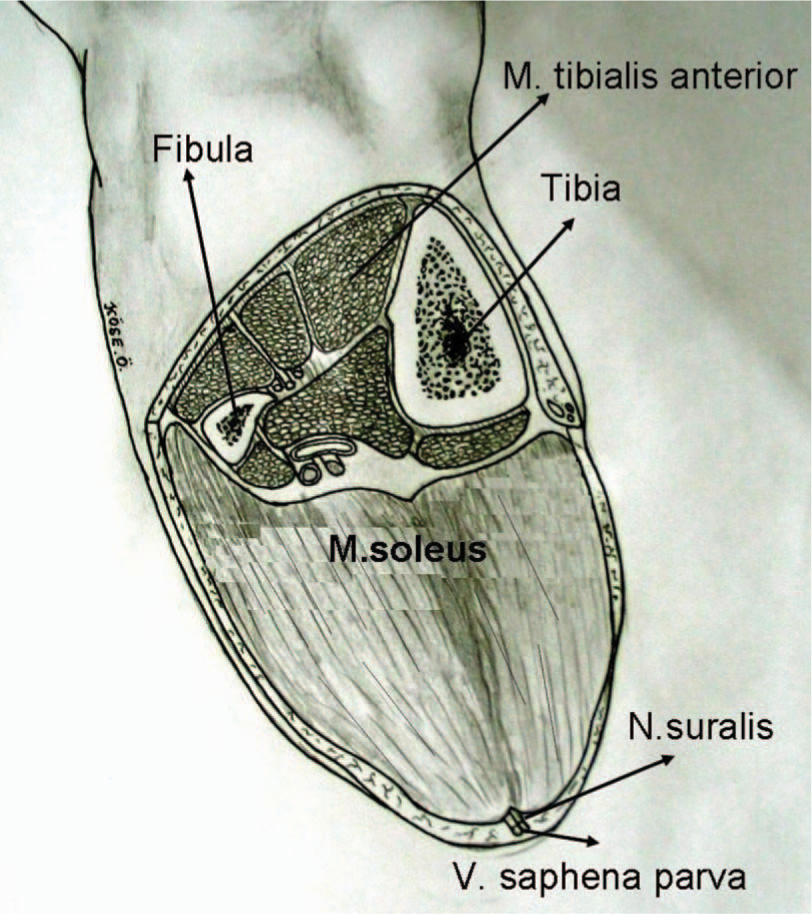
Burgess technique.
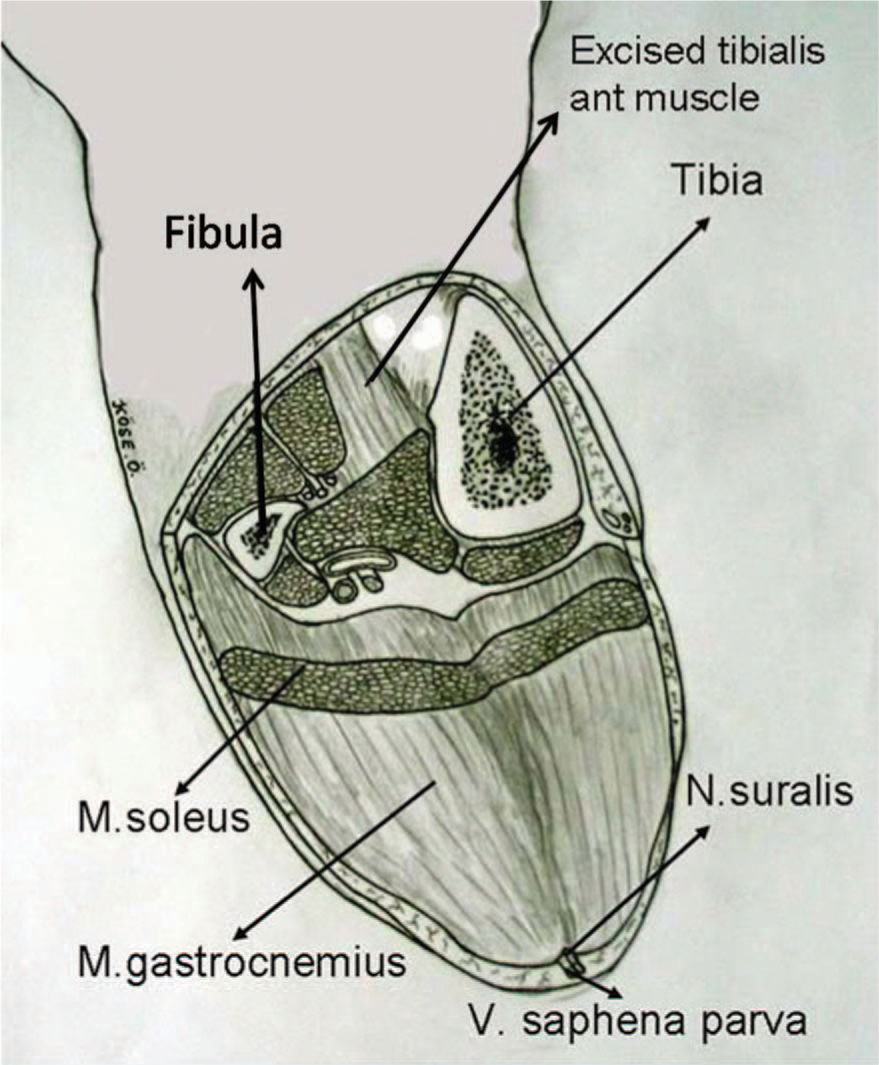
Brückner technique.
In this study, we describe a new technique modified from the Burgess technique and retrospectively evaluated the results of TTAs performed with this technique; compared these two techniques with each other and also with the results of thr Brückner technique from the literature.
Materials and methods
Patients
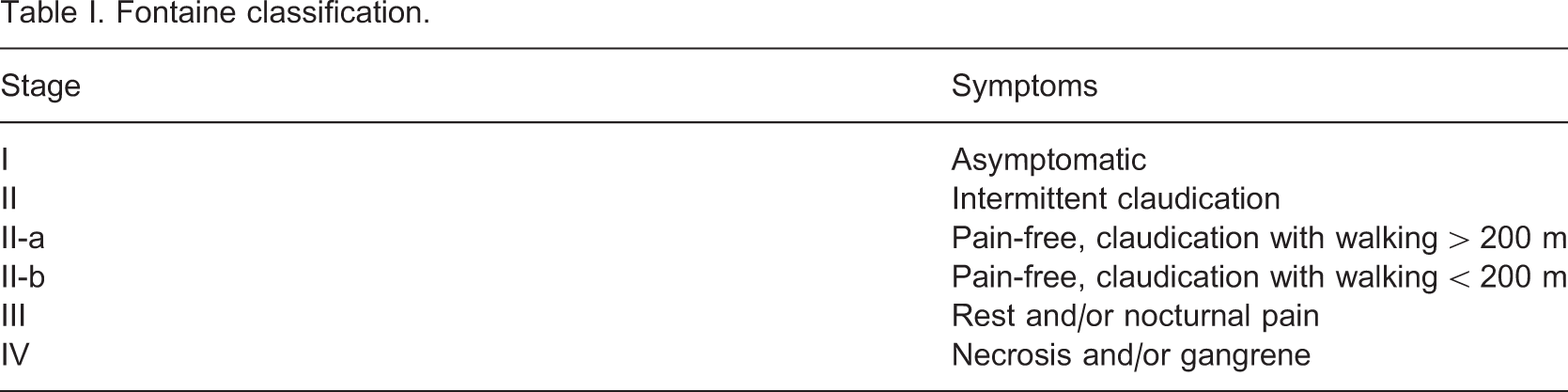
Fontaine classification
Disorders secondary to diabetes mellitus
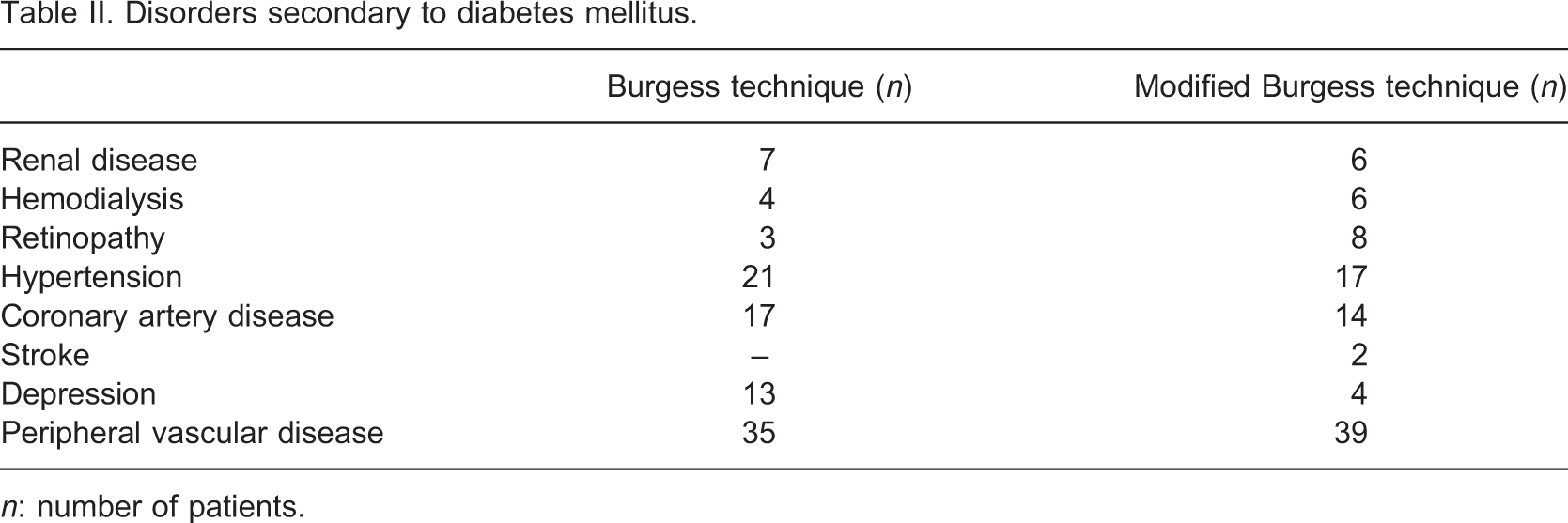
n: number of patients.
Surgical technique
In cases of the Burgess technique, all muscles in the amputation region were preserved and the stump was closed by a long posterior flap, whereas in the modified Burgess procedure, the stump was closed after removal of the entire tibialis anterior muscle