
Abstract
The objective of this study was to compare the effectiveness of irremovable total-contact casts (TCC) and custom-made temporary footwear (CTF) to heal neuropathic foot ulcerations in individuals with diabetes. In this prospective clinical trial, 43 patients with plantar ulcer Grade 1 or 2 (Wagner scale) were randomized to one of two off-loading modalities: TCC or CTF. Outcomes assessed were wound surface area reduction (cm2) and time to wound healing (days) at 2, 4, 8 and 16 weeks. To evaluate safety, possible side effects were recorded at each follow-up visit. The results showed no significant difference in wound surface area reduction (adjusted for baseline wound surface) at 2, 4, 8 or 16 weeks (adjusted mean difference 0.10 cm2; 95% CI −0.92−0.72 at 16 weeks). At 16 weeks, 12 patients had a completely healed ulcer, 6 per group. The median time to healing was shorter for the patients using a cast (52 vs. 90 days, p = 0.26). Five patients with TCC and two with CTF developed device-related complications. It was concluded that: (i) the rate of wound healing is not significantly different for patients treated with CTF or TCC. The difference in wound surface area was small and not significant at any time during follow-up; and (ii) the difference in healing time (38 days) may have attained statistical significance if the numbers in these sub-groups (2×6) had been higher. Since there appears to be little difference in effectiveness between both off-loading modalities, further investigation into the benefits of CTF is warranted.
Introduction
Diabetic foot ulceration causes considerable morbidity affecting up to 15% of diabetes patients in their lifetime; 80% of amputations are preceded by foot ulcers (Boulton et al. 2004). The mainstay of any treatment programme, alongside infection control and maintaining vascular integrity, is effective pressure reduction (off-loading). Off-loading is important as peripheral neuropathy results in loss of pain sensation that is responsible for self-protective behaviour. Off-loading can be achieved in several ways.
The technique studied most often is total contact casting (TCC), often regarded as the reference treatment (Armstrong et al. 2005). A TCC is minimally padded and moulded carefully to the foot's shape, thus redistributing weight off the ulcer and protecting the foot from repetitive injury and contamination whilst allowing ambulation (Sinacore 1996). Yet several drawbacks have limited its use. TCCs are considered contraindicated for wounds with soft tissue infections or osteomyelitis (Boulton et al. 2004). It is a technically challenging application that, in inexperienced hands, can lead to skin breakdown and ulceration. The overall average rate for all types of complications was estimated to be 20%, with ulcer recurrence rates ranging from 9 – 57% (Sinacore 1996). Casting does not allow daily inspection or treatment of the wound. Re-applying the cast frequently is labour-intensive and therefore expensive. Patients often find the TCC to be an impediment whilst bathing, sleeping or driving and pre-existent postural instability can be aggravated. For practical purposes, therefore, clinicians often choose to compromise and settle for less rigorous off-loading modalities.
In The Netherlands, custom-made temporary footwear (CTF) (Figure 1) is widely used to off-load. CTF allows daily wound care and ambulation is less impaired than with a cast; patients are not required to return weekly for cast changes. Its ease of removal may, however, be its Achilles heel since insensitivity due to neuropathy may contribute to non-compliance. Several studies (Knowles and Boulton 1996; van de Weg 2002, Armstrong et al. 2005) have demonstrated poor compliance with removable devices. Despite their widespread use, evidence to support the effectiveness of footwear as a primary intervention is scant (Cavanagh 2004; Maciejewski et al. 2004). The only randomized controlled trial comparing shoes, albeit off-the shelf, with TCC was undertaken by Armstrong et al. (2001). The significant difference in cumulative wound survival (89% for TCC vs. 58% for half-shoes, p = 0.012) appears to confirm experts' opinion (Armstrong et al. 2005) that TCC is more effective than off-the-shelf shoes.

Custom-made temporary footwear (CTF).
However, the authors were unable to identify any studies comparing TCC with custom-made footwear.
Off-loading with TCC may be superior to other off-loading strategies studied so far, but practical limitations (Armstrong et al. 2001) can dissuade clinicians from using this modality. Treatment with CTF may be more practical but there are no published studies to date comparing TCC to custom-made footwear.
