
Abstract
In patients with rotationplasty the biomechanical conditions in the ankle joint are altered dramatically. By displacement and reduction of the weight-bearing area of the joint, the stress affecting its cartilage is increased. The use of an exoprothesis results in skin and soft tissue irritation. Due to these biomechanical changes, a prearthrotic deformity or skin problems could be expected. The current study examines changes in 21 patients treated with rotationplasty (mean follow-up 13.5 years) because of a malignant bone tumour or a femoral segmental defect. Local tenderness, skin and soft tissue changes, problems with exoprostheses, and pain was assessed by clinical examination and documented. Osseous changes were evaluated by plain X-ray. A MRI-scan was also obtained in five patients. Hardened skin and blisters were located at the main loading areas of the rotated foot. These changes could be reduced by optimizing the exoprosthetic fit. Radiographically, a slight asymptomatic attenuation of the articular space was observed in four patients and a slight coexistent subchondral sclerosis with small osteophytes in one patient. No degenerative changes were observed on X-ray and no cartilaginous changes were observed on MRI. The results suggest that the foot is able to adapt to the load changes after this procedure and that rotationplasty does not cause an inevitable arthrosis in the ankle joint.
Introduction
Long-term survival of patients with malignant bone tumours has increased by the use of a combined therapeutic approach of chemotherapy and radiotherapy. Today, most of patients with osteosarcoma or Ewing's sarcoma survive long term (Cotterill et al. 2000; Paulussen et al. 1999, 2001; Winkler et al. 1993). It is therefore important to achieve good long-term as well as short-term results in terms of both functional outcome as well as psychosocial acceptance. Rotationplasty was first performed by Borggreve in 1927 (Borggreve 1930), and was introduced by Salzer in 1974 (Salzer et al. 1981) for the surgical treatment of malignant bone tumours of the distal femur. Due to further development of this technique, Winkelmann (1983) increased the indications for rotationplasty (Winkelmann 1986, 1996, 2000). Today it is possible to perform rotationplasty in patients with tumours located throughout the femur as well as the proximal tibia. Especially in very young patients the rotationplasty offers a good alternative to growing prostheses avoiding further operations due to complications or lengthening.
Rotationplasty achieves a good functional outcome in spite of completely altered biomechanical conditions (Gottsauner-Wolf et al. 1991; Hillmann et al. 1999, 2000a, 2000b, 2000c; Kotz 1997; Kotz and Salzer 1982). The ankle joint acts as the new knee joint (Figure 1) in an external below knee ortho-prosthesis. During gait the foot is flexed and unloaded in the swing phase, and extended weight loaded in the stance phase. These new functional gait pattern leads to a complete change of the weight distribution. In a cadaver study, Rosenbaum et al. (2003) could demonstrate a significant transfer on the loading zone to the posterior part of the talus, a significant reduction of the contact area and force, and a significant increase of the mean and maximum pressures. These results indicate that the rotationplasty causes pronounced changes in joint loading characteristics. For the orthopaedic surgeon the question raises whether these changed conditions subsequently leads to a secondary arthrosis of the ankle joint or the foot.