and part of the soleus muscle distal to the amputation level of tibia. All patients were operated by regional anesthesia without tourniquet. For the Burgess technique, a mark was placed on the anterior of cruris 15 cm below the knee joint line to obtain an ideal stump. Another mark was placed on the posterior cruris 10-15 cm distal to the mark on the anterior cruris to provide a long posterior flap (25-30 cm distal to the knee joint line). Starting from anterior part of cruris skin; subcutaneous tissue, fascia and muscles were incised to obtain a full thickness flap. Tibial osteotomy was done perpendicular to its long axis by a Gigli wire, 10-12 cm distal to the knee joint line and was completed by 45° inclination at the anterior one fourth of the diameter of tibia. Sharp edges of tibia were smoothed by a rasper. Fibula was osteotomized 1-1.5 cm proximal to tibial osteotomy. Amputation was finished by an amputation knife started from posterior of tibia and fibula, through the distal part of the fascia of deep posterior compartment down to the mark placed in the posterior cruris. Arteries and veins were tied up by non-absorbable sutures. Nerves were stretched out and tied up from the most proximal point and cut by one hit of a sharp scalpel to prevent neurinoma formation due to mechanical compression. Soleus muscle was thinned by the amputation knife to avoid a bulky posterior flap. Drainage was placed and the fascia of the posterior flap was fixed anteriorly to the periosteum. Corners of the skin were conformed; subcutaneous tissue was closed by absorbable sutures and skin was closed by stapler. In the posterior flap technique, incision is placed out of the loading axis, on the anterior region of the stump (Figure 3).