The authors conducted a randomized clinical trial to investigate wound repair in diabetes patients with plantar ulcers who were randomized for treatment with either TCC or CTF.
Research design and methods
Subject characteristics, in/exclusion criteria
Participants were enrolled from the rehabilitation departments of two hospitals between August 2001 and January 2005. All consecutive patients were considered for study enrolment. Inclusion criteria were confirmed diabetes, sensory neuropathy tested by a quantitative somatosensory threshold test using the Semmes-Weinstein 5.07 (10 g) monofilament (on first and fifth metatarsal heads, medial and lateral midfoot and heel), and a plantar ulcer Grade 1 or 2 using the Wagner scale (Wagner 1981). The grade was based on clinical examination and evaluation of a plain radiograph; the location of the ulcer and pre-trial ulcer duration were recorded. Patients unable to walk indoors, with dementia or life-threatening co-morbidity, ankle/brachial index <0.4 and/or osteomyelitis (determined by plain radiograph) were excluded.
Randomization
Patients were randomly allocated to one of two off-loading procedures: Total contact cast (TCC) or custom-made temporary footwear (CTF). Allocation was concealed using opaque, sealed envelopes. An independent person prepared a randomization list in advance with an equal number of treatment assignments (5/5) per block of ten to ensure approximately equal numbers of patients in each treatment group (Pocock 1991).
Characteristics of TCC and CTF
TCC. A well-moulded and minimally padded non-removable below-knee cast that maintains contact with the entire plantar aspect of the foot and lower leg was used. TCC was applied by a cast technician with at least five years experience using the Kominsky technique (Kominsky 1991). Prior to casting, a single layer of cast padding was applied. After debridement, the wound was dressed with aquacell (5×5 cm Hydrofiber [sodium carboxymethylcellulose] wound dressing with moisture-resorbing properties). Adhesive foam was used over bony prominences. Cast shoes with a polyphasic rocker were supplied; patients with poor postural stability were advised to use a crutch/cane to maintain balance. The cast was changed on a weekly basis for the duration of the trial (i.e., a maximum of 16 weeks).
CTF. The CTF was custom-made of felt and supplied with a rigid leather socket stiffened with Rhenoflex, a composite of rubber and plastic with thermoplastic properties. This ensures that movement of the foot in the shoe is restricted to an absolute minimum. The height of the shoes is twice the distance from the foot base to the lateral malleolus. The custom full-length insoles were made from cork and a plastazote and PPT (polyethylene foam and polyurethane) covering. Extra depth was provided in the inlay for the ulcer. To ensure maximal relief of pressure under the MTPs, the pivot point of the rocker bar was placed proximal to the MTPs and the outsole stiffened to facilitate the distribution of forces exerted on the foot. A plastic trial cast was always made for a test fitting to check the last measurements, innersole accommodation and balance before the shoe was completed. Patients were instructed to wear their footwear at all times whilst out of bed. Detailed instructions regarding routine care of the cast and shoes were given to all patients. All patients were advised to decrease their activity levels considerably (i.e., to one-third of their pre-morbid level). To avoid participation bias patients in the CTF group were relied upon to wear their shoes.
Co-interventions
Before the intervention ulcers were debrided of necrotic tissue; hypertrophic edges were removed. All patients received the same educational guidelines on foot care and general information on the importance of appropriate footwear. All patients attended the out-patient department regularly for device inspection. Wound care and wound debridement was carried out by a podiatrist blinded to treatment mode, and antibiotics dispensed if necessary. Patients having difficulty performing dressing changes were provided with assistance from a home care nurse.
Assessment of outcomes
Data were collected at baseline and outcomes assessed in all patients at 2, 4, 8 and 16 weeks. If patients had more than one plantar wound, the largest wound was used as the index ulcer for inclusion in this study. Two outcome measures were used. The primary outcome measure was reduction of wound surface area (WSA) during the 16 weeks follow-up. The WSA (cm2) was determined by tracing the perimeter of the wound onto clear plastic film. Wound measurement was undertaken by a research assistant blinded for the treatment; patients were instructed not to discuss the treatment with the investigator. The secondary outcome measure was time to wound healing in days. The exact moment of wound closure was identified by a patient's self-report. Wound healing was defined as complete epithelialization with no evidence of drainage or sinus formation. Subjects who discontinued were considered not healed and wound size recorded as last measured during follow-up.