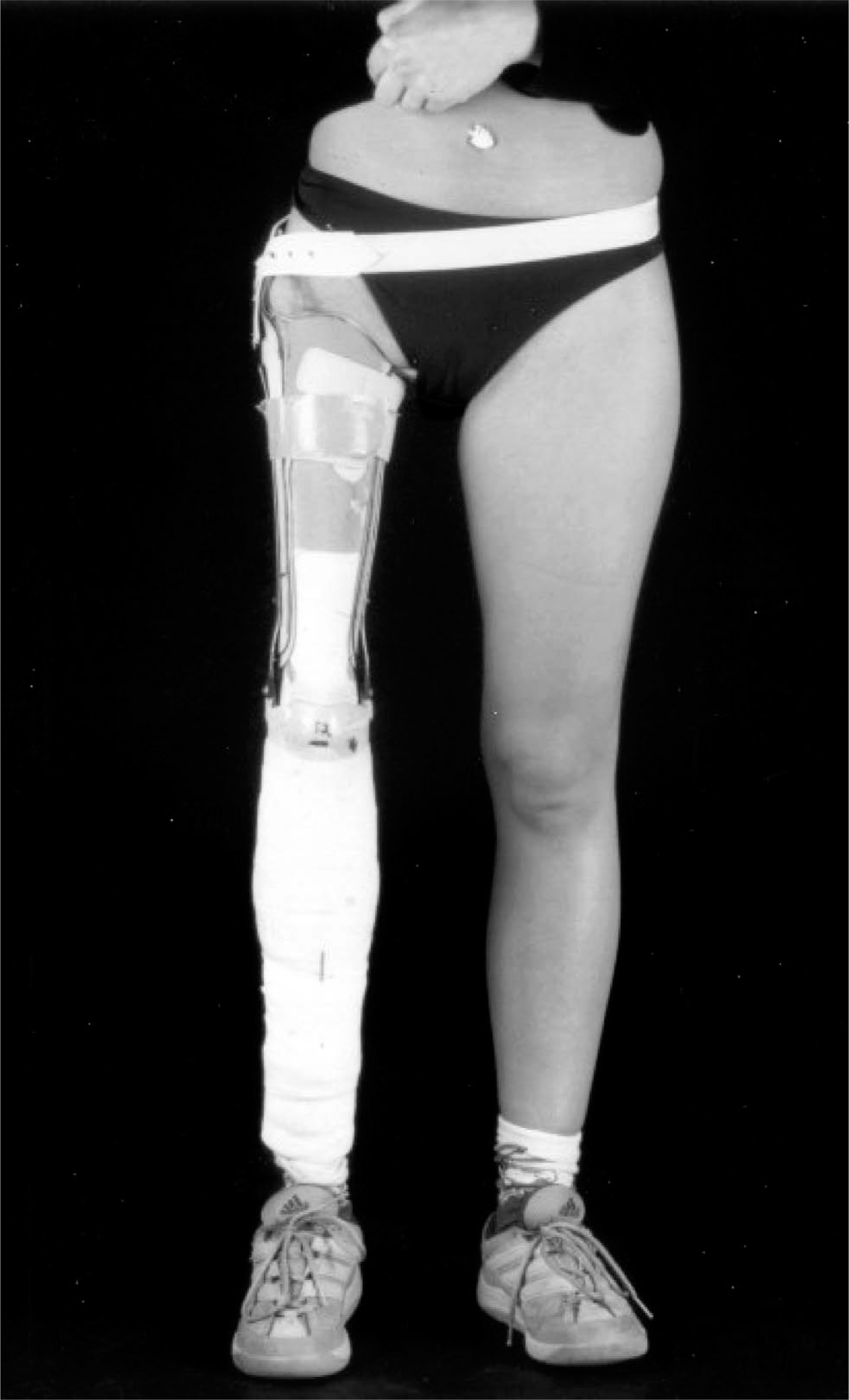
Patient who underwent a Rotationplasty with prosthesis.
Therefore the current study investigated long-term clinical and radiological joint changes, as well as prosthetic problems, in order to assess whether rotationplasty causes secondary arthrosis in the ankle.
Materials and methods
The authors retrospectively reviewed 21 patients (13 females, 8 males), who underwent rotationplasty between 1978 and 1993; 20 because of a malignant bone tumour (osteosarcoma in 16 patients, Ewing's sarcoma in three patients, malignant fibrous histiocytoma in one patient) and one because of a femoral segmental defect. The mean patient age at operation was 29.5 years (range, 7 – 65 years). In 17 patients, a rotationplasty type A1 was performed, according to Winkelmann (1983), and a type B3 in four patients. The mean follow-up time was 13.5 years (range, 10 – 25 years). Follow-up focused on daily and sporting activities, skin alterations as well as radiographic changes on X-ray and on MRI.
