
Abstract
Patients with diseases which impact on foot health, for example diabetes and rheumatoid arthritis, are known to have some benefit from prescribed stock footwear with regards to clinical outcomes. Achieving this is not just about getting the footwear designed and fitted to meet the clinical needs, but it also requires that the patient wears the shoes. This means meeting the non-clinical needs or criteria of patients. The aim of this study was to compare perceptions of the same footwear between patients with diabetes and patients with rheumatoid arthritis (RA) with regard to specific design features. Fifty-four patients with RA and 40 patients with diabetes who required prescription footwear were asked to identify issues of importance, and to assess the features of five different pairs of stock footwear using a Likert scale scoring form. There was a difference between the RA and the diabetes groups with regards their overall requirements from the footwear with comfort being a priority in RA and style a priority for diabetes. Both groups rated the same footwear as overall best from the selection, but the scores suggest that there were features with the ‘best’ shoe which were not acceptable suggesting that even the ‘best’ shoe was a compromise This possibly indicates that existing footwear ranges do not meet all the patients' requirements. Patients have different perceptions with regard to what is important to them in terms of footwear with regards to the specific features of the footwear and one of the influences appears to be the underlying systemic disease. Patient-based criteria may be an important consideration in the design of the footwear.
Introduction
There are several manufacturers of prescribed stock footwear who claim to meet the requirements demanded by clinicians in the care of patients whose foot status is regarded as being at risk of ulceration, infection, and gangrene. The clinical criteria for this footwear are primarily plantar pressure relief, reduced skin abrasion and foot and lower limb stability. The ultimate aim is to prevent the development of excessive pressure, since this is a precursor to the development of callus, tissue damage, and ulceration. Patients with diabetes, rheumatoid arthritis, connective tissue disorders, peripheral vascular disease and other conditions associated with compromised neurological status and poor tissue viability are known to have some benefit from prescribed stock footwear with regards to clinical outcomes (Chalmers et al. 2000; Striesow 1998; Donaghue et al. 1996; Uccioli et al. 1995; Michelson et al.1994; Chantelau et al. 1990).
Achieving the clinical benefits footwear is not just about getting the footwear designed and fitted to meet the clinical needs, but it also requires that the patient wears the shoes. This means meeting the non-clinical needs or criteria of patients. Reports have recommended that patients are involved more in the provision of footwear (Bowker et al. 1992; Disabled Living Foundation 1991) as footwear needs extend beyond the patients' clinical needs and the clinical rationale for their footwear. Footwear is intimately linked to body image and self-esteem, which themselves are linked to mood, levels of depression, well-being and quality of life. These issues may well impact differently on the patients supplied with this footwear due to the many variables which are presented with such as gender, age, disease, patients' previous experiences, perceptions and expectations.
Two of the main groups to which specialist footwear is supplied are patients with diabetes and rheumatoid arthritis (RA). These diseases differ in their impact on the individual patient in terms of body image, general well-being, mental health and quality of life. In rheumatoid arthritis, the deformity and pain has an impact on how the body physically looks, and can have a detrimental effect on many areas of life including moods, activities of daily living and the patients' perceptions about their body image. These issues are important in the well recognized effect of RA on quality of life (Whalley et al. 1997) and the elevated levels of depression in patients. The impact of foot pain not only affects mood but results in a visible sign that the patient is in pain. This links with body image not only because the feet physically look different, but also because the pain becomes ‘visible’ once it alters the way the patient walks. An early study by Minaker and Little (1973) demonstrated in 50 in-patients with RA that 88% had a characteristic shuffling gait and shortened stride. Thus foot pain, foot deformity, body image, well-being and patient quality are all intimately linked, and footwear has a clear role in influencing these issues. The non-clinical role of footwear is therefore potentially very important in RA.
In contrast, patients with diabetes do not suffer with disabling joint pain in the feet. The main problems associated with the diabetic foot are lack of sensation and in some, unsteadiness as a result of neuropathy. The visible signs of diabetes are less obvious and therefore body image is therefore affected less (Cavanagh et al. 1993). Mobility and depression are also less common issues than in RA. The objective of supplying footwear to patients with diabetes is to prevent occurrence or reoccurrence of foot ulceration. Patients with diabetes who have been prescribed specialist shoes often do not wear them, giving reasons such as being too big, and being unsightly (Ward 1993), suggesting they are more concerned with the visual appearance of the footwear rather than the functional and comfort aspects. By contrast, dissatisfaction with specialist footwear in patients with RA tends to be in the areas of poor fit, weight of the shoe and comfort problems (Stewart 1996), issues which are related to the functional aspects of the footwear. The non-clinical role of footwear is perhaps less important in diabetes than in RA.
