
Abstract
Aim: The phantom phenomenon is a well-known example of the difference between body awareness and body schema. The present study is aimed at showing how body changes and prosthesis use are reflected in body schema and body awareness–the latter relating to the image that various amputees have of their bodies.
Subject and methods: (i) Examining the configuration of body schema: A trial examining the spatial location of the phantom limb (50 people with lower or upper limb loss); (ii) examining the functional aspect of body schema: The distribution of weight power between intact and prosthetic limbs (34 people with tibial amputation); (iii) examining body awareness: Body Focus Questionnaire by Fisher (44 people with lower limb amputation, 33 intact people); and (iv) Questionnaire on anamnesis- and prosthesis-wearing habits (people participating in research methods [i] and [iii] mentioned above).
Results: We found that when the amputees wore their prostheses, the configuration of body schema did not change, however, the people who had not used their prosthesis for a long period of time (in our study, at least for six years), the phantom limb shortened, a phenomenon known as telescoping. The functional adaptation of the prosthesis to the body schema starts in a short time (within two weeks) after wearing it, and it becomes close to normal in carrying body weight after a longer period of time (two years). In the beginning phase of rehabilitation, the awareness of legs is similar to that of the control group, while later on it this awareness decreases. Over time, however, the lost limb, regardless of having a prosthesis or not, loses its importance. People with a more serious or vascular amputation of the upper limbs have a clearer image of them. Limb parts having a greater cortical representation appear more intensively in phantom sensations, while the strength of the cortical representation in body schema has no significance.
Conclusion: From both configuration and functional aspects, wearing a prosthesis helps maintain a body schema in which the phantom limb remains similar to the intact one, which can be explained by the connectional schema model. This is needed for movements to be carried out properly. Although the amputee can see the prosthesis and senses the phantom limb, they do not consider it their own since they are aware of the loss. Therefore, the fact that a prosthesis is worn will not be represented in body awareness as the highest level of mental structure.
Introduction
The loss of a limb results not only in morphological changes, but leads to changes in peripherical proprioceptive and visual stimuli as well. Changes to these stimuli will consequently alter the processes of motional control of the central nervous system at different levels. Patients are aware of the fact that their limbs have been lost; however, they will sense them as if they were not lost (Knecht et al. 1998; Davis 1993). In this study we have launched an enterprise to find out how body change and prosthesis use affect body awareness and body schema.
Fisher (1986) defines body image as ‘the image of our own body. It refers to the body as a psychological experience which includes our emotions and attitudes, developed through our experience, toward our own body’: Kudar wrote, Schilder (1935) sees body awareness as a subjective experience of bodiness; the complexity of the principles of body schema, body posture, and body position in relation to spatial motions (Kudar 1994).
Kudar (1994) argues that body awareness is the conceptualization of body image–its conceptual realization, which is based on the experience coming from our body and on the evaluation of the information received from different sources.
Lakatos (2000) says that according to Vayer and Destrooper, body awareness can be considered as the basis of personality; the individual arranges his/her behaviour and activities (consciously and unconsciously) by building on it. Fisher conducted several surveys on body awareness, which Kudar (1977, 1988, 1994) presented in his studies. Fisher's findings show that individuals focus disproportionately more on specific body areas than on others, and this is a characteristic feature of personality. In his Body Focus Questionnaire, he examined the awareness and clearness levels of images of different body parts. He found that there is a difference between men's and women's awareness levels of body parts. For men, body awareness has more permanence. He found a relationship between dexterity or left-handedness and body awareness. Left-handed participants were more certain in perceiving their body senses, while right-handed ones showed less body divergence. Higher scores were assigned to the Head, Stomach, and Eyes Scales of right-handed women, and Legs, Heart, Arms, and Stomach Scales of right-handed men (Fisher et al. 1984). When examining patients with Raynaud Syndrome, it was found that there was a positive relationship between vasomotor activity and the Arms Scale (Surwit et al. 1978).
Kudar (1994) studied the structure of body awareness (in Fisher's reading) by comparing 300 intact right-handed sportsmen with 60 people not involved in sports. The primary goal of his research was to obtain information on the effect of performing demanding bodily activities (physical exercises, learning motions, body harms) on body awareness. In his analysis (relying on Fisher's theory on oriented body image) he also examined how body areas of different awareness levels can be interpreted as body awareness signs of different attitudes and characteristics, beyond what they reveal about themselves.
As a main component of his analysis, he found that the factoral structure of body awareness is rather stable. He compared earlier samples of American (Fisher et al. 1984) and French (Bruchon-Schwitzer 1979) males and found significant cultural differences. In comparing American and Hungarian samples the latter's scores for the Right Side and Heart Scales were higher; those of the Back, Head, and Stomach Scales were lower, while the Eye scale had similar scores. Accordingly, Hungarian men focus more on their heart and the right side of the body and less on the back of the body, the head, and the stomach. The body awareness of French males is similar. He explains these findings with the influential effect of different socio-cultural and psycho-cultural factors concerning body awareness. In comparing the data of sportsmen who had undergone amputation within one year, he found that the injury appears in the body image and is reflected in the Right/Left Side Scale and the factorial structure of body awareness. As he explains, the injured body part becomes a point of reference because of the effect of the injury, which hinders the execution of motions, and the motions are adjusted to the environment with respect to this. In comparing sportsmen involved in weightlifting, judo, and canoeing, he found a higher level of image sharpness of arms, which can be explained by their specific functional role in these sports. Also, he found a connection between the awareness level of different body areas and some personal characteristics.
Murray and Fox (2002) analyzed the body image of amputees and their relation to the prosthesis, using the Amputee Body Image Scale and the Trinity Amputation and Prosthesis Experience Scales, and found a highly negative correlation between body image disorder and prosthesis satisfaction. Fisher and Hanspal (1998) found a significantly negative correlation between body image disorder and mobility with the help of Body Image Questionnaire and Harold Wood Stanmore Mobility Scale. Wetterhahn et al. (2002) also found a positive correlation between physical activity and body image. Amputees who perform regular physical activities have a more intact body image.
Paillard (1999) also distinguishes between body image and body schema. He believes that body schema does not ascend to the level of consciousness; it is mainly needed for the spatial design of motions. Body schema is a central representation of spatial characteristics of the body, which include the length of body segments, their hierarchical structure and configuration, and the form of body surfaces. Body image is the conscious visual representation of how we see our bodies from outside and is not closely related to motion control. Haggard and Wolpert (2005) acknowledge seven main characteristics of body schema: Spatially coded, modular, adaptable, supramodular, coherent, interpersonal, and its role in the actualization of motions. Body schema represents the position and configuration of the body as an expansive material in space. Its main function is to integrate tactile information coming from body areas and proprioceptive information about the limbs into an amodal code. This integration is the basis of the ability to localize a stimulus spatially on the body. Body schema adapts to gradual changes in the spatial characteristics of the body, which can be slow (ageing) or fast (changes caused by fitting objects onto the body). The change caused by tool use is indicated by the change in the function of cerebral neurons and in its relational system (Iriki et al. 1996).
Modular neuron systems provide a representation of different body parts and their relation to each other. Head (1924) thinks that every perceivable change works its way into consciousness by relating to something that happened before (in Kudar 1994). Through a constant change of position, we continuously build up our postural model, which changes all the time. Every new motional position is fixed in this plastic ‘schema’, and the activity of the celebral cortex relates to every latest cluster of senses, aroused by every altered position to it (Kudar 1994). There is a sudden realization of the position when this relating process is complete. Modern psychology, surpassing the earlier models, but following Head's findings, imagines and explains sensation in a connectional, i.e., a network model. The expression ‘emergent schema’ is used for the explanation of schemes, i.e., it considers spontaneous, self-organizing development important. In this theory, there are no previously stored schemas, but a schema is created from emergent characteristics of a network consisting of simpler units in the moment when they are necessary. A pattern which forms a schema is flexible and changes according to context, keeping the micro-characteristics specific to the schema. The structure of a schema is determined by the global representational system (Szokolszky 1998). Kudar (1994) thinks that experts doing research on the matter explain the schema formation of objects in the course of perception, and make its understanding more plastic, but the time will come when the theory of spontaneous self-organization turns to the perception of our own body. The connectional theory gives us an outstanding chance to understand body schema phenomena more precisely in the course of reorganization and the emergence of changing experiences.