Local tenderness, skin and soft tissue changes, and malposition of the foot and toes were documented by clinical examination every year. Foot position and range of motion were thus determined. The ‘normal’ range of motion after rotationplasty should be 90° plantar-dorsal flexion, with the regular position of the foot defined as 90° plantar hyper-extended, without pronation or supination.
Anterior-posterior and lateral radiographs of the ankle joint with weight-bearing, as well as an anterior-posterior view without weight-bearing, were taken. The radiographs and MRI were commonly evaluated by one radiologist and two orthopaedic surgeons. Radiographs were assessed for signs of osteoarthritis: Attenuation of the articular space, subchondral sclerosis, formation of cysts, osteophytes or subluxation. The lateral view was further used to document the plantar arc.
In five patients a MRI scan (T1-weighted sequence, T2-sequence and PD-sequence) was available. Highly sensitive cartilage sequences were used in order to image early cartilage defects. Particular attention was paid to any cartilaginous changes, joint effusion or bone marrow oedema.
Results
All patients were free of pain and had no restrictions in their daily activities during the follow-up period. In particular, none of the patients reported any load-dependent pain, or morning stiffness suggestive of arthrotic problems in the ankle joint.
Skin and soft tissue changes were found in 11 patients. Hardened skin and blisters (Figure 2a, b) were located at the back of the foot (eight patients), and in the region of the medial (7 patients) and lateral malleoli (five patients). These skin irritations were particularly observed in very active patients (5 badminton players, 2 table tennis players, 1 mountain biker), although further operative treatment was not indicated.
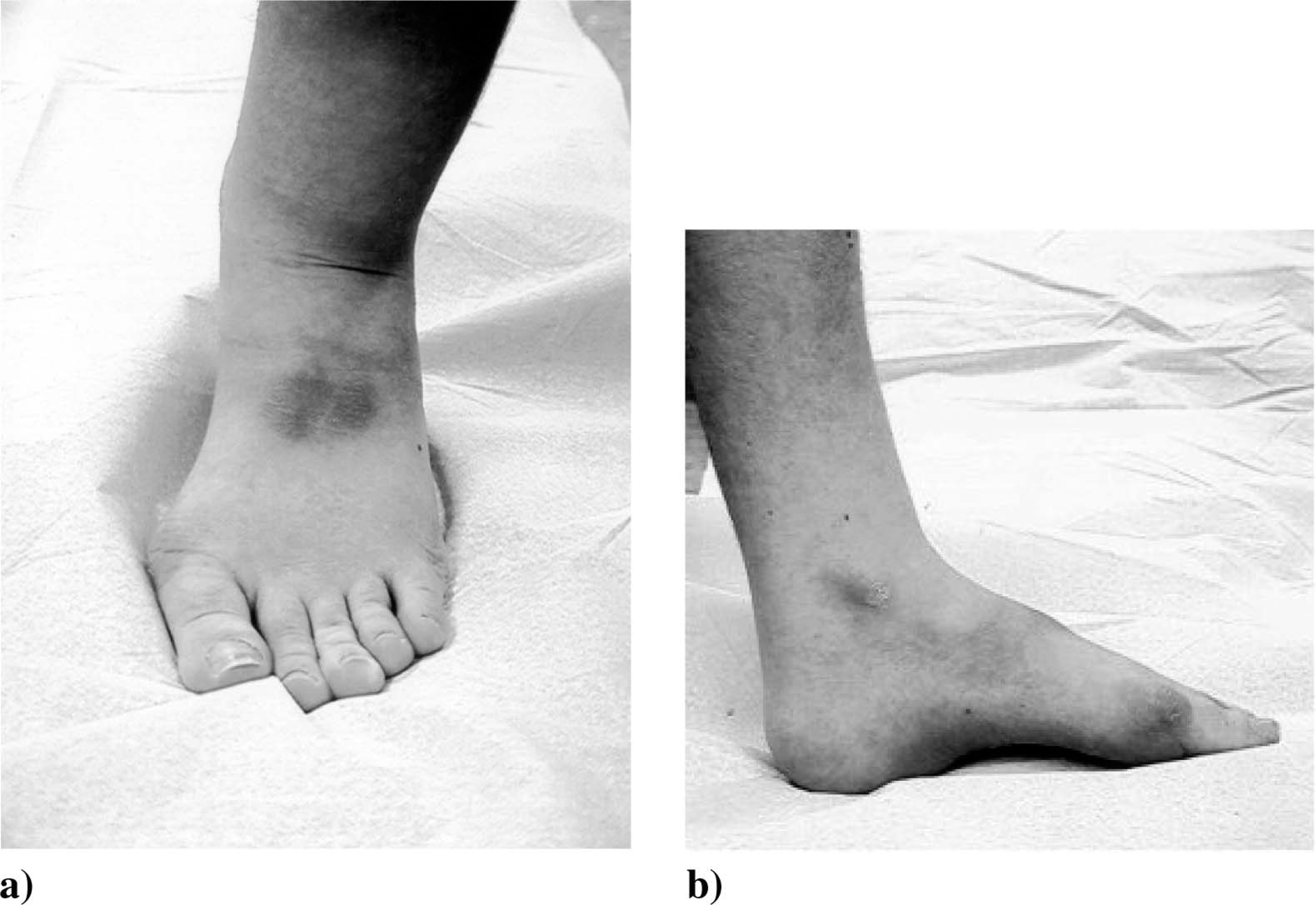
Typical skin alterations caused by the prosthesis.
Malposition of the foot (supination) with a consecutive enhanced skin alteration of the lateral aspect of the dorsal foot was observed in two patients after traumatic events (distal femur/distal tibia fracture), and a clear elevation of the plantar arch (Figure 3) was seen in 4 patients.

Slight attenuation of the articular space accompanied by an elevation of the plantar arc in lateral view in an asymptomatic patient.
On radiographic examination, a slight asymptomatic attenuation of the articular space was observed in four patients 12 – 15 years after surgery and a slight coexistent subchondral sclerosis with osteophytes in one patient (extreme active mountain biker).