Whilst the footwear currently provided can, in principle, adequately meet the clinical needs of patients, it must also meet the non-clinical needs of patients, and these differ between different patient groups and individual patients and are closely related to the nature of the disease, its consequences and its status. The fact that these non-clinical needs can be different between patients and different patient groups questions whether the footwear choices currently offered to various patient groups meets these differing needs. This is important because meeting these non-clinical needs will be critical to ensuring patients wear their footwear and subsequently in meeting their clinical needs. The evidence for high levels of non-compliance suggests that perhaps patients' needs are not being met otherwise they would be wearing the footwear supplied (Knowles and Boulton 1996; Lord and Lewis 1998).
Current stock footwear design has been developed through technological advancements, results of research and the requirements of the clinician. The clinician takes into account the requirements of individual patients and therefore the patient has had an indirect influence the evolution of the footwear available today. However, no previous study has formally and systematically explored in detail the requirements of a group of patients. It is recognized that in many orthotic/footwear services the choice available to patients is restricted by contracting arrangements which limit the clinical often to one footwear manufacturer. This is all the more reason to ensure that the footwear available from all manufacturers have been designed with some appreciation of patient requirements of footwear, and thus to investigate patient perceptions of footwear. The opinions of individual patients will of course differ but there may be distinct differences according to the impact of different diseases such as diabetes and RA. The current stock footwear design process is based on clinical need and clinical perspectives without, apparently, an understanding of patient expectation and perceptions of footwear. This study therefore aimed to explore perceptions of footwear in patients with diabetes and RA, compare footwear issues that are important to patients in these groups, and explore and compare their preferences for footwear using a range of currently available stock prescription footwear. The purpose in doing this was to gain insight into how patient expectations and perceptions might influence footwear design.
Method
Fifty-four patients with RA (20 men and 34 women), and 40 patients with diabetes (19 men and 21 women) were recruited from local health services (n = 6) in the North West of England and enrolled into the study, having given written consent to participate. All patients had been deemed ‘unable to fit into retail shoes’ and therefore required prescribed stock footwear by a referring orthotist or podiatrist.
A choice of five pairs of women's and five pairs of men's prescribed stock footwear were selected from the current market. All were suitable for actual use in the patient population that were recruited and were therefore a genuine reflection of shoes that might be offered through a clinical service to these patients. All the shoes were marketed for patients with diabetes but most were also used for patients with RA. To standardize the footwear the patients examined, the women's shoes were all size 5 and black, the men's were all size 8 and black (Figure 1). Black was chosen as the commonest colour chosen by patients in clinical practice and the authors wanted patients to focus on specific design features of the footwear rather than the colour.