A good example of the difference between body awareness and body schema is the phantom phenomenon, in which the individual feels his/her lost limb as real despite being aware that it had been amputated (Kudar 1994). Haggard and Wolpert (2005) create groups of body schema disorders according to functional deficiencies. Phantom phenomenon belongs to body size disorders.
Research on phantom phenomenon as a body schema disorder
Body schema research has not been able to do without examining phantom phenomenon; several theories have been created to explain its origin. Some have argued for its peripherical origin, while others believe in its central roots.
Upon amputation, the peripherical nerves, on which neurofibromas can appear, are injured. They can also transmit information. The treatment ‘TENS’ (Transcutaneous Electrical Nerve Stimulation) of these nerves can reduce phantom pain (Malin and Winkelmüller 1985).
To prove the peripherical origin of phantom phenomenon, it was claimed that the phenomenon does not occur in children born with limb loss. This hypothesis has been proven false, however, because some patients have reported to have had the sensation of a phantom limb since then. The sensation of phantom limbs for children with congenital limb loss was examined: 42% of the children reported phantom sensation, and 29% of them had phantom pain (Wilkins et al. 1998).
The central origin theory is supported by an early experiment by Hindenmayer. He got people with limb loss to do similar tasks with their intact side as well as their side with limb loss. He examined the results with EEG. The EEG registered the same changes on both sides (Hindenmayer 1962).
Liaw et al. (1998) examined phantom phenomenon with photon emission tomograph. The examinations were made during phantom activity. A change in the cerebral circulation was recorded, but there was no significant difference between the left and the right side. In their opinion, phantom pain is connected to the frontal, temporal, and parietal cortex, and a polysynaptic track might exist there which transmits phantom perception to the cortex.
The rearrangement of the somatosensory cortex was observed with traumatic arm-amputees. The representation of the lower limbs shifted to the region of the hand (Knecht et al. 1998). Phantom phenomenon has also been observed in psychiatric and/or neuropathological and cerebral-operated patients, and not only amputees, which provides evidence of its central origin and components (Souques and Poisot 1905; Malin and Winkelmüller 1985; Grossi et al. 2002). Melzack's neuromatrix theory has recently become the most widely-accepted one, holding that phantom phenomenon has a supraspinal origin (Ramachandran and Hirstein 1998).
The role of stimuli of different modality
Researchers debate whether visual or proprioceptive stimuli play a greater role in the arrangement of body schema. Ramachandran and Hirstein (1998) claim that visual feedback has an important role in perceiving phantom limbs. A ‘virtual reality box’ was created for patients lacking phantom phenomenon. The mirror within the box reflected the motions of the intact limb as an illusion of the lost limb. Patients reported the motional perception of the lost limb. This perception did not occur without the mirror (Ramachandran and Hirstein 1998).
Poeck and Ograss (1934) did not find a big difference in the results of exercises with body schema on sane, blind, and seeing children. This fact implies that proprioceptive information plays a rather important role in the arrangement of body schema.
Hunter et al. (2003) examined which sensory stimuli play a role in phantom phenomenon. He concluded that visual, tactile, and sensomotoric stimuli all play a role simultaneously, but the most intensive phantom sensations were created by visual stimuli, the illusion of which was made by the mirror.
Andre et al. (2001a) questioned people with acquired and congenital limb loss about their spontaneous perception, the existence of the missing limb, its posture, motions, and memories. His research revealed that the representation of the phantom limb depends on the individual's perception and is the result of both congenital characteristics and peripheral information. In another study (Andre et al. 2001b), he analysed the connection between the vestibular system and body schema. Vestibular stimulation caused a temporary perception of the phantom limb in 16 of the 17 cases of amputees who had not had a phantom sensation. Twelve patients having a painful or deformed phantom limb felt a normal phantom sensation from the stimulation. The findings indicate that vestibular stimuli play a rather important role in building a body schema. He suggests a complex neuromatrix theory to explain phantom phenomenon.
Pucher et al. (1999) agree about the connection between body image, phantom pain, and limb loss and advance this theory. Few participants who were actually successful in adjusting to limb loss, less suffered from phantom pain. At the same time, the people who suffered more from phantom pain perceived their bodies as a coherent whole.
Proprioceptive mechanisms can be improved. Amputated and intact limbs were slowly and passively moved in people with an amputation above the knee. The amputee's ability to reproduce different limb positions was examined. There was a significant difference between the two kinds of limbs. The number of mistakes was proportional to the time that had elapsed since the amputation, meaning that amputees had improved the rest of their skills, i.e., the lack of knee articulation structures was compensated by improving sciatic articulation proprioception (Eakin et al. 1992).
The expected success of rehabilitation depends on several factors. Kullmann et al. (1991) examined the results of 394 amputees after one and a half years, on average, following amputation. Two thirds of the participants had a vascular disease. Less than half of the people of an advanced age or with a vascular disease left their home. A wheelchair was used only by those with a vascular disease or with several lost limbs. In his review, Cutson and Bongiorni (1996) summarizes that age itself is not a dominant factor, but accompanying diseases and general conditions are. In the case of older patients suffering from vascular diseases, the aim of rehabilitation is short-term walking and cosmetic replacement. Hermodsson et al. (1994) found a difference between patients suffering from vascular disease and tibial amputation following an accident; the standing balance of patients with a vascular disease was worse than that of amputees after an accident.
Quite a few authors deal with the change of body schema and phantom phenomenon; the topic has been approached from several aspects. The manifestations of phantom phenomenon are well known. The effects of both peripherical and central processes must be accepted as an explanation for their appearance. The stimuli of different modality (visual and proprioceptive) have an effect on the phenomenon simultaneously. However, the effect these two kinds of stimuli have on the rearrangement of body schema through prosthesis use has not been examined. Following the amputation, body schema, body image and the satisfaction with them have been mostly researched. What has not been studied, however, are the effects of limb loss on body awareness.
This study is aimed at presenting how body change and prosthesis use are reflected in body schema and body awareness, the latter in amputees' self-image about their different body areas in proportion to time elapsed since amputation? Our research hypothesis is listed as follows:
It is assumed prosthesis use helps maintain a configuration similar to the normal one; i.e., patients sense their bodies as a configuration before the amputation. At the same time, amputees who have not been wearing a prosthesis will experience a shortened phantom limb. Wearing a prosthetic limb (it is a kind of tool use, though), which will be sensed as one's own body part through time, shows the functional aspect of body schema. Since the structure of body awareness is rather stable (Kudar 1994), it is assumed that this structure, following limb loss, will change after a longer period of time (at least six months), and the change will be reflected only in the body part in question, i.e., the Legs Scale; the awareness level of other body areas does not change. It is also assumed that wearing a prosthesis–which will be continuously evaluated through body awareness including the combination of visual and somatosensory stimuli–does not have an effect on the awareness level of missing body parts as the highest central level structure, i.e., the awareness of the lost body area following the amputation will decrease in patients wearing and not wearing a prosthesis alike. In the case of double tibial amputation, it is assumed that prosthesis use does not influence the image sharpness of lower limbs parts, i.e., the supporting surface of the knee, since the tibial prosthesis does not mean lead to a sharper image of the rest of the lower legs. The circumstances surrounding the amputation determine the aim of rehabilitation. A lower level of activity can be expected from the elderly who suffer from vascular disease. It is also assumed that the Arm Awareness of amputees with vascular disease is lower. It is also assumed that, according to the function principle, the arm awareness of people suffering from a more serious body deficiency–double tibial loss–is higher.