A load-dependent change in the topology and alignment of the trabecular structure was observed in eight patients as well as a dorsally subluxation like position of the talonavicular joint in the lateral view in five patients. These changes were less distinctive in older patients (n = 3, >50 years) who were unable to optimally plantar flex their ankle joints. No other signs of degenerative changes were observed on plain X-ray and no cartilaginous changes were observed on special cartilage sensitive MRI (Figure 4a – d). In particular, no joint effusion or irregularity in cartilage thickness or shape was detected.
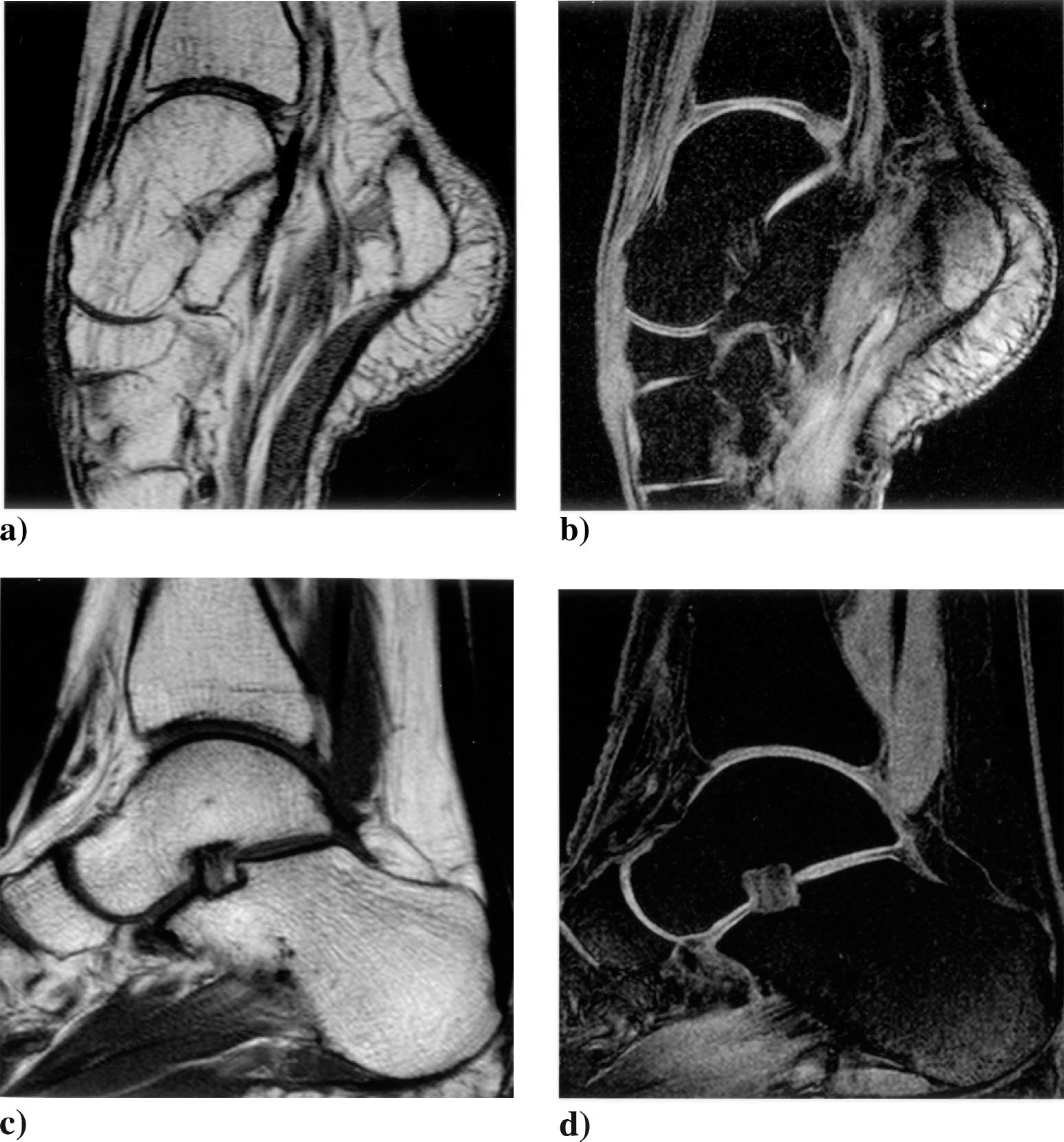
Comparison of the normal (c, d) and the rotated ankle joint (a, b) 10 years after surgery. The sagital T1 weighted turbo-spin-echo sequence (a, c) shows the changed anatomic appearance of the talus with adapted trabecular structures. The 3D T1 weighted fast-field-echo water selective sequence (b, d) shows the appearance of the articular cartilage with only mild changings in the rotated ankle joint.
Discussion
Rotationplasty is known as a safe procedure and is well accepted by patients as a form of operative treatment for malignant bone tumours, whenever conventional limb salvage is impossible (Gottsauner-Wolf et al. 1991; Hillmann et al. 1999, 2000c; Winkelmann 1996, 2000). It provides good functional results with fewer major complications than endoprosthetic replacement, but there is little data from long-term follow-up regarding the hyper-extended ankle joint (Hillmann et al. 2000b, 2000c; Kotz and Salzer 1982).
