
Abstract
Transfer of Musculus Latissimus dorsi/M. Teres major to the rotator cuff with or without M. Subscapularis/M. Pectoralis release is a widely used procedure for restoring shoulder abduction and external rotation in squeal of obstetric brachial plexus palsy. After the operation a shoulder abduction orthosis in maximal external rotation and 90 – 100° abduction is utilized following six weeks of immobilization in a shoulder spica cast for protecting the newly transferred muscle from undue elongation. However this in turn may cause contracture of the external rotators. To overcome this problem, a modified shoulder abduction splint with adjustable internal-external rotation/abduction-adduction ranges was developed in the orthotics department of a rehabilitation center. The custom molded adjustable shoulder abduction orthosis is described and the preliminary results are compared with former applications.
Introduction
The incidence of obstetrical brachial plexus palsy (OBPP) is as high as four per 1000 births in populations with poor medical facilities and 0.1 – 0.3% where good obstetrical care is available (Narakas 1987). Lesions range from neuropraxia to neurotmesis or root avulsion. Consequently the outcome also ranges from recovering function before the end of the first month in which case the infant presents a normal extremity at 4 – 6 months to a poor pattern of recovery with concomitant sequel and a non-functional extremity.
Although the extent and severity of the deformity varies, the shoulder is the most frequently affected joint and internal rotation contracture causing limitation of abduction and external rotation is common in patients who have not recovered (Demirhan et al. 2002; Waters and Bae 2005).
The treatment algorithm to maximize each child's long-term functional recovery is continuously evolving. Children who fail to attain active abduction and external rotation are candidates for tendon transfers. Most commonly this involves transfer of the Musculus latissimus dorsi and M. teres major to the greater tuberosity insertion of the rotator cuff (Bennett and Allan 1999; Moukoko et al. 2004; Akinci et al. 2005; Waters 2005; Waters and Bae 2005).
Post-operative management
There are essentially four main areas of concentration in the post-operative management of tendon transfers: Immobilization, scar management, muscle re-education, and functional performance. In all tendon transfers, there is an initial period of casting followed by protective splinting with a removable splint. The initial period of cast immobilization usually continues for approximately 3 – 6 weeks (Raimondi et al. 2001; Shenaq et al. 2004). After initial immobilization a removable splint is fabricated for full time use. During this period, the splint may be removed for bathing and therapy. The position of splinting usually replicates the position of casting which is approximately 90° shoulder abduction, 90° external rotation, 90° elbow flexion, neutral forearm rotation with wrist support if necessary. The duration of splint utilization is usually 2 – 6 weeks. The last period of splinting is for protection at night, which continues for 3 – 6 months after surgery (Chin and Chan 1998; Al-Qattan 2003). Unrestricted active and passive motions are permitted after immobilization. Improved active motion of shoulder flexion, abduction, and external rotation is expected after tendon transfers. Post-operative improvement in external rotation of greater than 45° and abduction of greater than 60° has been reported for these transfers (Kozin et al. 2002).
With an internal rotation contracture and limitation in external rotation movement it will not be possible to bring the hand to the mouth in a normal position without compensatory motions. This inadequacy makes itself manifest with the trumpeters sign where the abductors are used unduly so that the angle between humerus the trunk increases during hand to mouth movement (Nath et al. 2006). Although this phenomenon is widely acknowledged in the OBPP literature, (Al-Qattan 2003; Pagnotta et al. 2004; Pearl et al. 2006) in our experience the exact opposite is also valid. Whilst splint usage following six weeks casting is essential for protecting the newly transferred muscle from undue elongation, this also increases the risk of developing an external rotation contracture and limitation in internal rotation movement with long-term utilization. In our orthotics department we have encountered numerous patients with zero or even negative internal rotation. Since in most studies the result of the operation is evaluated with the improvement in external rotation and abduction if the patient demonstrates improved global shoulder function, the aggregate Mallet Score and Toronto Scale, widely used classifications to indicate the degree of impairment in OBPP, will increase even if there is a decrease in range of internal rotation (Clarke and Curtis 2001; Ozkan et al. 2004; Waters and Bae 2005; Pearl et al. 2006).