Methods
Subjects
In the research on the configuration of body schema
51 limb amputees took part; 33 of them had lost one, two, or three of their limbs due to vascular disease, 18 of them lost limbs in accidents. The average age was 58.4 ± 15.3 years. There was forearm, upper arm, tibial, femoral amputations, or hip disarticulation. Time elapsed since the operation: 1 week to 60 years, average: 87.0 ± 162.0 months. Two patients never wore a prosthesis, 19 were beginners in wearing a prosthesis, 23 were experienced in wearing a prosthesis, and seven patients did not wear one, although they had learned to use it (Table I).
Data of participants in the research on body awareness and on the configuration of body schema
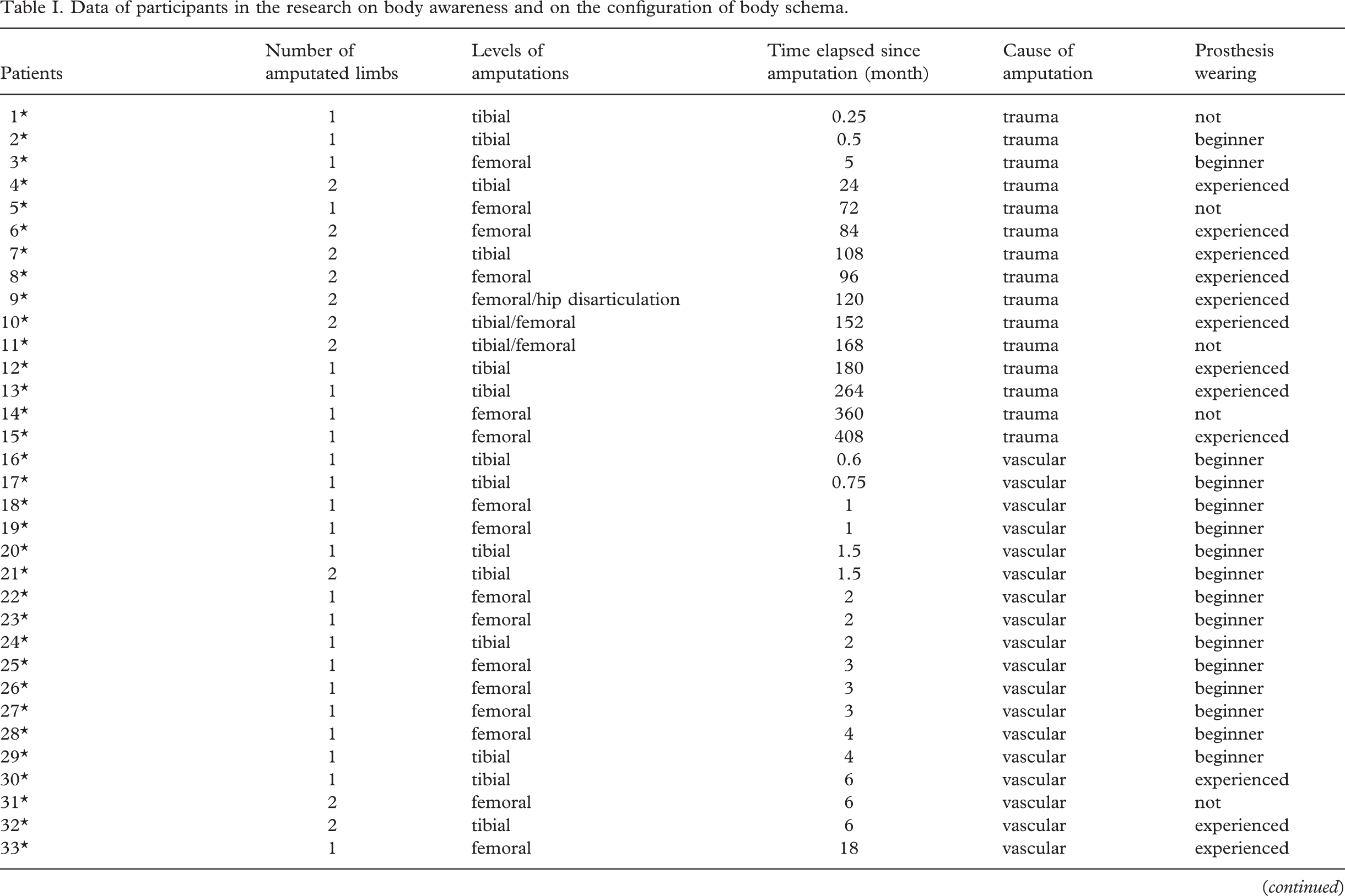
∗Participants in the research on body awareness; #Participants in the research on the configuration of body schema.
In the research on the functional aspect of body schema
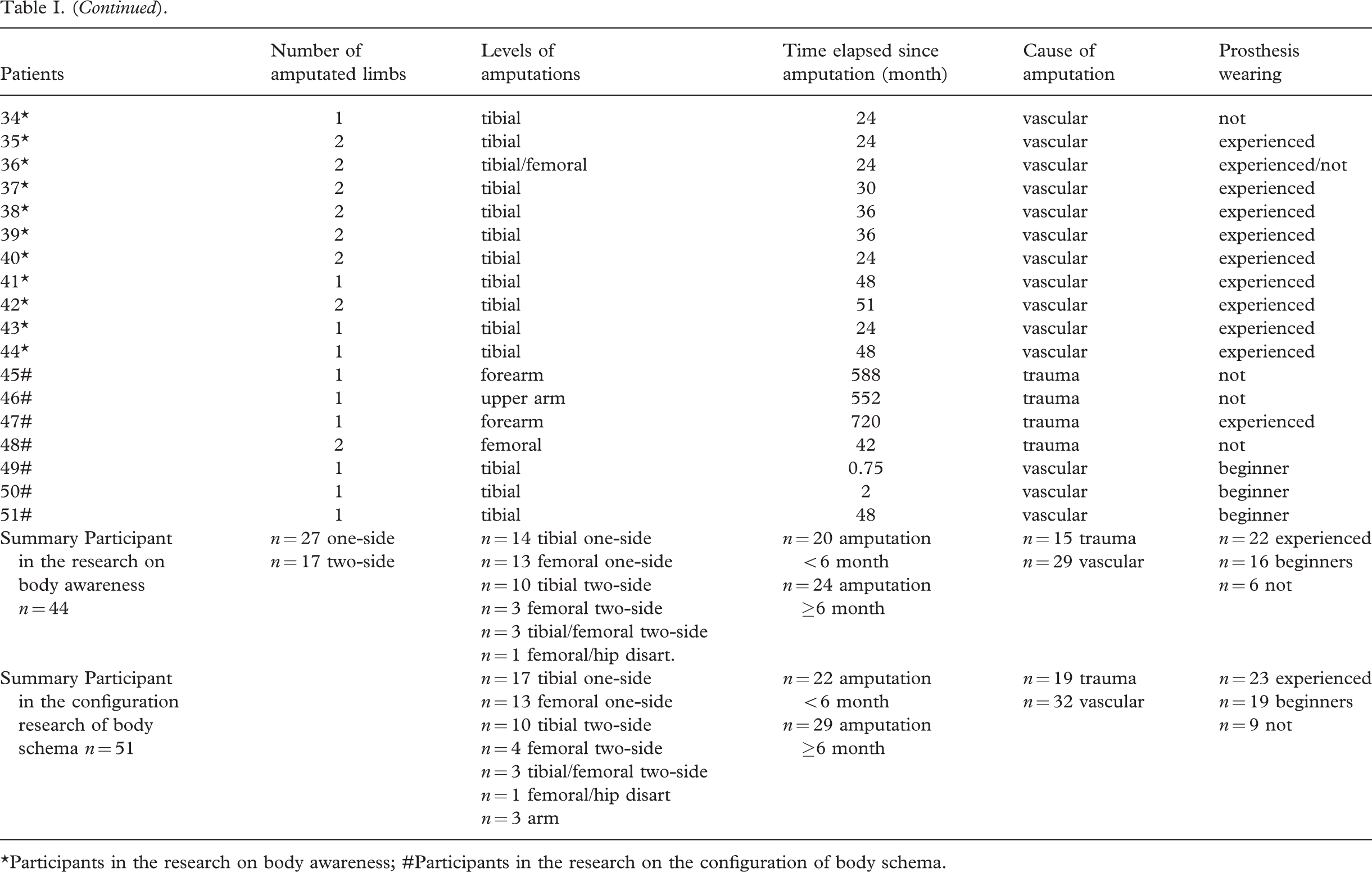
34 patients with vascular disease who had undergone tibial amputation participated. Their average age was 60.0 8 ± 8.85 years. We formed three (in fact four) groups of participants. Eighteen patients had had an amputation five weeks before on average, and they started to practice walking between 2–4 days before the first examination (Group 1). Six patients were checked before and after the two-week walking training (Group 1/a). Ten had had an amputation on one side (Group 2) and six had lost their limbs on both sides (Group 3). Amputees in groups 2 and 3 had lost their limbs 3.6 and 3.3 years before on average, respectively, and were experienced prosthesis wearers (Table II).