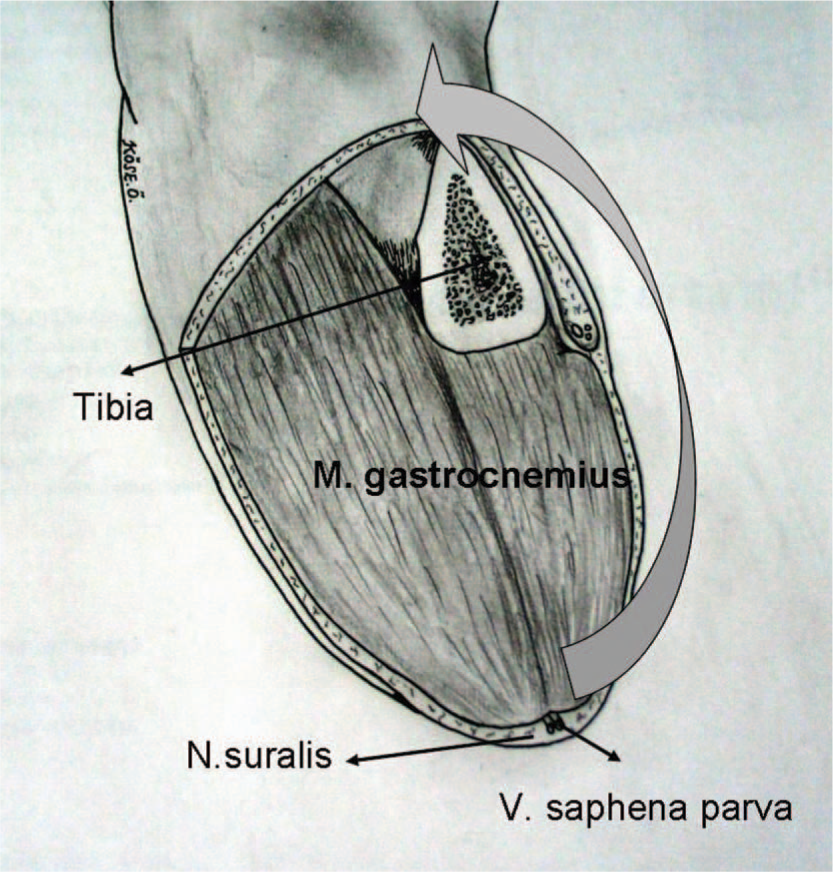
Modified Burgess procedure.
In the modified Burgess procedure; skin markings, incision site and shape, tibial and fibular osteotomies and posterior flap formation were similar to the Burgess technique. As the difference from the Burgess technique, we have completely removed the tibialis anterior muscle which is most vulnerable to ischemia.22,23 Although resistant to ischemia, soleus presents a high risk of thrombus due to relative stasis formed in its large venous plexus when posterior flap is turned to the anterior,24 thus part of the soleus distal to the tibial osteotomy site was removed to prevent its rotation (Figure 3).
The stump was covered by elastic bandage rolled as one layer, taking care not to exert any force25 throughout the first 15 days after operation. In the next 30 days, the stump was bandaged loosely from posterior to anterior to form an ideal stump. All cases were followed until functional rehabilitation was achieved with mobilization without crutches. We have used χ2 test for statistical analysis.
Results
Ischemic gangrene due to occlusion of crural arteries in diabetic patients
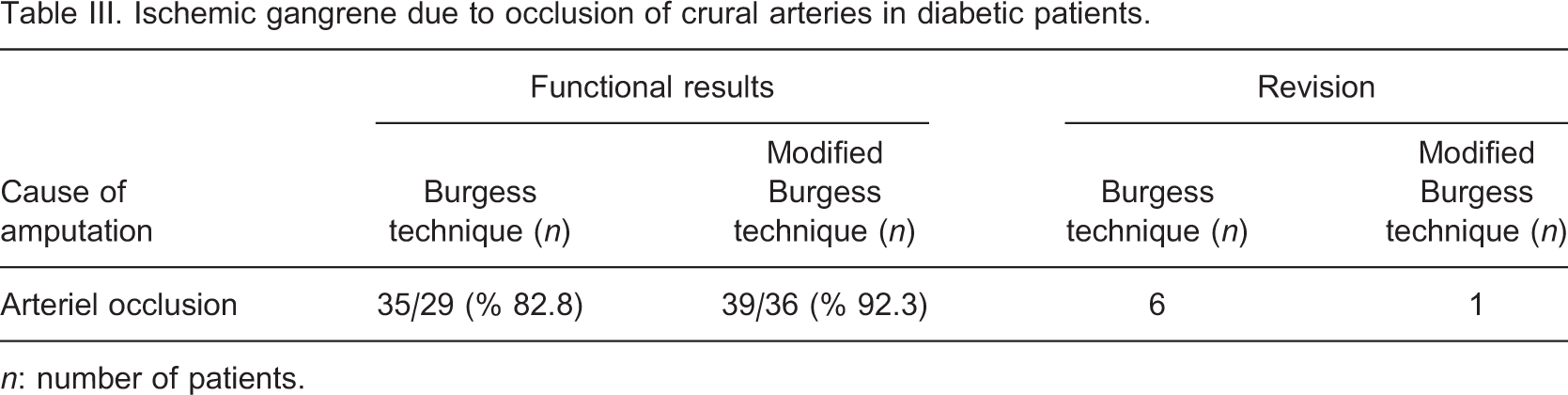
n: number of patients.