To overcome this problem we have developed a modified shoulder abduction splint with adjustable internal-external rotation/abduction-adduction ranges. The main aim of this modified splint is to allow a desired position of the joint as the newly transferred external rotation muscles gain strength and to maintain a balance in the joint between two unequal forces without jeopardizing the transfer. This splint allows for the physiotherapist to adjust the internal-external rotation in concurrence to the needs of the patient; even on a daily basis when required.
The aims of this article are to share our thoughts concerning a problem that is usually not given sufficient consideration; to describe this new adjustable shoulder abduction splint and to share the preliminary results attained.
Materials and methods
In our orthotics department, we treat patients who have undergone transfer of the latissimus dorsi and teres major to the greater tuberosity insertion of the rotator cuff. These patients require protective orthosis following six weeks in a shoulder spica cast (Chin and Chan 1998; Al-Qattan 2003). We manufacture these orthoses, at the same time a physiotherapist begins electrical stimulation for muscle re-education and active assistive movements for recovering normal range of motion and muscle strength especially of external rotators. Electrical stimulation for muscle re-education is advocated in the literature (Burridge and Ladouceur 2001; Brushart et al. 2002, 2005).
An adjustable shoulder abduction orthosis was designed to resolve some of the problems encountered during post-operative period in this group of patients following muscle transfer. Ethical approval for the study was obtained from the Ethical Committee of Hacettepe University.
Splint design
The orthosis is custom made directly on the child's torso and arm. The orthosis consists of three main components and two adjustable connecting components. One of the main components is the torso piece with anterior closure secured with Velcro strapping and extending from over the anterior superior iliac spine to as high into the axilla as anatomically feasible. The other main components are the arm and forearm pieces. The forearm component supports the forearm in neutral pronation-supination and extends over the wrist to support it in the functional position if necessary; the thumb and the fingers are left free. All three components are made of thermoplastic materials. The adjustable connecting components or tubes are made of steel. For internal/external rotation control, there are two tubes one rotating inside the other with corresponding holes