A WSA reduction difference of 50% between groups (a reduction of 2 cm2 vs. 1 cm2, SD 1.0), could be detected with a sample size of 17 per group, yielding a power of 80%. An α of 0.05 was used.
Statistical analysis
Comparability of the two groups at baseline was assessed for demographic and clinical characteristics and baseline values of wound size, grade and location. The analysis of effectiveness was done according to the intention-to-treat principle. WSA changes since baseline were calculated for each participant for each moment of follow-up. Subsequently, differences in these changes between groups were analysed using linear regression analysis. All analyses were adjusted for potential confounding by difference in baseline WSA by entering the baseline WSA in the regression analysis. The authors present both crude and adjusted mean differences between groups in the reduction of WSA, including 95% confidence interval (95% CI); p values < 0.05 were considered significant. Analyses were carried out using SPSS 12.01 software.
Ethical considerations/side effects
Informed consent was obtained from all patients before baseline assessment and randomization. The clinical study protocols and the informed consent procedure were approved by the Medical Ethical Review Board, Onze Lieve Vrouwe Gasthuis, Amsterdam, The Netherlands. Side effects were carefully noted. Patients with serious side effects (abscess, osteomyelitis, re-ulceration) could be referred to an independent physician who could decide to discontinue treatment.
Results
Study population