Comparison of the results of the Burgess technique and the modified Burgess technique
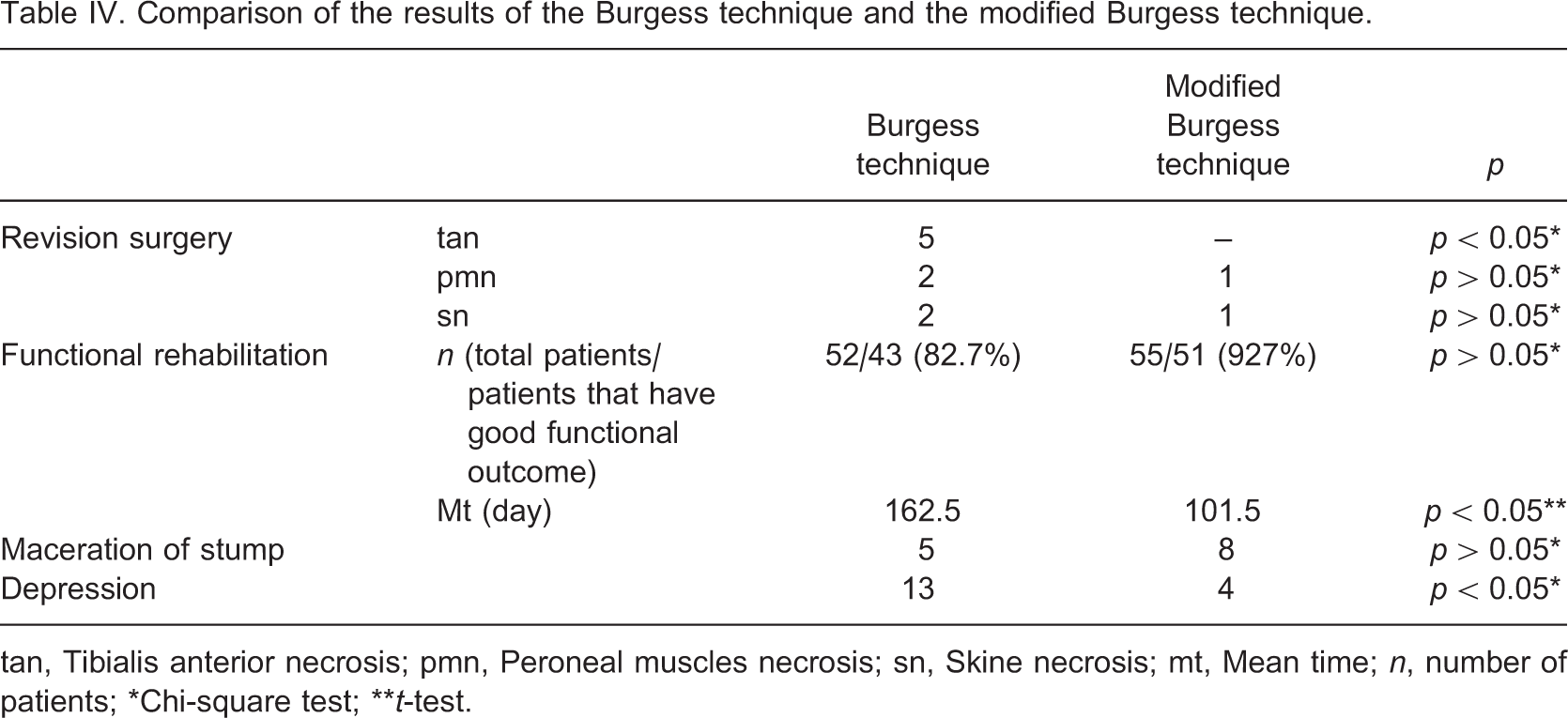
tan, Tibialis anterior necrosis; pmn, Peroneal muscles necrosis; sn, Skine necrosis; mt, Mean time; n, number of patients; ∗Chi-square test; ∗∗t-test.