every 1.5 cm. The stationary tube with the wider diameter is attached to the posterior arm piece; the rotating one with the smaller diameter, after being bent to keep the elbow at 90° flexion, is attached to the posterior forearm component. To give the desired degree of internal/external rotation, adjustments are made by simply rotating the smaller tube within the wider one. For stabilization, the cap screw is tightened. For the adjustment of abduction/adduction two other tubes, connecting the arm and torso components, with a mechanism similar to a length adjustable cane or crutch is utilized and a shoulder strap is sometimes added across the contra lateral shoulder to decrease migration of the orthosis (Figures 1 and 2).
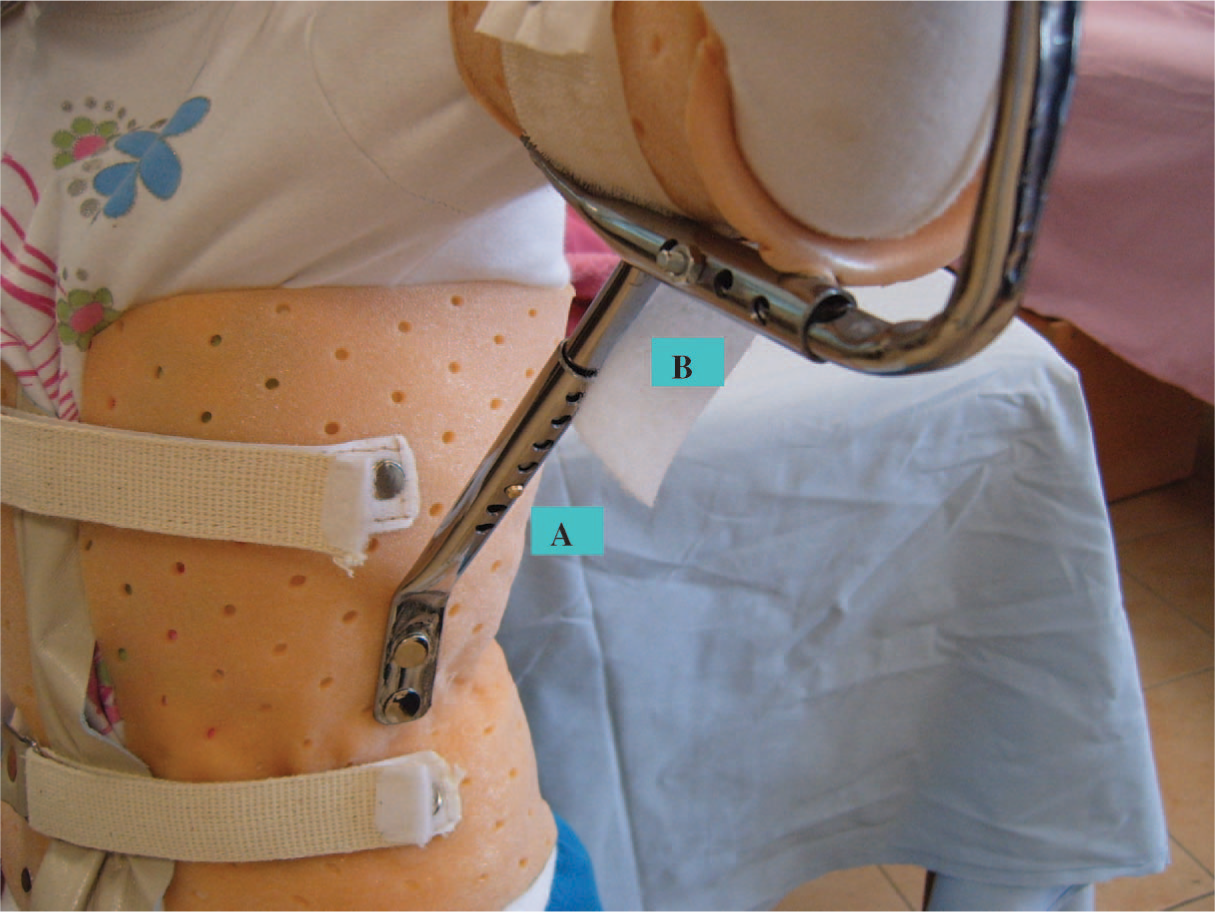
(A) Abduction/adduction degree adjustment pin; (B) Internal/external rotation degree adjustment pin.

A physiotherapist adjusting the orthosis.
Preliminary results with the orthosis
We have used the new adjustable orthosis in five patients with a mean age of 4.4 years and an age range of 2 – 7 years. Three patients had undergone m. Latissimus dorsi transfer only. The other two had a combination of procedures; the 4th patient had an M. Latissimus dorsi transfer and M. Subscapularis release, the 5th patient had an M. Latissimus dorsi and M. Teres major transfer. The five patients were referred to our orthotics department six weeks after their operation for a shoulder abduction orthosis replicating the shoulder spica cast; and to the physiotherapy department for muscle re-education. While receiving treatment the physiotherapist adjusted their orthosis on a weekly basis in favor of internal rotation as the external rotators gained strength. We evaluated these patients with the Mallet and Toronto scales (Mallet 1972; Clarke and Curtis 2001) following a period of 45 days, meaning that they had all been weaned to nocturnal use of the orthosis and had finished their daily physiotherapy programme and were being followed with a home programme. Our first impression was that all patients had complied with the orthotic programme. There was no compromise in the position of the orthosis which the physiotherapist had adjusted; and none of the caregivers had changed the position that the physiotherapist had determined depending on the outcome of her/his treatment. There was no problem of maintenance of skin integrity; caregivers were satisfied with this orthosis since the child was less frustrated by the restriction of movement. Parents said, as an oral feedback, that the children did not have anger tantrums insisting that the orthosis be taken off.