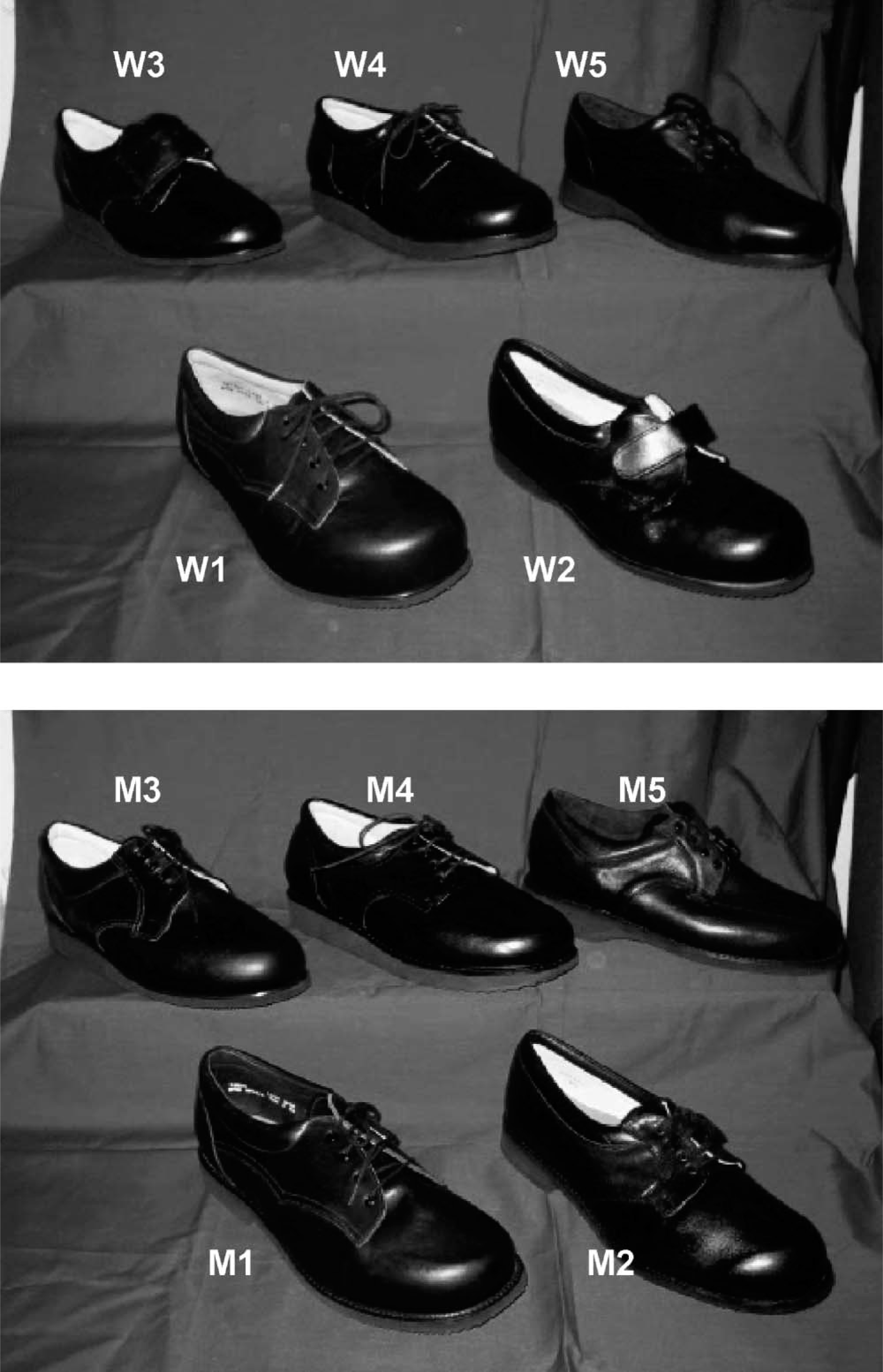
The women's (top) and men's (bottom) shoes used in the study.
The process for collecting data was the same for both the male and female groups. Patients examined shoes and were interviewed individually. Patients were shown five pairs of shoes which were arranged in a random order on a table (the arrangement of the shoes was changed between patients). The patients were prompted to examine each of the five pairs of shoes. Patients who only took a superficial interest in examining the shoes were prompted to examine in detail different aspects, such as the shoe upper, the sole, the tread and shape of the heel. Patients were allowed to ask general questions and discuss with the interviewer the shoes, but no opinions were given by the interviewer. After the interviewer was satisfied that the patient had paid sufficient attention to each pair of shoes (which typically took 4 – 5 min), the patient was seated away from the shoes for the interview. The interview had three parts.
Firstly, through open dialogue the patient was asked to highlight ‘the most important things with regard to your footwear’. The interviewer took brief notes of the main issues suggested by the patient and any comments related to these issues, identifying key words and associated phrases. These issues were reiterated to patients for confirmation.