Data of participants in the research on the functional aspect of body schema
The research on body awareness
There were 44 male participants who had lost one or both of their lower limbs. The average age of the patients was 56.6 ± 15.3 years, and 22 of them were experienced prosthesis users, 16 were beginning prosthesis users, and six of them had never been worn a prosthesis (one of them had just been operated on). A total of 29 patients had lost their limbs due to vascular disease, and 15 had been due to accidents. Some 27 of the amputations had been on one-side only, 17 had been two-sided amputations. The control group included 33 intact men with an average age of 51.7 ± 14.9 years. One week to 34 years had elapsed since the operation. We created two groups based on time elapsed since amputation, taking into account prosthetization and rehabilitation processes. Group A included patients with an operation less than 6 months before, and Group B consisted of patients having been operated on over 6 months before (Table I).
Every question about anamnesis and prosthesis wearing habits was answered in the questionnaire by all the members of both groups.
Protocol
Research on the configuration aspect of body schema: An experiment to examine the spatial posture of the phantom limb
Lakatos (2000) used a well-known body schema experiment to self-diagnose directional skills of children with a neurological injury. He asked the children to show six different body parts of their own with their right and then left index finger with closed eyes, i.e., without the chance for visual stimuli and control. From the research, he draws conclusions on the maturity of the body image, the exactness and quality of pointing motions, and the ability to discriminate between left and right (Lakatos 2000).
Similarly, we examined the actual manifestation and change of body image through the spatial position of the phantom limb in our research. We asked the patients, seated on chairs with eyes closed, to show where they sense the different parts of the lost limb. Tibial amputees had to show their feet, femoral amputees their knees and feet, forearm amputees their hands, and upper arm amputees their elbows and hands. When the patient felt the body part where the missing limb had been located, we concluded that it was not an example of the ‘telescoping’ phenomenon. We believe this proves that body change is not followed by body schema change, i.e., the extent of the change is not reflected in the body schema yet. We consider the more proximal perception of the body parts in question as an example of shortening, and telescoping, i.e., a change in the body schema. When the examined limb did not shorten and the participant was not able to locate the limb, we considered this to be the beginning of body schema change.
Research on the functional aspect of body schema: The distribution of the body's weight load between the intact limb and the prosthetic one
We applied two force platforms for estimation the weight distribution between the two legs. In the first measurement patients were weighed on one of the force platforms standing in small straddle position. They maintained this position for 26 seconds on a force platform. In the second measurement the force platforms were placed 2 cm from each other and the patients were asked to stand in the same position as before, placing their prosthetic limb (double amputees putting their right limb) on one of the force plates, and the other or intact limb on the other plate. The weight load on the force platforms, i.e., the body weight load of the prosthesis, was measured for 26 sec, at a sampling frequency of 16 Hz. The body weight estimated at the two measurements was averaged. In the evaluation, the weight load difference between the two lower limbs was measured as a percentage of total body weight, so that the distribution of the body weight of double-sided amputees would be comparable to that of the other groups.
Body awareness
Reviewing the Questionnaire, Kudar (1986, 1994) says the BFQ material was compiled by Fisher based on literal and clinical experiments to examine experiences in connection with the body. His original aim was to map out how people focus on different body areas. His findings showed that the participants focused disproportionately on certain body areas, while other areas were considered less important. While filling in the questionnaire, the participants had to choose the limb they could envision more clearly from a pair of limbs. The original version of the questionnaire contained 108 questions, eight of which related to the body, i.e., eight scales: Arms, Front/Back Side, Right/Left Side, Head, Eyes, Mouth, Stomach, and Heart Scale. The Hungarian version of the questionnaire (Kudar 1986) uses an additional ninth scale: Legs, but without any changes or alternations. In Fisher's original idea, different psychical awareness contents and attitudes are associated with different body areas. To conceal the research focus on body and different body part experiences, questions related to body parts were placed randomly in the questionnaire. The Leg Scale was divided into four subscales: Thigh, knee, shank, ankle/foot. That is, we pointed out the four connecting items from the Leg Scale without changing the original scale.
The author believes that this method involves a compromise between the two aspects. One of them is that interpretable samples are needed about some subjective aspects of body experiences. The other is that this information should be easily interpretable in a quantitative way. The preliminary, earlier studies showed that it is extremely difficult to code the spontaneous, qualitative statements expressing the experiences of the participants in connection with their bodies and to use it to determine how they distribute their focus among the different body parts. The BFQ method makes it possible to formulate the sensations in connection with the body by focusing on narrow, easily comprehensible areas. The results relating to the different body parts are simply numbers that indicates how much clearer and more imaginable the opposite limb is considered to be. During the evaluation (apart from the raw points), we attempted to make the results suggestive of the number of possible answers about the different body parts. We used percentages based on the number of answers given by the participants so that parts of the lower limb could be comparable.
Questionnaire on anamnesis and prosthesis wearing habits
We developed a questionnaire which the patients completed. The questions in the questionnaire were related to anamnesis (age, sex, cause, and date of amputation), prosthesis wearing habits, and the localization and characteristics of phantom sensations and their cause.
Statistical analysis
Mean and standard deviation ( ± SD) was calculated for each parameter. Non-parametric statistical calculations were applied using the Mann-Witney U-test and the Spearman correlation of Statistica program package. Significant differences were accepted at p <0.05.
Results
A total of 47 of 51 patients (92%) reported phantom sensations. Most of the patients who had had an amputation could not remember clearly when the first phantom sensations occurred. Seventeen of 22 newly-amputated patients (77%) sensed the existence of a lost limb immediately after waking up. In two cases, this sensation arose two weeks after amputation. A patient injured in World War II also reported intense sensations of phantom phenomenon.
The two patients who had not been wearing a prosthesis because of the short time that had elapsed since amputation and the 16 patients who were beginning prosthesis wearers did not report telescoping; the four beginning prosthesis wearers were inaccurate in indicating the body areas in question and could locate them only with a deviating axis. In every case, the latest, major amputation was preceded by an earlier series of vascular operations and toe amputations.
Telescoping was not experienced in traumatic patients who had had an amputation six months before and had not been wearing a prosthesis. A war veteran with a forearm amputation who had been regularly wearing his prosthesis for 60 years also did not have telescoping. In earlier cases, when the patients had not been wearing a prosthesis (n = 6), shortening was reported (time having elapsed since amputation: 7–55 years). Patients with a femoral amputation had a shortened shank and thigh sensation, with a forearm amputation a shortened forearm sensation, and with an upper arm amputation a shortened forearm and upper arm sensation. At the same time, the sensation of the ankle/foot, hand, palm and elbow remained.
Every lower limb amputee having phantom phenomenon (n = 43) reported sensation in the ankle, foot, toes, sole, and heel areas. Moreover, those patients who also indicated tibial sensation had had problems with their tibial area before the operation. Upper arm amputees reported (n = 4) palm and hand sensation.