Clinical characteristics of the patients are summarized in Table I. All but four patients presented with a Grade 2 ulcer. Differences between both groups were observed with respect to gender and baseline wound surface. The participant flowchart is shown in Figure 2. Follow-up was not achieved throughout the trial in four patients: One died, one was amputated on the affected side and two withdrew from follow-up (all from the TCC group). Minor abrasions not necessitating a treatment stop occurred in two CTF patients; five patients with TCC developed complications, leading to discontinuation before 16 weeks in two cases. All complications that occurred were local and related to the device (CTF/TCC).
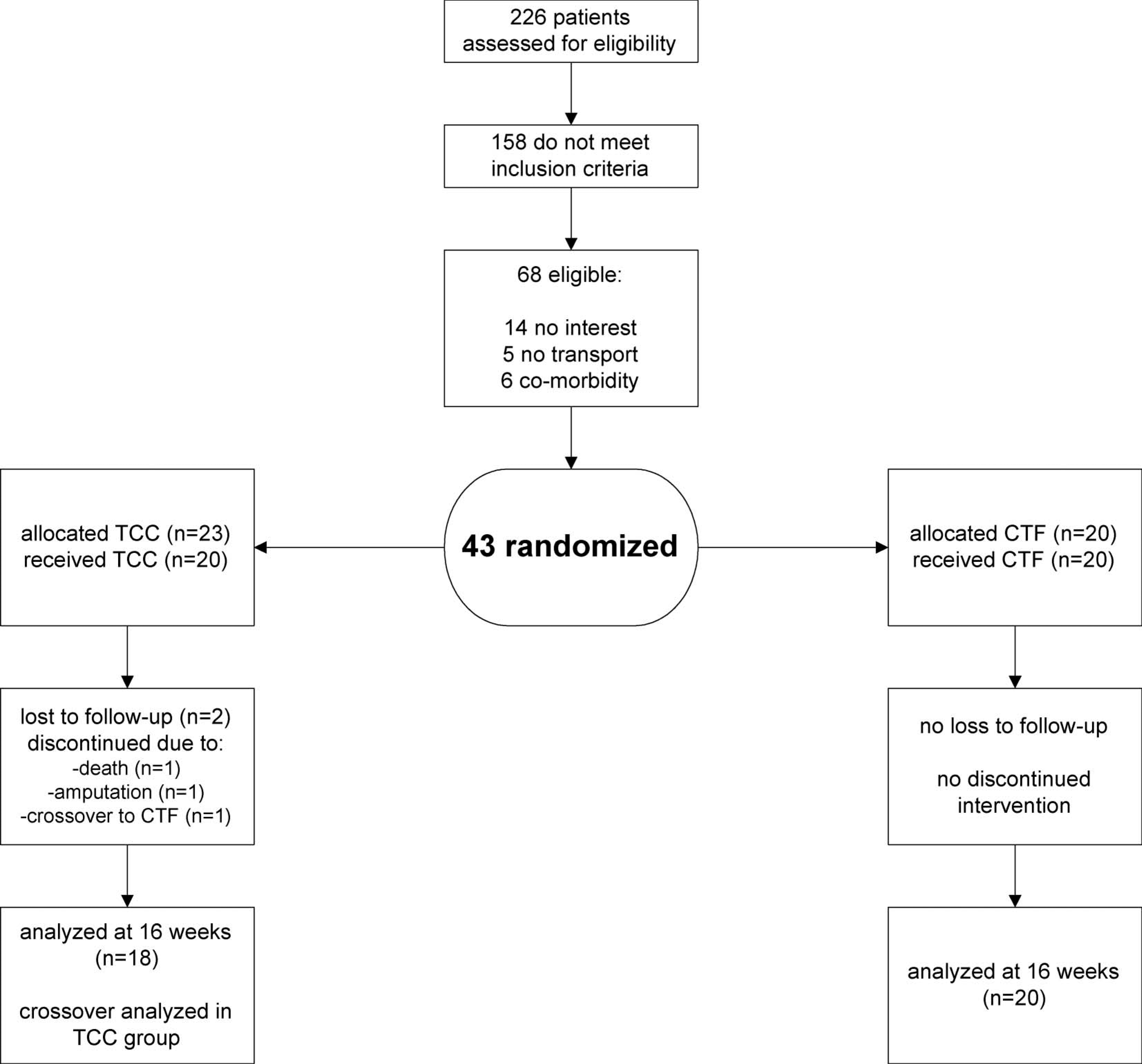
Participant flow through trial.
Baseline characteristics of diabetes patients with plantar ulcers.
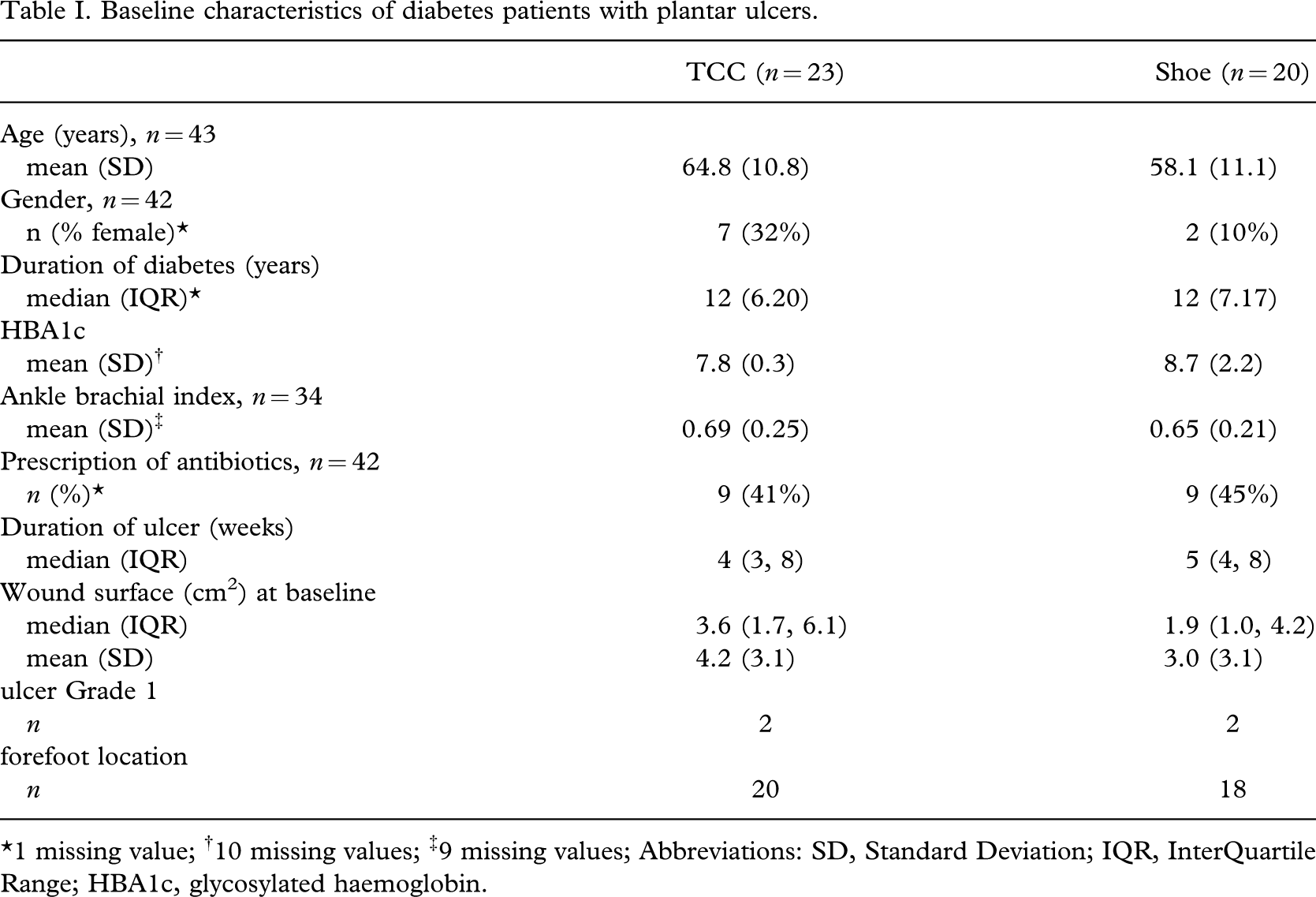
∗1 missing value; †10 missing values; ‡9 missing values; Abbreviations: SD, Standard Deviation; IQR, InterQuartile Range; HBA1c, glycosylated haemoglobin.
WSA reduction
Ulceration had been present for a median of 4 weeks in the TCC group and 5 weeks in the group using CTF. At baseline the median WSA was 3.6 cm2 in the TCC group and 1.9 cm2 in the CTF group. At 16 weeks the median WSA was 0.4 cm2 in both groups. The WSA reduction was not significantly different between groups at any point of time during follow-up (Table II). After adjustment for differences in baseline values, the difference between groups in reduction of wound surface was 0.10 cm2 (95% CI −0.92 to 0.72).
Decrease in wound surface (cm2) after baseline (mean, SD) in patients with diabetic foot ulcers using a cast or footwear∗.
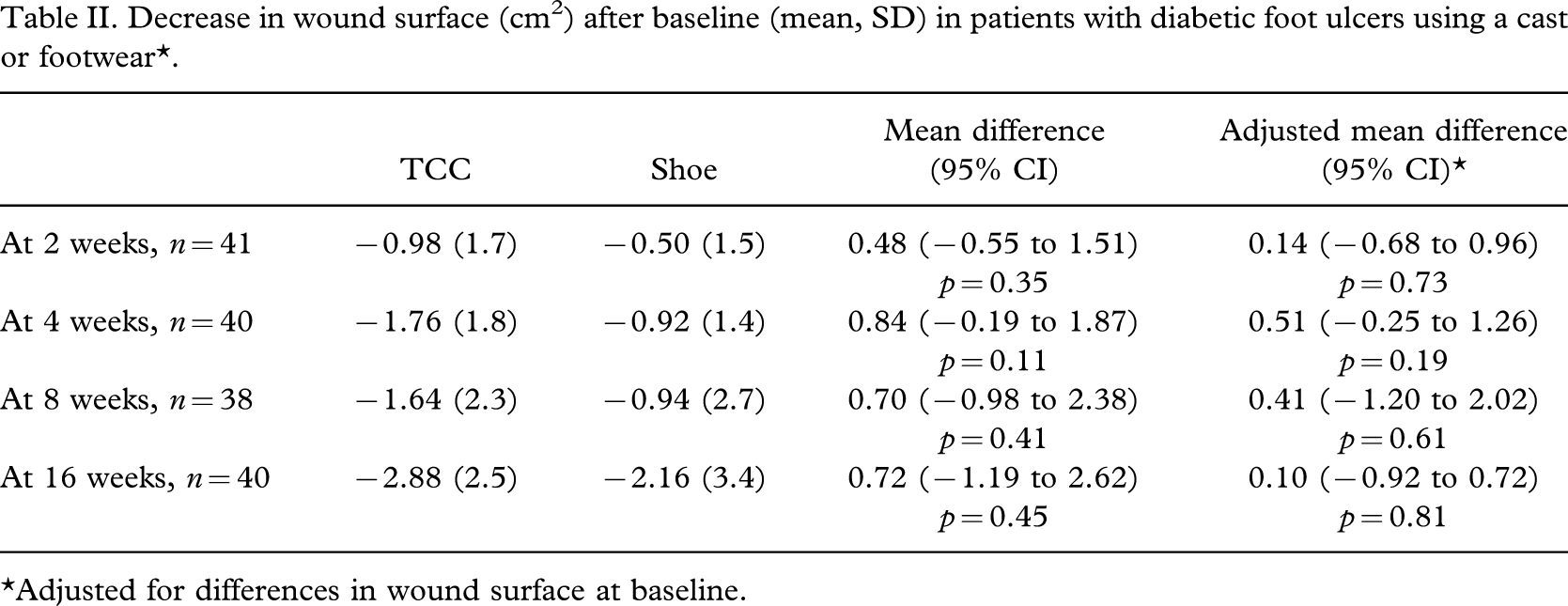
∗Adjusted for differences in wound surface at baseline.