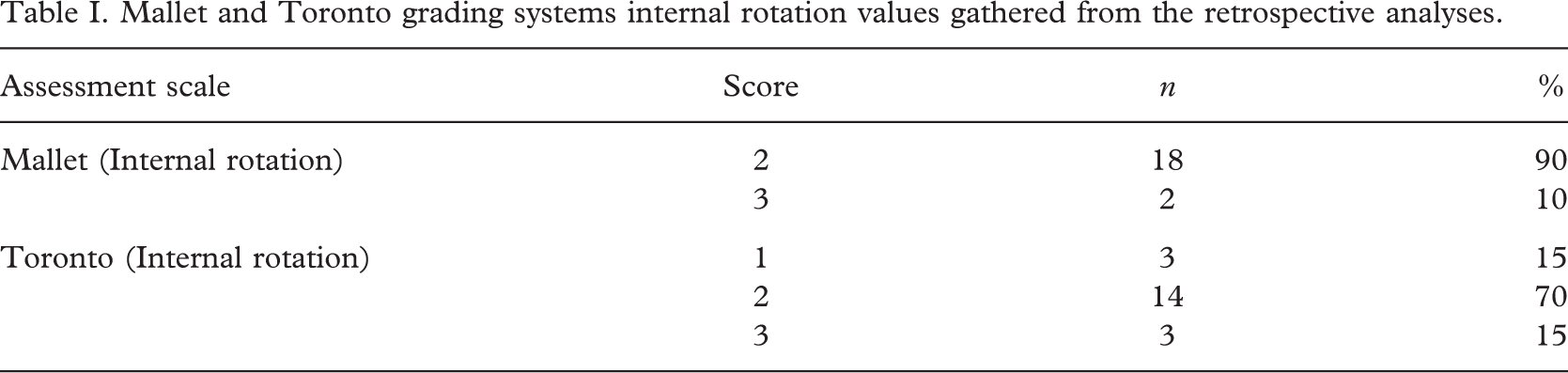
The most impressive outcome was that there was an increase in internal rotation range manifesting itself by the related items of the Mallet and Toronto grading systems, without a sacrifice on behalf of external rotation range. Although all subjects showed an increase in internal rotation range compared to former patients, the number of subjects was insufficient for a statistical method to be applied. However, we performed retrospective analyses in a randomly chosen group of 20 patients, with a mean age of 3.15 years who were treated with a static shoulder abduction orthosis and physiotherapy. Internal rotation values of the Mallet Classification System obtained from the patient files one month after using the static shoulder abduction orthoses showed that the hand to back score was II in % 90 of the patients. This value indicates that it was impossible for the patients to bring the dorsum of their hand to their backs, meaning a serious limitation in internal rotation range. Only % 10 could bring their hands to the spine at the level of S1 (Mallet III); none of the 20 patients could bring their hands to the level of T12 (Mallet IV) (Table I). Of the five patients who were given the new adjustable orthosis, two of the patients had a Mallet II score; the other three had Mallet III score (Table II).
Mallet and Toronto grading systems internal rotation values gathered from the retrospective analyses.
Mallet and Toronto grading scores of the five patients using the new adjustable orthoses.
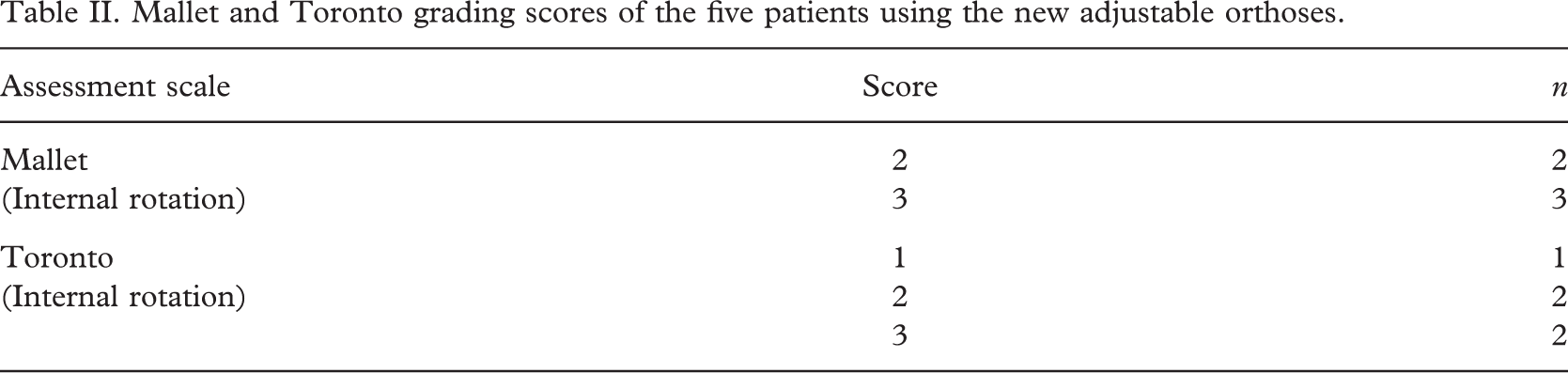
When the internal rotation of the arm was evaluated by the Toronto Scale, % 15 of the patients had showed contraction but no movement (Toronto 1), % 70 of the patients were able to bring their extremity to less than half of the total range (Toronto 2), and % 15 were able to bring their extremity to more than half of the range of internal rotation (Toronto 3) (Table I). Of the five patients that were given the adjustable orthoses, one patient exhibited contraction but no movement (Toronto 1), two patients were able to rotate their extremity below half the normal range of internal rotation (Toronto 2), and two patients had the ability to rotate their extremities above half the normal range of internal rotation (Toronto 3) (Table II). Although these results confine to only five patients they imply that the patients benefited from the adjustable orthosis.
Discussion
Although it is essential to protect the surgery with the utilization of a shoulder abduction orthosis which prevents the elongation of the transferred M. latissimus dorsi tendon to the external rotators; in the long term it may likely cause an external rotator contracture or shorten the posterior capsule of the glenohumeral joint. Thus the persistent usage of the splint may sometimes reverse the disorder (Aydin et al. 2004; Pearl et al. 2006).