We can identify several precipitating factors of phantom phenomenon (without a prosthesis) including tiredness, weather changes, and dreaming or having a rest, though most patients cannot determine the exact cause. There were no reports of phantom sensation while walking with the prosthesis.
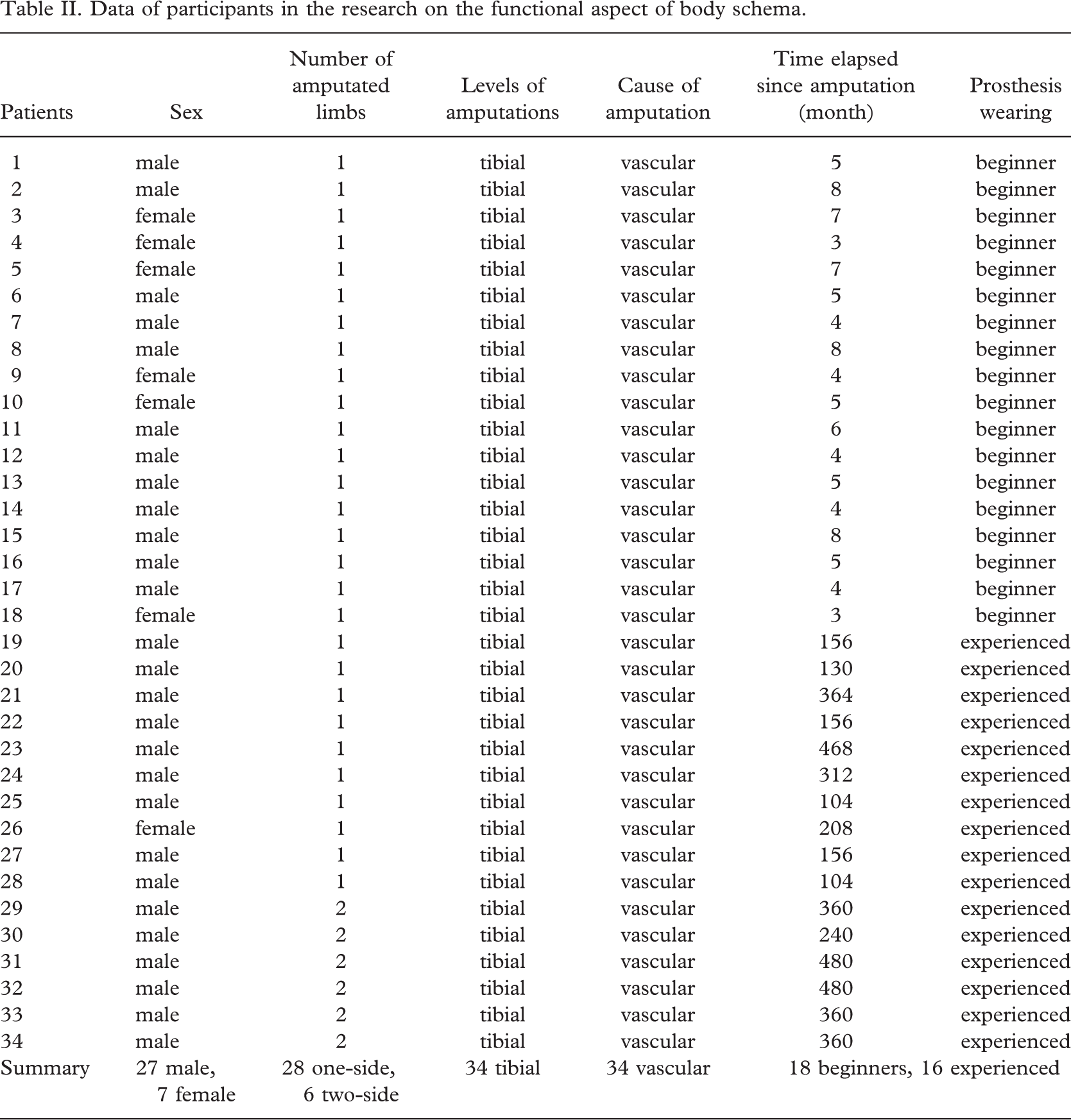
Upon examining body weight distribution, we found that in patients having had a single limb amputation a short time before (Group 1/a), the difference in body weight distribution between the two lower limbs significantly improved following walking training (Figure 1). It was also learned, however, that while there was a difference between the weight load of the two limbs in patients having a single limb loss for a short time (in Group 1: 27.78 ± 15.89%), the patients, independent of whether they had a single or double limb loss (in Group 2 and 3: 6.4 ± 6.72 and 7.67 ± 5.99) for whom a longer time had elapsed since the amputation (an average of 3.6 and 3.3 years), distributed their body weight power almost evenly between the two limbs (Table III) (Figure 2).
The difference of distribution of weight load of the body between legs in terms of % (Mean±SD)
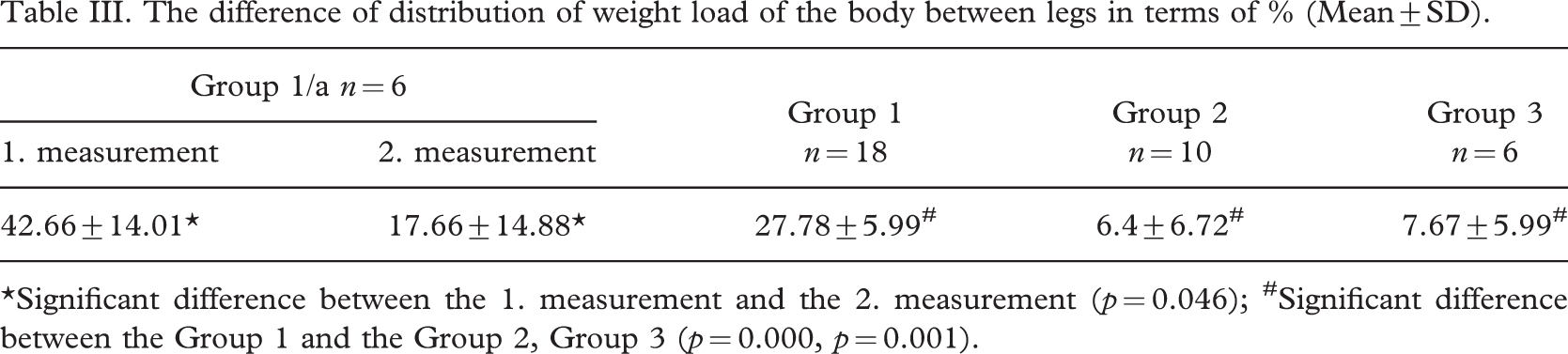
∗Significant difference between the 1. measurement and the 2. measurement (p = 0.046); #Significant difference between the Group 1 and the Group 2, Group 3 (p = 0.000, p = 0.001).
The 44 amputees showed extremely different awareness levels of their legs (lost 1 week to 34 years before). The number of answers to the Leg Scale was between 0 and 18. One patient, having been amputated with vascular stricture, expressed no image sharpness about his leg, which had been lost two years before. Presumably, his leg awareness disappeared from body awareness, and he might have had a strong suppression to exclude his leg from his consciousness. This latter conclusion, i.e., the mechanism of suppression was drawn from personal discussions (Table IV).