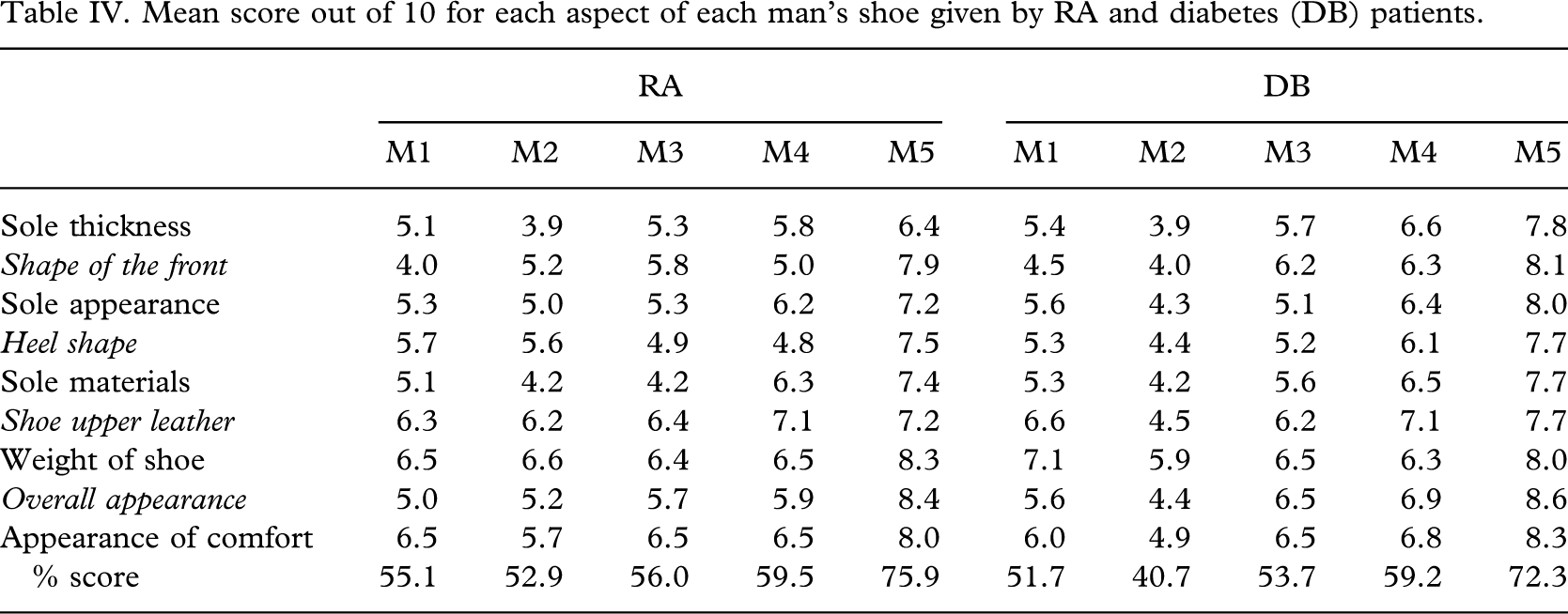
Secondly, patients were then asked to re-examine each pair of shoes (in a random order) and rate on a 10 cm visual analogue scale (zero = very poor, 10 = excellent) their opinions of 9 aspects of each of the five pairs of shoes. These aspects were: ‘sole thickness’, ‘shape of the front’, ‘sole appearance’ (two aspects: the peripheral aspects of the sole that are visible when the footwear is being worn and the plantar aspect that is visible when the footwear is removed and inspected), ‘heel shape’, ‘sole materials, ‘shoe upper leather’ (the quality of the leather used for the shoe upper), ‘weight of shoe’ (when the shoe is being inspected rather than when the patient wears the footwear), ‘overall appearance’ (how the footwear ‘looks’ to the patient when all its the features are taken into account), ‘overall comfort’ (refers to the appearance of comfort – the patients did not wear the footwear as the authors wished to evaluate the patients' perceptions of comfort).
If a patient perceives that the footwear ‘looks’ comfortable then this may be the factor which engages them to wear the footwear. In particular, for therapeutic footwear, patients may choose footwear from a catalogue or from an example shoe which they are not able to try if it is not the correct size. The authors were interested in what patients perceived to embody ‘comfort’.
Thirdly, the patient was allowed a few minutes to re-examine the five pairs of shoes and choose the best and worst pair of shoes. The shoe chosen as the ‘best’ was then placed in front of the patient, and they were asked what they liked the most about the shoe, and whether there was anything they disliked about the shoe. The same was completed for the shoe chosen as the ‘worst shoe’, identifying what was disliked the most, and any aspects of the shoe that the patient did like.