Time to wound healing
Six patients wearing shoes (mean baseline WSA 4.5) and six patients using a cast (mean baseline WSA 4.7) had a completely healed ulcer. The mean time to healing was shorter for the patients using a cast: 59 (SD 39) days for TCC vs. 90 (SD 12) days for CTF, but the difference in this small subgroup was not statistically significant (t-test, p = 0.11). Patients without complete healing had median ulcer sizes of 0.8 cm2 (mean 1.1, SD 1.2) for CTF vs. 0.9 cm2 (mean 1.5, SD 1.6) for TCC at 16 weeks.
Discussion and conclusions
Neuropathic foot ulceration is associated with significant morbidity. Ulcers, soft tissue infections and osteomyelitis contribute to major and minor amputation (Boulton et al. 2004). The tremendous consequences for patients and caregivers press the need for an off-loading device that is both efficacious and practical. Bedrest and elevation of the involved extremity may facilitate healing, but can hardly be considered practical. TCC have been advocated by several authors as the reference treatment and the superiority of TCC over traditional dressing treatment, half shoes or removable cast walkers appears undisputed (Boulton et al. 2004; Armstrong et al. 2005). Insofar as the authors know, this is the first randomized controlled trial comparing off-loading by means of a standard TCC with custom-made footwear. Since the adjusted mean differences in WSA are less than 0.5 cm2 at each moment of follow-up, this study suggests that CTF may be as efficacious as TCC in reducing WSA and may be associated with fewer complications.