Values of BFQ-scales of all amputees (n = 44), in group of patients (Group A) whose legs had been amputated less than 6 months before (n = 20), in group of patients (Group B) whose legs had been amputated more than 6 months before (n = 24), in group of patients with vascular disease (n = 29), in group of traumatic patients (n = 15), in group of unilateral amputees (n = 27), in group of bilateral amputees (n = 17), and in the Control Group (n = 33)
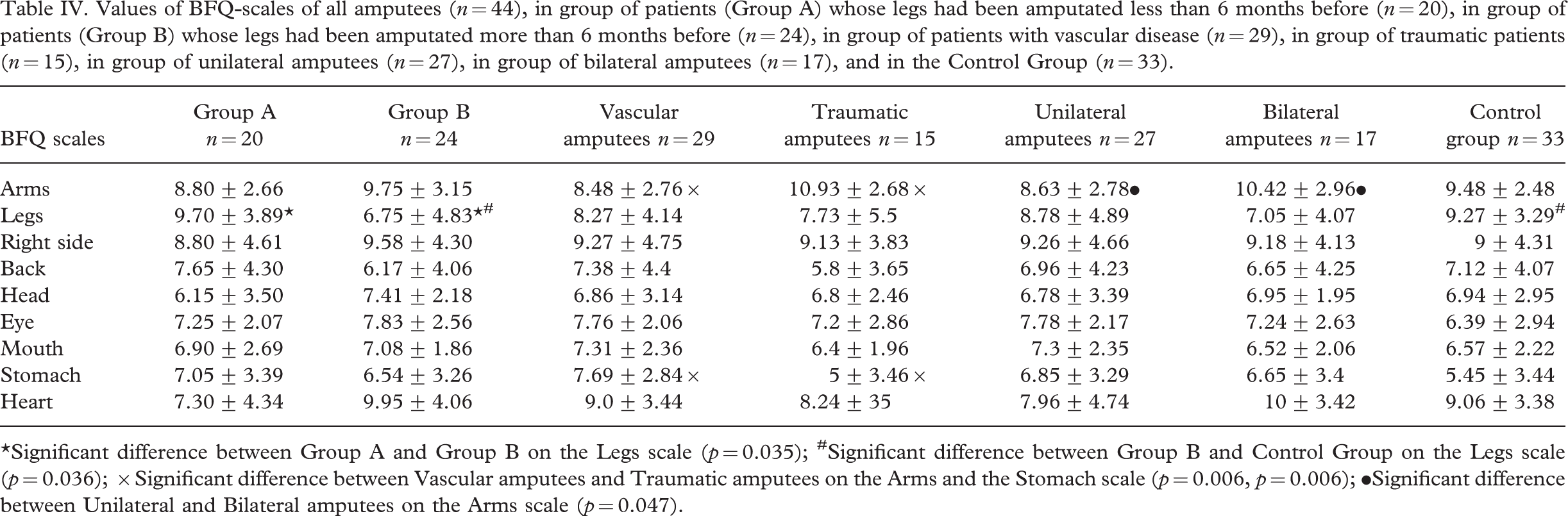
∗Significant difference between Group A and Group B on the Legs scale (p = 0.035); #Significant difference between Group B and Control Group on the Legs scale (p = 0.036); ×Significant difference between Vascular amputees and Traumatic amputees on the Arms and the Stomach scale (p = 0.006, p = 0.006); •Significant difference between Unilateral and Bilateral amputees on the Arms scale (p = 0.047).
In Group A, leg awareness was significantly higher than in Group B (28.14%). The leg awareness of the control group and patients whose legs had been amputated less than six months before did not show a significant difference, while the leg awareness of patients whose legs had been amputated over six months before was significantly lower than that of the control group (25.35%) (Table IV). The other scales indicated no difference. A very weak, but significantly negative correlation was found between the scores of the Legs Scale and the time elapsed since the amputation (r = −0.36).
There was no significant difference between the leg awareness and arm awareness of patients wearing a prosthesis (n = 23), not wearing a prosthesis (n = 6), and beginning prosthesis wearers (n = 15). Therefore, we accepted the hypothesis that wearing a prosthesis does not affect the awareness of the missing body part as the highest level central structure.
The aforementioned hypothesis about patients with a bilateral tibial amputation who wear a prosthesis did not affect their image sharpness of lower limbs parts (e.g., the knee as the supporting area of the tibial prosthesis did not show an increase in these patients' image sharpness), was proved to be right.
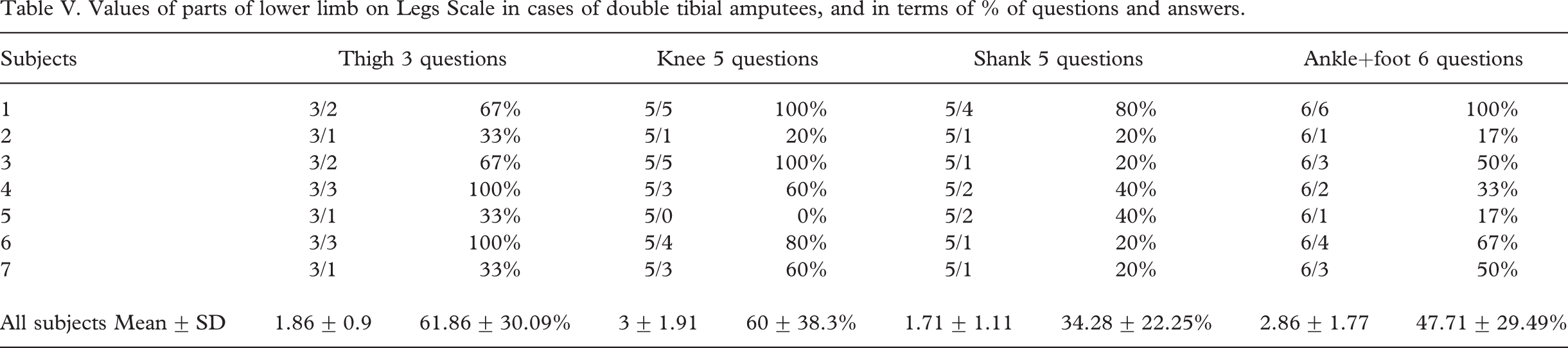
We examined how patients with a bilateral tibial amputation distribute their focus among the different parts of the lower limbs: Thigh, knee, shin, ankle/foot. An answer of 0 was given once for the knee, and the other body parts had a positive result despite the fact that due to amputation, the lower third of the shin and body area ‘ankle/foot’ were missing. It is worth mentioning that the Thigh, Knee, Missing Shin, and Ankle/foot Scales received 60, 61, 36 and 48%, respectively. There is no significant difference between these parts. Thus, we did not find the awareness level of the knee as the support area of the tibial prosthesis different from that of the other body parts, i.e., wearing a prosthesis did not affect leg awareness (Table V).
Values of parts of lower limb on Legs Scale in cases of double tibial amputees, and in terms of % of questions and answers
We can classify the amputees into two groups: Accident patients and those suffering from a vascular disease because the cause of amputation determines the chances and aims of rehabilitation. There was no significant difference between these two groups of amputees and the control group. At the same time, arm awareness level was higher for patients suffering from trauma than amputees with a vascular stricture (22.41%) or the control group (13.27%). Moreover, patients suffering from a vascular disease have a stronger stomach awareness than traumatic amputees (34.98%) or the control group (29.3%). The further BFQ scales did not indicate a difference between the groups (Table IV).
There was a significant difference in patients' Arms image sharpness amongst the single and double amputees and the control group. Patients suffering from a more serious body deficiency, i.e., a double lower limb loss, had higher image sharpness than patients with a single lower limb (17.18%). There was no difference between the amputees and control group in the Arms and Legs Scales (Table IV).
General discussion
The changes in the configuration of body schema were influenced by the time elapsed since amputation and prosthesis use. Both patients who had not worn a prosthesis and beginning prosthesis users were influenced by the fact that the short period of time elapse since amputation does not allow the brain to rearrange the impulses coming from the periphery and create an altered body schema. The beginning of body schema rearrangement was observed in four beginning prosthesis users, all of whom had had an amputation a short time before, were suffering from vascular disease, and who could only complete the phantom spatial location test with a deviating axis. In this case, the alternation of body schema might have started in the period prior to the amputation due to the preceding operations, because the painful body parts were used less and a medical aid was used for walking. Phantom limb shortening and telescoping were only experienced with patients not wearing a prosthesis. When a patient refuses to wear a prosthesis, it can be concluded that a long time period, at least four years, seem to be needed for a significant change to the body schema. The importance of the effect of peripherical information is reflected in the case of a patient with a bilateral lower limb amputation, who regularly wore a prosthesis only on one limb: The phantom limb is of normal size on this side, while the body schema of the side he had worn the phantom limb on randomly changed.