This whole process typically took 25 – 30 min. Throughout the examination of shoes, the interview, and the analysis of the data the researcher was blind as to which shoe related to any manufacturer, and all shoes were only identifiable by number (M1-5 (men's shoes), W1-5 (women's shoes)).
Content analysis was used to establish the issues that were most important to patients in terms of their footwear. For responses to the question ‘what are the most important things with regard to your footwear’, lists of keywords were created taking a maximum of five from any single patient and the frequency of use of each word recorded. To reduce data, and since they did not appear to be genuinely separate issues, some words were assumed to refer to the same issue. For example, ‘look’, ‘style’ and ‘appearance’ of the shoe were considered to be referring to the same issue, namely the cosmetic qualities of the shoe. Keywords were added to the list until 95% of all keywords given in the interviews were included. The 5% of keywords not included were only mentioned by one patient. This provided a list of the issues most commonly raised by patients with regard to their footwear and the frequency was used to rank the issues in terms of priority, a higher frequency indicating more patients raised the issue and thus it was deemed to be a higher priority. A separate list of issues and frequency table was produced containing only the first issue raised by each patient.
The score for the nine individual aspects of each shoe were added together and expressed as a percentage. The scores for each shoe were then averaged across the patients in each of the four patient groups (men with diabetes, women with diabetes, men with RA, and women with RA). This produced average scores for each shoe from each of the four patient groups.
