
Abstract
The objective of this study was to compare the effects of wearing an insole with toe separator and night splint on hallux valgus and intermetatarsal angles and also on the intensity of pain in patients suffering from painful hallux valgus deformity. Subjects in this study consisted of 30 female patients aged 19 – 45 years (mean 27.83 ± 8.91) who were divided into two groups. The first group received the insole and toe separator and the second group received night splint. Hallux valgus angle and intermetatarsal angle were radiographically measured before and after a 3-month study period. Foot pain intensity was assessed by 10 cm Visual Analogue Scale before and after intervention. After statistical analysis the reduction of pain was significant in the first group (p < 0.05) whereas in the second group no significant difference was obtained. The hallux valgus angle and intermetatarsal angle decreased in both groups; however, the reduction was not significant. According to the results of this study, using night splint seems to have no effect on painful hallux valgus deformity. On the other hand, although the insole with toe separator significantly decreased the pain intensity in these patients and was a good option for pain reduction, it was not effective in improvement of the great toe angles.
Introduction
Hallux valgus is a complex progressive deformity affecting the forefoot in which lateral deviation of the great toe is the most obvious feature. It is associated with a bunion, i.e., the prominent first metatarsal medial eminence and overlying chronically inflamed adventitious bursa. The deformity comprises medial deviation of the first metatarsal, giving rise to a widened forefoot and lateral deviation with or without pronation of the hallux. The progressive incongruity of the first metatarsophalangeal (MTP) joint and secondary osteoarthritis is common and crowding of the lesser toes can result in hammer deformities with subluxation of the lesser MTP joints (Thomas and Barrington 2003).
Hallux valgus occurs almost exclusively in shoe-wearing societies. It has been shown that there is an extremely high prevalence of bunions in American women in the fourth, fifth, or sixth decade of life, implicating that the footwear is a cause of this deformity (Coughlin and Thompson 1995). Likewise in Japan, Kato and Watanabe (1981) showed that the prevalence of hallux valgus increased dramatically following the introduction of high-fashion footwear after World War II. This theory is supported by a study from China (Lam and Hodgson 1958) where the prevalence of hallux valgus was shown to be 15 times higher in people who wore shoes than in those who did not.
Although improper footwear seems to be the primary extrinsic cause of hallux valgus, there are some intrinsic factors as well. Mann and Coughlin (1993) reported that pes planus has some influence on bunion formation, whilst Inman (1974) suggested hindfoot pronation as a major cause of this problem. Metatarsus primus varus which is often associated with a hallux valgus deformity is characterized by an increased angle between the first and second metatarsals. Other intrinsic causes of hallux valgus include contracture of the Achilles tendon, generalized joint laxity, hypermobility of the first metatarsocuneiform joint and neuromuscular disorders (including cerebral palsy and stroke) (Coughlin 1996). Heredity is also thought to be a factor in the development of hallux valgus deformity. Coughlin (1996) noted that a bunion was identified in 29 (94%) of 31 mothers of children who had hallux valgus.
Bunions range in severity from mild to severe anatomic deformity of the hallux valgus angle, intermetatarsal angle, and sesamoids (Mann and Coughlin 1993). The first treatment considered for people with symptomatic bunions is the shoe modification. Adults with bunions of mild-to-moderate severity may be candidates for orthotic treatment or surgical correction. Often, pain, blistering, and bursal inflammation can be relieved by elimination of friction over the medial eminence. Evaluation of the patient's footwear may prove helpful for making recommendations for modifications or a change in size or style of the shoes. A wider toe box may reduce symptoms substantially (Coughlin and Thompson 1995). Stretching of areas of the shoe that cause increased pressure can result in complete relief of the symptoms overlying a painful bunion. A patient who has pes planus can be managed with an orthosis. Despite non-operative treatments, some patients eventually need operative management (Coughlin 1996).
Method
Subjects
Patients recruited to this study consisted of 30 female subjects ranging in age between 19 and 44 years (Table I summarizes the patients' characteristics). Inclusion criteria were having a painful bunion and the hallux valgus angle 35° or less and the intermetatarsal angle of 15° or less (Mann and Coughlin 1993). All patients had mild to moderate bilateral flexible hallux valgus. Any foot that had previously undergone bunion surgery, had hallux rigidus, hallux limitus was excluded in the study. Other exclusion criteria were age younger than 19 or older than 45 years, previous use of foot orthoses, rheumatoid disease, and pregnancy.
Patients' characteristics: Mean and standard deviation of age, height, weight and BMI.

Human research ethics committee of Iran University of Medical Sciences approved the study protocol and patients taking part in the study also gave their informed consent.
Randomization and treatment
In this clinical trial study, a judgmental sampling method from the convenient samples was recruited. Data were collected in this study by means of a demographic questionnaire, clinical evaluation and observation of the patients and radiographs. Subjects were randomly allocated in either first group receiving insole with toe separator or the second group receiving night splint as their treatment option.
The semi-rigid insole in this study was a total contact insole made of full length polyfoam material and a polyethylene part as the middle layer, ending before metatarsal heads. The toe separator which was also used along with the insole was made of plastazote material to make space between the great and the second toe and also provides some cushioning (Tang et al. 2002). The night splint consisted of a polyfoam soft part and a rigid polyethylene bar on the medial side of the hallux (Crawford et al. 1997).