The current study presents to our knowledge the first systematically collected cases of 21 patients with a follow-up of at least ten years. During this study's follow-up, no patients complained of any pain suggestive of arthrosis in the ankle joint. Clinically, prosthetic-related problems and inevitable skin alterations were the only signs of the altered load-bearing situation. Hillmann et al. (2000a, 2000c) showed that the main loading areas of the rotated foot inside the prosthesis are: medially on the dorsal aspect, the plantar aspect of the mid-foot region, and the heel and toe region. The dorsal loading area of the skin has been smaller than the plantar area (Hillmann et al. 2000c). In patients with rotationplasty, skin alterations caused by the prosthesis are inevitable. As a result, hardened skin and blisters are common and are the result of adaptation to continuous mechanical irritation. These changes were more observed in very physically active patients and could be related to the type of the worn exoprosthesis and may develop after more or less extended and vigorous activities (Hillmann et al. 1999; Rosenbaum et al. 2003). The consequence often is a redesign or modification of the prosthetic shaft to improve the fit (Hillmann et al. 2000c). Sports prostheses manufactured with glass/carbon fibres allow physically active patients to perform activities such as badminton or table tennis. In these patients, the fixation of the foot should be very strong, ensuring firm contact with the prosthesis. Further on it is known from foot loading measurements and gait analysis that in type and the fit of the exo-prosthesis can have a significant influence on the joint contact forces. The body weight is transferred to the prosthetic shaft that encompasses the foot, which leads to a reproduceable decreased plantar and dorsal pressure measured inside the prosthesis (Hillmann et al. 2000c; Rosenbaum et al. 2003). Therefore continuous inspection enables early recognition of skin ulceration and further complications can be prevented by optimization of the exo-prosthetic fit, but it could be assumed that skin alterations are inevitable in patients who wear prosthetic devices.
As Hillman et al. (2000a, 2000c) described in vitro, one would expect to see pathological bony changes as a result of the altered load-bearing on the ankle joint. However, a misshapen of the talar trochlea, which was observed by other authors up to 20% (Capanna et al. 1992; Hanlon and Krajbich 1999; Heise and Minet-Sommer 1993), should be assumed as adaptive changes, because, consistent to all other authors, these changes did not correlate with clinical symptoms (Capanna et al. 1992; Hanlon and Krajbich 1999; Heise and Minet-Sommer 1993; Hillmann et al. 1999; Rosenbaum et al. 2003).
MRI revealed no cartilaginous defects and no early signs of arthrosis and without clinical symptoms suggestive of arthrosis, the radiological alterations seen were assumed to be part of an adaptation process.
However, from a biomechanical view, it could be assumed that the unphysiological load of the foot created by rotationplasty would result in arthrotic deformity at an early stage. The weight-bearing area of the ankle joint is displaced to the posterior part of the talus resulting in a reduced articulating surface and an increased load onto the cartilaginous surface. In vitro studies have shown that rotationplasty results in a significant transfer of the loading zone onto the posterior part of the talus, a significant reduction in the contact area and a significant increase in mean and maximum weight pressures (Rosenbaum et al. 2003). However, in the presented study no painful degenerative changes were seen in the ten years after surgical treatment, although the physiological load-dependent changes did result in the formation of new bony structures. These changes did not result in clinical symptoms like an arthrotic deformity. This may due to the fact, that part of the induced body weight is transferred to the prosthetic shaft that encompasses the foot. This effect has been demonstrated with plantar and dorsal pressure measurements inside the prosthesis that revealed a marked load transfer to the foot from both aspects (Hillmann et al. 2000c; Rosenbaum et al. 2003). An altered topology and alignment of the trabecular structure was also observed, particularly in young patients with an ‘optimal’ plantar flexion in the ankle joint. These changes were less distinctive in older patients, highlighting the fact that, despite the decreased biological potential of their cartilage for adaptation, no arthrosis was observed in their ankles.
This may be explained by the fact that older patients have a restriction of daily live activities. Furthermore, these patients have a reduced range of motion, especially regarding the plantar flexion of the ankle joint, which causes a more physiological weight bearing because of a lesser pes equinus bearing. Consequently it is more challenging to achieve a cosmetically adequate exoprosthesis with these patients, because the inability of their joints to maximally hyper-extend thickens the exoprothesis. However, this has no functional consequences for using the prosthesis and the biomechanical changes after rotationplasty were less severe in older patients.
The present results suggest that the foot is able to adapt to the load changes from rotationplasty, and that this does not cause an inevitable arthrosis in the ankle joint. As no patients in this study complained of pain at least ten years postoperatively, we believe these observed changes to be as a result of physiological adaptation to the altered anatomy and biomechanics after rotationplasty.
Nevertheless, it is possible that degenerative changes will occur in the future. Further studies, with a longer follow-up and including older patients, are required to support these results.