Discussion
Making amputations due to chronic arterial occlusion as distal as possible and preserving the knee as the basic principle decreases mortality and positively affects the prognosis and function of the prosthesis.8-10 TTA is the best amputation in terms of functional outcome and energy requirement.10-12 The major disadvantage of Burgess' long posterior flap technique relates to the objective intraoperative evaluation of muscle viability (color, contractility and capillary bleeding). Therefore revision surgeries due to wound healing problems and secondary muscle necrosis are not uncommon.19-21 We performed stump revision surgeries due to necrosis at the incision site and necrosis of the muscles in the anterior and lateral compartment in 11.5% of the cases and knee disarticulation in 5.7% of cases that were amputated by the Burgess technique.
Complications of the Burgess technique led Lutz Brückner to perform physiologic studies on muscles of cruris in the 1980s and he classified the muscles of this region as tonic muscles (with slow contracting fibrils, i.e., soleus and gastrocnemius) and phasic muscles (with fast contracting fibrils, i.e., tibialis anterior and peroneal muscles).25 He claimed phasic muscles were vulnerable to ischemia as the cause of secondary muscle necrosis and thus recommended excision of all muscles of the anterior and lateral compartment. He has also excised fibula to fill the defect, to prevent abduction deformity of fibula8,24 and closed the stump with complete medial part of gastrocnemius and a part of lateral gastrocnemius. But in this type of amputation where anterior and lateral compartment is completely removed together with fibula and a short stump is left, Jones reported poor adaptation to prosthesis and skin ulcerations on the lateral-distal part of the stump.26 In the cases of modified Burgess technique where we have removed the tibialis anterior muscle, we have observed recurrent skin macerations in 14.5% of the cases due to decreased soft tissue mass between tibia and fibula. This problem occurred in 9.6% of the cases amputated by the Burgess technique.
In their individual studies Bruckner and McCollum have determined tibialis anterior as the most vulnerable muscle to ischemia.22,23 Other studies showed that soleus muscle has a large venous plexus and if posterior flap of stump is rotated to anterior, relative stasis is formed within the plexus that leads to thrombus formation and subsequent necrosis.24 In the modified Burgess technique, we removed these two muscles carrying high risk of necrosis, but preserved the muscles of the lateral compartment and the fibula. Only 3.6% of the cases amputated by this technique required revision surgery whereas this number was as high as 17.2% in the Burgess technique. Our results showed a 1.8% increase in revision surgery due to the remaining peroneal muscles compared to the Brückner technique, but problems of adaptation to prosthesis in the Brückner technique described by Jones were not observed.
Studies have shown show that TTA provides better results and has superior prognosis than transfemoral amputations, thus amputations as distal as possible should be preferred.9-12 We have performed the shortening of stumps in four cases and knee disarticulation in three cases in the Burgess group due to muscle necrosis. Complications that developed in two cases of the modified Burgess technique were addressed by only soft tissue procedures. Good functional results were obtained in 82.6% of the cases of the Burgess technique, but in 92.7% of the cases of the modified Burgess group.
In the cases of the Burgess technique, repeated revision surgeries due to problems at the incision site of the stump and muscle necrosis has increased the length of hospital stay, delayed the rehabilitation, impaired the functionality of the prosthesis due to shortened stump and deteriorated the psychological status of the patients. Using the Burgess technique, 82.6% of the cases have returned to daily activities with good functional outcomes without crutches in an average of 162.5 days; and using the modified Burgess technique, 92.7% of the cases have returned to daily activities in an average of 101.5 days. In our study, we observed that 17 cases received antidepressants, had delayed rehabilitation and poor adaptation to prosthesis.
Our retrospective study has shown that the modified Burgess technique is an alternative method that can be preferred for TTAs in chronic arterial occlusions because of less need for revisions, quick adaptation to prosthesis and better functional outcome when compared to the Burgess technique. In the light of the literature, the technique also seems to be superior to the Brückner technique, with reduced adaptation problems to the prosthesis and few skin macerations.