Phantom sensation occurs more intensely on sites with a greater cortical representation (ankle, foot, toes, sole, and heel) (Davis 1993). The sensation of body areas having a distal, greater cortical representation was experienced by each amputee with a phantom phenomenon; the more proximal areas have less importance and are mostly not sensed. Body areas with less representation were found to fall out of structural body schema in patients with telescoping, while body areas with more representation remained.
The difference in the distribution of body weight reflects the functional adaptation level of the prosthesis into body schema. At the beginning of walking training, the asymmetry of the weight load indicated the starting phase of the adaptation process. Although two weeks can be considered a short period of time, the difference between the load of the two limbs had already increased, indicating that there was considerable progress in the adaptation process. The image of a symmetric load emerged after a longer time (at least two years, in our case). The functional adaptation of the prosthesis was completed by the time a symmetric load image was created. At the early stage of walking practice, a special four-leg walking frame was used by patients; they gradually changed to crutches and some even walked without any medical aid. With the increase of the weight load of the prosthesis, a medical aid was less and less necessary.
Regular prosthesis wearers must have two action schemas for walking with or without a prosthesis (in our case the latter was less frequent, but sometimes inevitable). When walking with a prosthesis, no medical aids (or in fewer cases) were needed, however, walking without a prosthesis always required a crutch or a walking frame. In the connectial schema model, walking is performed within a global representational system frame. One of its elements is one's own body sensations. Different types of information are received from the periphery, depending on whether a prosthesis is being worn or not; the activation of the actual necessary smaller networks emerge accordingly. Anderson and Brophy (1984) differentiate strong and weak schemas, which is valid in amputees, too. The presence of the phantom in prosthesis wearers indicates that the strong schema is sensed by the body as a whole, i.e., together with the prosthesis. In patients with an earlier amputation, a strong, complete body schema is created due to regular prosthesis use; while in patients not wearing a prosthesis, the strong schema is the altered body schema involving the shortened phantom limb.
Following the functional adaptation of the prosthetic limb starts during walking practice. In this period, there is a difference between the configuration and the functional side of the body schema: Structurally, the phantom sensation is complete, while the patient is hardly able to use it. However, the adaptation of the prosthetic limb begins very soon; a considerable improvement takes place in the body weight load of the patient within two weeks, and with rehabilitation, patients acquire the highest walking skill attainable after about six months. By this time, the prosthesis is completely adapted to the functional body schema and the structural body schema is complete as well.
In the case of amputees who did not wear a prosthesis, the lack of adaptation to the body schema is followed by a reduction of the structure, but only years after the amputation. However, a total reduction of the structure, i.e., the entire disappearance of the phantom phenomenon, did not occur in our pattern. The close connection between structure and function is emphasized by Simmel (1956) and Price (1976), who in examining patients suffering from leprosy found that the lack of the phantom phenomenon may originate from the deficiency of the sensomotoric functions–because in these cases, the reduction of the function and morphology happened in a similar way. However, our research on the patients finds a sudden disappearance of the function, and then a slow reacquisition in the cases of those who wear a prosthesis. In patients not wearing a prosthesis, the disappearance of the function is followed by the change of structure, while regaining the function helps the structure remain.
The amputees' phantom phenomenon is the manifestation of body schema and its configuration and functional features should be separated. While the configuration one changes slowly, functionally, the prosthesis does not literally fit in the place of the lost limb, i.e., the amputee does not experience the movements of the prosthesis as the ones of the phantom but totally independently of it (i.e., like in a dream). Fitting in (adaptation in) body schema means that the prosthesis, as a new means of changing location and position, infiltrates into the already existing body limits. The ability to use the new prosthesis properly can be acquired by learning how to apply it and the increased proprioception and cortical representation of the stump. In the case of monkeys which underwent an amputation, the change of mental and spinal sensory representation was proved. The representation of body parts proximal to the stump increases and seems a lot more extended than in the case of intact animals (Wu and Kaas 2002).
Despite limb loss, only one of 44 patients did not focus on his/her lower limbs. However, the focus on the legs is highly diverse. But if we consider time passage since amputation, one can see that body awareness has been influenced. At the initial stage, the Arm and Leg Scales did not produce any significant differences in comparison with the control group, which supported Kudar's results that body awareness is a stable organization. After a longer period of time, irrespective of wearing a prosthesis, a lower level of consciousness may be experienced, which results in keeping the phantom in the body schema (in the case of amputees using a prosthesis), while for those who do not wear one its participation in the body schema decreases.
Shortly after amputation, the lower leg is present both in body schema and body awareness. A passage of time needs to occur to identify the difference between them. Further disparity occurs between the different parts of the lower limb in connection with body schema and awareness. In studying the latter, no difference could be shown in the level of focus on the thigh, knee, and shin+ankle fields; nevertheless, no participant had focused on the shin+ankle field after the amputation. It was not even modified by wearing a prosthesis.
Tibial amputees' focus on the knee, in spite of the fact that it is an important area for transmitting sensoric information rather than as a supporting surface, does not differ from the quality of focus on other areas of the lower limb. The structural body schema as an extension was influenced by wearing a prosthesis; the intensity of the sensation of some lower limb areas was determined by the cortical representation of the different areas. Patients with telescoping did not report lower leg sensation, for example, while the ones having a normal phantom sensation indicated the sensation of distal areas rather than that of the shin.
Body awareness is not influenced by the cortical representation of the different areas. Consequently, only body schema is influenced by wearing a prosthesis, while body awareness is not. The latter, as we know, is a rather stable structure and does not change immediately after limb loss, but after a few months; although the amputee can see the prosthesis and sense the phantom limb, they do not consider it as their own since they are aware of its absence. It does not appear in the image sharpness because it is the highest level of mental structure.
No difference has been found between the traumatic and vascular amputees concerning the image sharpness of the Legs, however, the image sharpness of the Arms was higher in traumatic amputees and was similar to those with a double lower limb loss, regardless of the indication. The greater importance of the Arms is explained by their role in physical activities, but it is also mainly due to postural stability. Kudar's (1994) and Fisher's (1986) study shows that the image sharpness of the Stomach is connected to relaxedness, among others. In patients with an amputation due to vascular disease, the higher image sharpness of the Stomach can refer to their constant frustration because they are multimorbid people, and their disease may affect the whole body which had not been cured with an amputation. Loss of the legs causes the decrease of physical power. Kudar (1994) argues that frustration results in a strong image of the legs, and its body awareness sign is connected to the difficulties of realizing power and low risk-taking. Thus, the decrease in the image sharpness of the Legs can be explained by the changes in morphological and psychical features due to the new life situation. In accepting Melzack's theory that the phantom phenomenon has a supraspinal origin, we also have to consider the role of peripheral information too, which may influence prosthesis users' phantom phenomenon sensations?
Conclusion
The results of this study suggest that by wearing a prosthesis, the amputee can maintain their body schema similar to an intact leg, including the phantom limb. At the same time, amputees who have not been wearing a prosthesis will experience a shortened phantom limb, which is explained with the connexial schema model. Although the amputee can see the prosthesis and sense the phantom limb, he/she does not consider it as their own, being aware of its absence. Subsequently, wearing a prosthesis does not appear in body awareness as the highest level of mental structure. The values of Leg scales decrease independently of prosthesis usage. Arm Awareness in people with amputation due to a vascular cause is lower than that in people with greater limb loss like bilateral amputations. When planning rehabilitation, physical exercises aimed at adapting the prosthesis into the body schema must be involved in the program.