Studies investigating off-loading with shoes are limited to off-the shelf shoes comparing some form of therapeutic shoe with ‘standard’ treatment, i.e., the patients' usual footwear. Considering the widespread usage of shoes to off-load, it is surprising that the evidence to support their effectiveness is so scant. Systematic reviews of foot ulcer prevention (Mason et al. 1999; Spencer 2005) found only one study that had assessed the efficacy of therapeutic shoes. In this controlled before-after design (Uccioli et al. 1995) patients were assigned to wear either their own shoes or manufactured therapeutic shoes. The relapse rate was significantly lower in the latter (28% vs. 58%), although alternate allocation leaves open the possibility of bias. One randomized controlled trial involving 63 patients (Armstrong et al. 2001) compared half-shoes with TCC and found a statistically significant higher proportion of healed wounds in the TCC group (89% vs. 58%). Half-shoes suspend the forefoot in mid-air, causing instability and increased pressure on the midfoot. A cautionary note is that drop-out in two treatment arms differed to a large extent (24% TCC vs. 4% half-shoe) whilst analysis was not according to the intention-to-treat principle. The authors also summarized six potential negative detractors limiting the applicability of TCC in daily practice. The proportion of healed wounds is considerably lower in this present study than in the study by Armstrong et al. (2001). A difference in the inclusion criteria (Grade 1A ulcers vs. predominantly Grade 2 ulcers in this present study) may explain part of the difference; the higher compliance in the present study may also be a contributory factor.