The objective of most research is to determine the effects of correction of external rotation weakness and internal rotation contracture which usually means subscapularis and pectoralis major muscle releases and transfer of the latissimus dorsi/teres major muscles to the rotator cuff. And the result of the operations are evaluated with passive and active motion gain in abduction, external rotation and the aggravate Mallet score showing global shoulder function following the operation (Beauchamp et al. 1998; Ozkan et al. 2004).
Contradictory to our observations, Waters and Bae (2005) have reported that each element of the modified Mallet Classification, including hand to spine motion (showing ability of internal rotation), had improved following tendon transfer procedures.
The restoration and preservation of the range of external rotation is the primary objective of surgical protocols. Although increases in external rotation movement following release a M. Latissimus dorsi transfer or M. Latissimus dorsi and M. Teres major transfer are given in detail in many studies, the decrease in internal rotation is either not mentioned (Al-Qattan 2003; Pagnotta et al. 2004), or mentioned but not dwelt upon. Some studies have acknowledged that there is a significant loss of internal rotation (Aydin et al. 2004; Pearl et al. 2006) but do not dwell upon the functional implication of such a loss. Bielocerkowski et al. have claimed that, since most outcome instruments were developed by surgeons, their items might not measure important therapy or family oriented variables; such as developmental milestones and compliance with home exercise programs. Pearl et al. (2006) have reported that for most patients the decreased internal rotation was within the functional range, however, if the post-operative passive internal rotation had a negative value there would be severe functional loss and this would prompt consideration of additional intervention such as internal rotational osteotomy (Bielocerkowski et al. 2005; Pearl et al. 2006). We believe that there is no need to tolerate a loss in internal rotation for the sake of a full range external rotation since most demanding daily activities also necessitate normal internal rotation or at least neutral position of the arm.
Conclusion
The aim of orthotic and physiotherapy treatment following muscle transfer for OBPP is essentially to restore a physiologic balance between internal and external rotation without jeopardizing the effectiveness of the operation. For this we designed an adjustable orthosis that would enable the therapist to make adjustments as required and believe that our study addresses and endeavours to find solutions to a hitherto neglected issue in the treatment of infants who have undergone muscle transfer following OBPP. The results attained from this preliminary study warrant further studies presenting statistical analyses and long-term results.