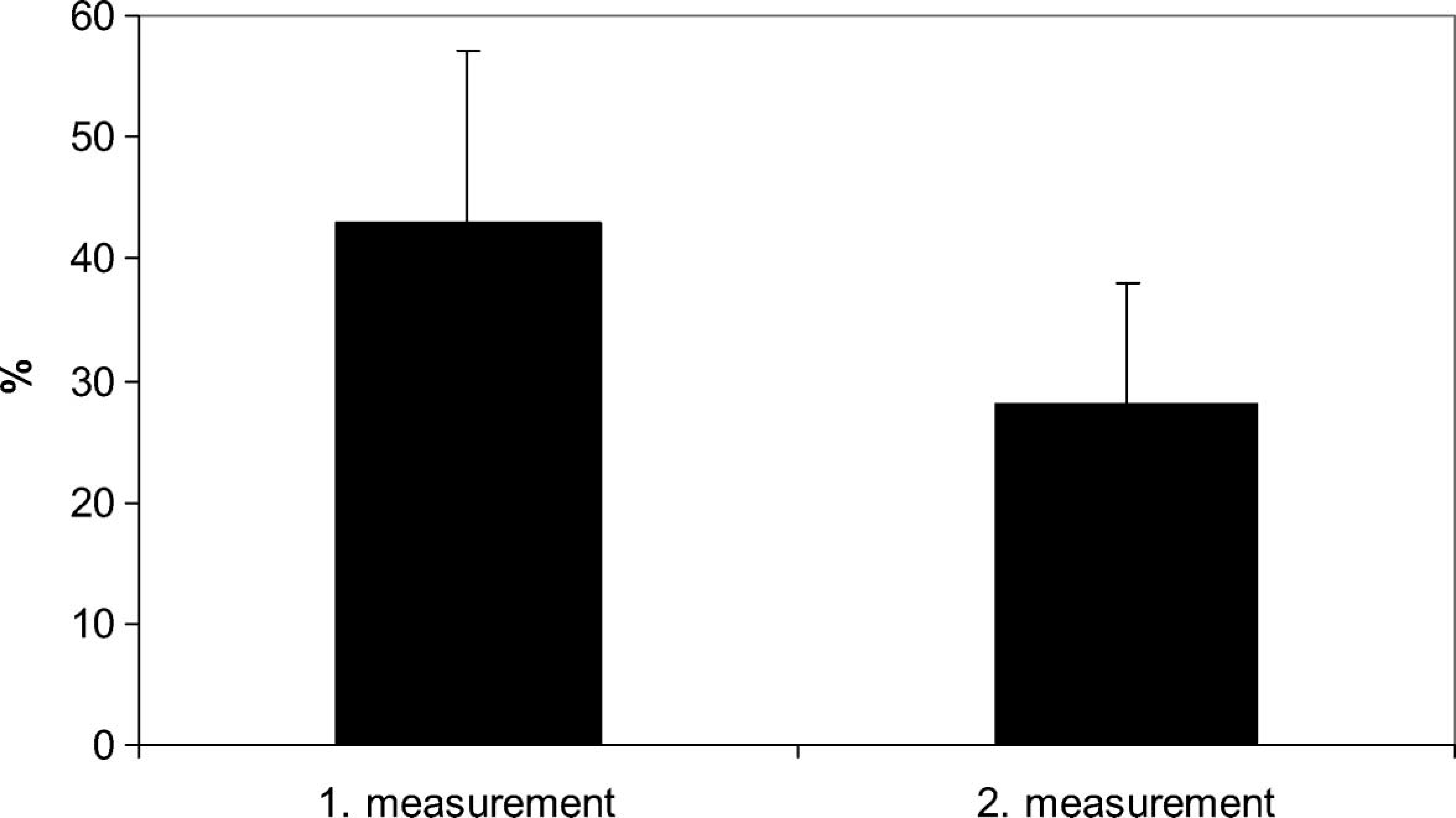
The difference of distribution of body weight load between the two lower limbs in the group of patients having had an amputation a short time before (Group 1/a), with 2 measurements (n = 6).
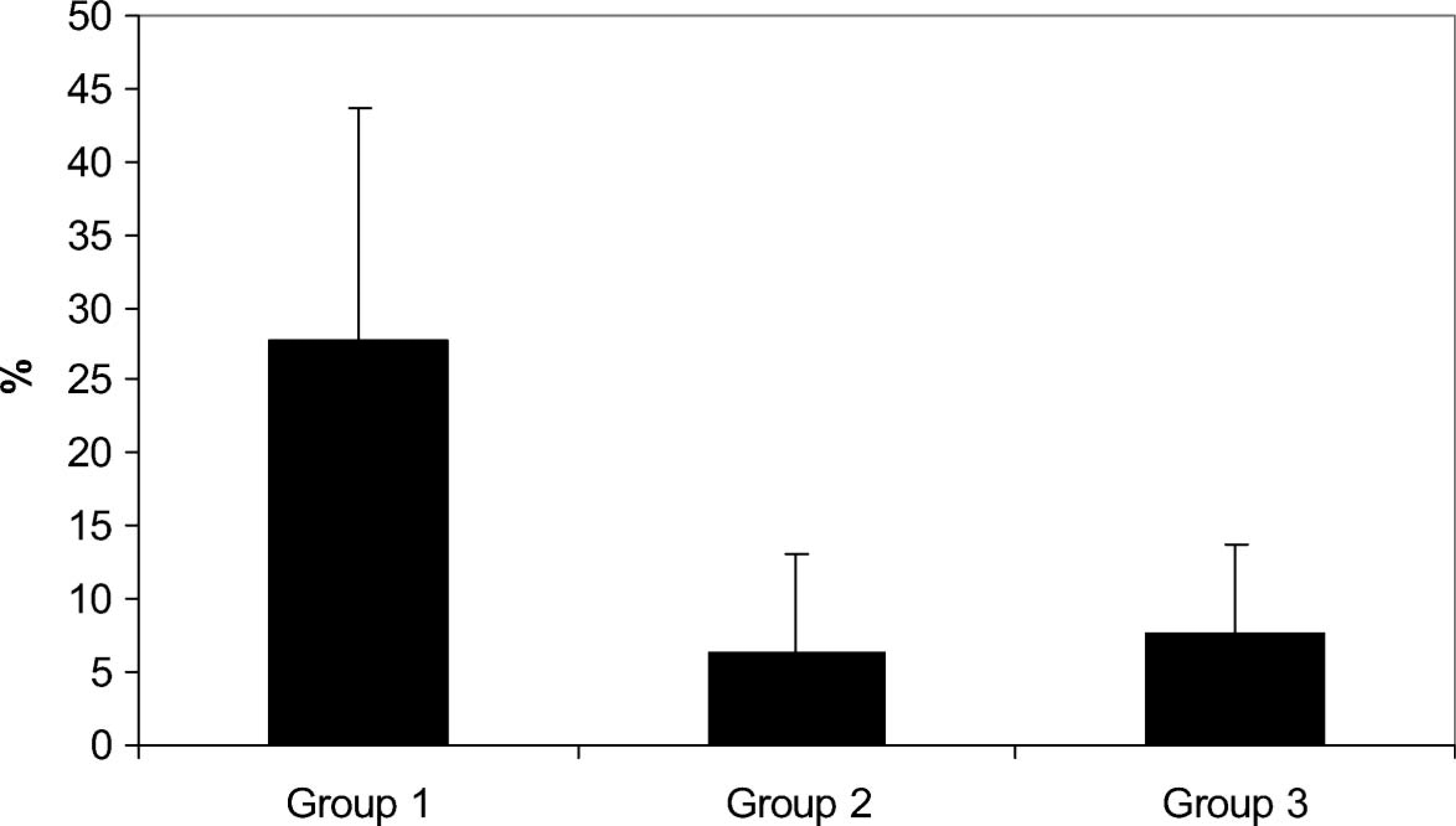
The difference of distribution of body weight load in the groups amputees (Group 1, n = 18; Group 2, n = 10; Group 3, n = 6).