Whilst casting may be effective, the regimen is not always well accepted and patients may be reluctant to have the casts renewed. In addition, applying TCC is time-consuming and therefore relatively expensive. Moreover, casts only present a temporary solution. Ultimately, the major challenge is to prevent long-term ulcer recurrence which, arguably, can only be achieved by off-loading with custom-made shoes. An advantage of CTF is that the trial cast can be utilized to make the definitive shoe. In The Netherlands, therefore, off-loading is primarily achieved with custom-made shoes. An important stimulus is nationwide public health service coverage and the affiliation of most hospitals with an orthopaedic shoe technician. It is reassuring that shoes may be as effective as casting with respect to wound healing and it is, in the authors' view, somewhat premature to state casting as the reference treatment, considering the limited evidence on which this opinion is based (Armstrong et al. 2001; Spencer 2005).
Since shoes can be removed and TCC cannot, a difference in compliance is unavoidable. In fact, as Armstrong et al. (2005) have pointed out, the TCC's main asset may be to force compliance inadvertently. This may be a great bonus in a group with proven poor compliance (Knowles and Boulton 1996; Van de Weg 2002). Compliance in the CTF group was not recorded, but it can be safely assumed that some patients were non-compliant, at least partially. Non-compliance may account for the longer time to heal (38 days) in the sub-group of CTF patients with healed ulcers. Activity monitoring has shown (Armstrong et al. 2003) that the majority of patients wearing removable devices use the off-loading device during less than half of average daily activity. From the literature, it is unclear if compliance can be improved by specific measures such as frequent counselling and improved education. In the present study the authors tried to stimulate compliance by stressing the need to wear the prescribed footwear at all times whilst out of bed, but lack of compliance was considered as a ‘natural’ and unavoidable consequence of shoe therapy. It was chosen to investigate effectiveness (the extent to which an intervention does what it is intended to do in a population) rather than efficacy (the extent to which the intervention produces beneficial results under optimal conditions). The authors therefore feel that the present results can be more easily generalized to clinical practice than if adherence had been strictly pursued. If compliance as a possible confounder had been included, the results could have been positively biased towards shoe therapy. Nonetheless, even allowing for a poorer compliance in the shoe group, the outcome in terms of wound reduction was similar in both groups. A possible lower activity pattern in the TCC group emphasizes rather than contradicts our conclusion that CTF may be as effective as TCC.
This study has several drawbacks. Follow-up, for practical purposes, was relatively short. The authors therefore cannot address the long-term consequences of either therapy. With regards to blinding, it was obviously impossible to blind the patients to the treatment. It was found that blinding the investigator proved to be difficult too in a number of cases, with patients either ‘giving away’ the treatment despite admonishments, or the investigator recognizing the side effects (e.g., the TCC imprint). As the investigator was in no way involved in the treatment nor biased toward the treatment procedures it is believed this had a negligible effect on the outcome. Time to heal (the secondary outcome measure) was determined by the patient's self-report. The authors are aware that this introduces some degree of unreliability but, generally speaking, patients with ulcers are extremely keen to see their wound heal and therefore their report can be considered quite accurate. Naturally their observations were always corroborated at follow-up visits.
Despite a priori sample size calculations, sample sizes were too small to investigate the possible confounding effects of the baseline characteristics Hba1c and sex. The authors were able to adjust all analyses for potential confounding by differences in baseline ulcer surface, but a larger sample size might have resulted in better similarity of groups at baseline.
In conclusion, considering these limitations this study cannot pretend to offer any definitive answers but may be interpreted as an encouragement to other researchers wishing to investigate the off-loading abilities of custom-made footwear.
Footnotes
Acknowledgements
This study was supported by a grant from Convatec Netherlands and the OFOM (Ontwikkelingfonds Orthopedisch Maatschoeisel). Neither was involved in the handling of data in any way or in the publication of this manuscript.