Content analysis was also used when examining the responses to what aspects about the ‘best’ and the ‘worst’ shoe were most liked/disliked, producing a list of keywords and frequency table for each shoe when it was considered the ‘best shoe’, and a list for when each shoe was considered the ‘worst shoe’.
All data was separated into the four patient groups and comparisons made between the diabetes and rheumatoid arthritis groups for the men and women separately.
Results
Twenty males and 34 women with RA (mean age 63 years; age range 32 – 82), 19 males and 21 women with diabetes (mean age 55 years; age range 29 – 79) took part in the study. Twenty-one of the RA patients and 26 of the diabetes patients were wearing retail footwear and the remainder had previous experience of prescription footwear. Two women with RA and one male with diabetes could not comprehend and complete the visual analogue scale scoring. Two women with RA and one woman with diabetes did not like any of the shoes and could not choose best or worst, but did complete the visual analogue scales.
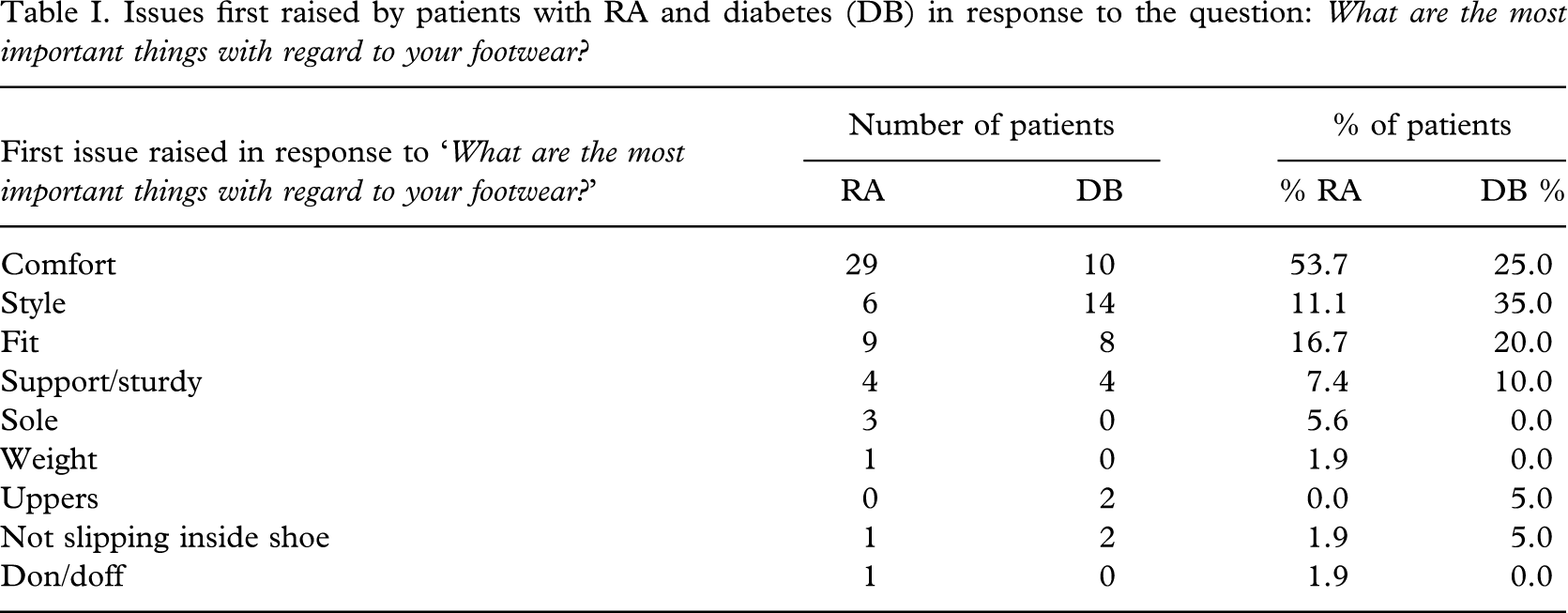
Table I lists the first issue raised by patients with RA and diabetes in response to the question ‘What are the most important things with regard to your footwear?’ and the number and percentage of patients giving each response. Table II lists 95% of all the issues raised in response to the question ‘What are the most important things with regard to your footwear?’ and the number and percentage of patients who had RA and diabetes giving each response.
Issues first raised by patients with RA and diabetes (DB) in response to the question: What are the most important things with regard to your footwear?
Details 95% of all the issues raised by patients with RA and diabetes (DB) in response to the question: ‘What are the most important things with regard to your footwear?’

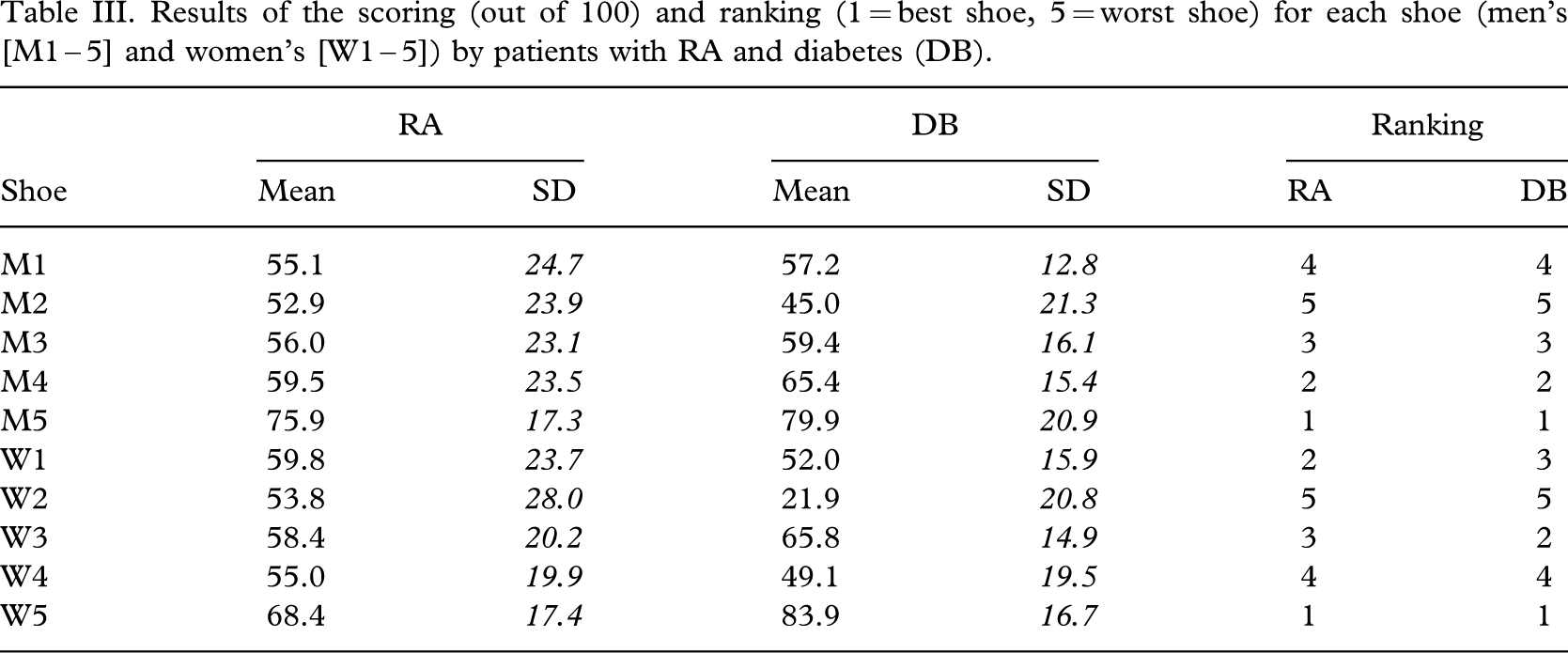
The percentage score given by the four patient groups to the footwear (M1-5, W1-5) through the visual analogue scales scoring of nine aspects of each shoe are detailed in Table III.