Both orthotic options were custom fabricated made by negative cast technique. Patients in both groups were advised to purchase shoes 1 size larger than their normal shoe size so that the total contact insole with toe-separator would fit inside the shoe. Even though the second group did not have any orthosis to insert in the shoe, they were also to advised to purchase shoes 1 size larger eliminate the bias of the pain relief due to the reduced pressure on the medial side of first metatarsophalangeal joint as would have been probably attained in the first group.
Assessment
The intensity of foot pain was evaluated by the 10 cm Visual Analogue Scale (VAS) before receiving the intervention and after the 3-months follow-up period. Hallux valgus angle and intermetatarsal angle were obtained through radiographic measurements before and after the 3-month study period.
Statistical analysis
The Kolmogrov-Smirnov (K-S) test was used to assess the normal distribution of the data. The paired t test was used to compare the angles (i.e., hallux valgus angle and intermetatarsal angle) and pain intensity based on VAS scores before and after the study period in each group. The independent t test was also used to compare the angles and pain intensity scores between the two groups before and after receiving the intervention. Statistical significance was set at p < 0.05.
Results
Thirty female patients took part in this study (Table I) suffering form painful flexible hallux valgus. They were randomly allocated in either first or second group.
The normal distribution of data was tested by the means of K-S test which showed that the data were normally distributed. Using paired t-test, it was revealed that intensity of foot pain decreased significantly after 3 months in patients wearing the insole with toe separator (p < 0.05) this showed that the intervention was effective in reducing foot pain intensity (Table II). However, the pain reduction was not significant in the second group wearing a night splint. The differences between the amount of hallux valgus angles and intermetatarsal angles were insignificant in both groups after the 3-month study period.
Data comparisons of the study variables before and after the 3-month study period.
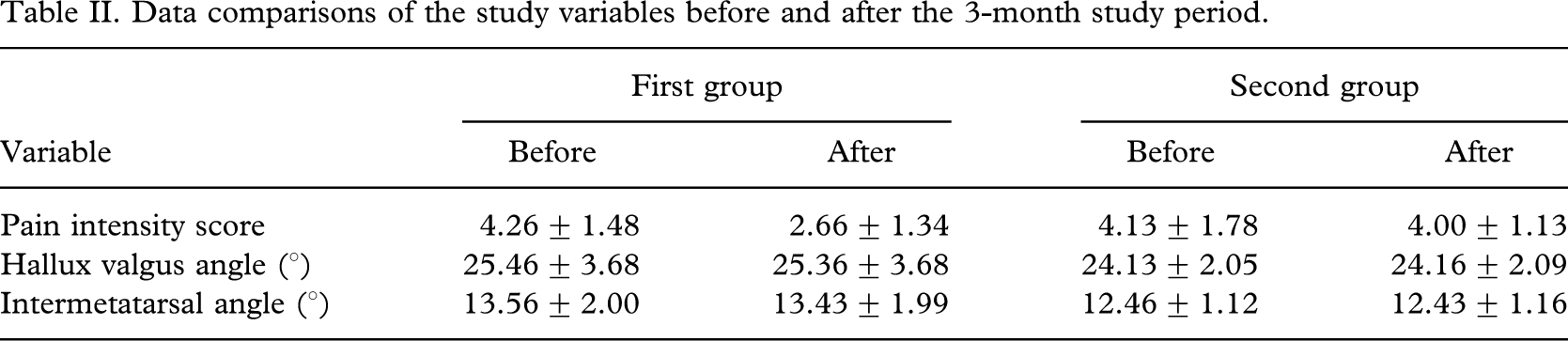
The independent t-test before the intervention showed no statistically significant difference in amount of hallux valgus and intermetatarsal angles and also pain intensity score between two groups. After the 3-month study period the difference in amount of hallux valgus and intermetatarsal angles was still insignificant, but the pain intensity score was significantly different (p < 0.05).
Discussion
Although the patients participated in the present study were diagnosed by having only mild to moderate hallux valgus deformity, the foot pain had caused notable disability especially while walking. In this trial, the authors were able to evaluate and compare the effectiveness of two orthotic treatment options.
When hallux valgus is caused by intrinsic factors such as pronation of the hindfoot forefoot varus, Achilles' tendon contracture, joint laxity, hypermobility of the first metatarsocuneiform, or neuromuscular disorder treatment strategy should focus on restoring an anatomically and biomechanically functional foot (Coughlin 1996). In this patient population, constructing a total contact insole according to the foot's positive mould with adequate arch support and posting would be a better intervention because anatomic alignment of the foot can be correctly restored (Nawoczenski 1997).
Use of insole with toe-separator caused significant reduction of pain in the first group. The reason of this reduction might be because toe-separator can correct the alignment of the toes and this functional realignment helps foot to propel better in the gait cycles.
On the other hand, the insole decreases the over pronation of the foot which is a known feature in these patients. These two factors together help maintain the foot structure in a biomechanically and anatomically functional state during both static and dynamic activities. The main advantage of the insole with toe separator was the restoration of correct anatomic alignment of foot.
However, in the second group the night splint could not improve the pain intensity of the patients. This might be because of this fact that mere nocturnal use of splint is a limited usage in a static way and this cannot reduce the pain in the dynamic activities of daily living.
Regarding the angulations featured in this deformity, the 3-months study follow-up appeared not to be long enough to make structural changes, yet preventing the increase in these angulations which is another feature of this deformity to be progressive.
Conclusion
The insole with toe separator seems to be an effective orthotic treatment to reduce the pain and in patients with painful hallux valgus deformity. On the other hand, the night splint was unable to reduce the pain in these patients. Although neither orthoses decreased hallux valgus and intermetatarsal angulations, both prevented the increase in angles in the two groups.