Results of the scoring (out of 100) and ranking (1 = best shoe, 5 = worst shoe) for each shoe (men's [M1 – 5] and women's [W1 – 5]) by patients with RA and diabetes (DB).
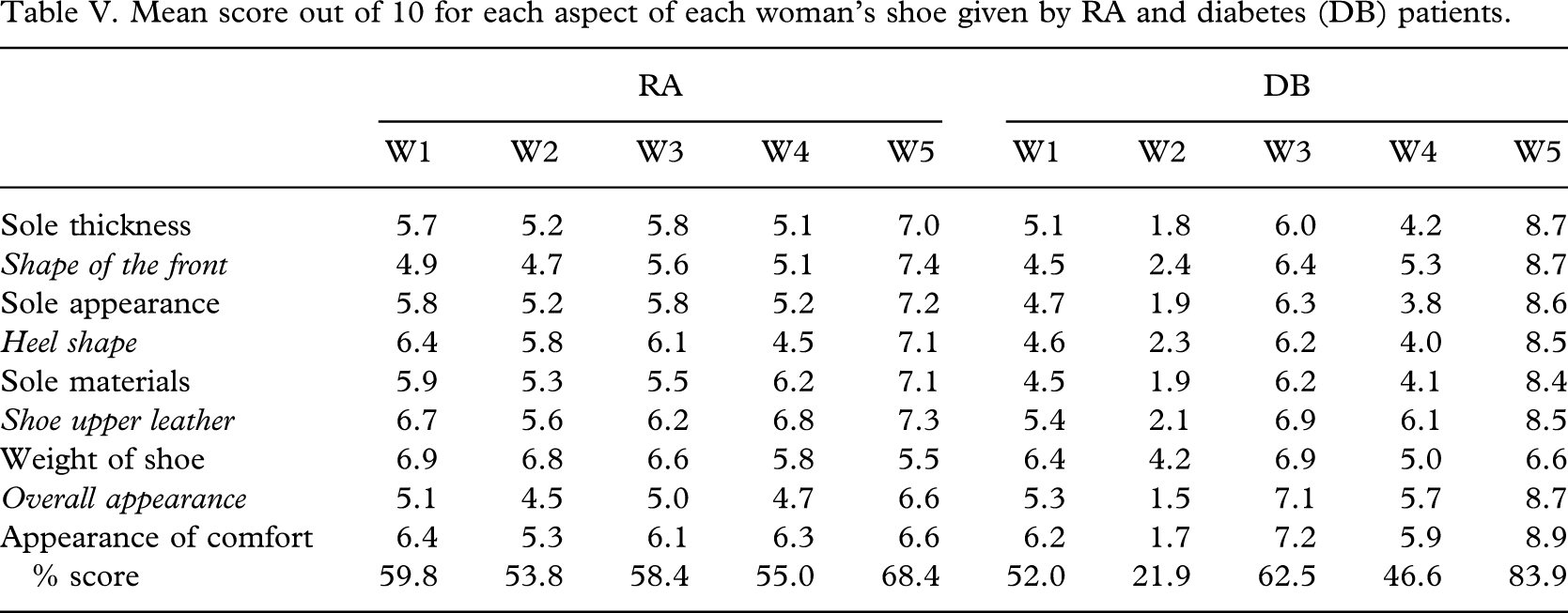
The mean scores given for each of the nine aspects of each of the RA and diabetes groups are detailed in Tables IV and V for men and women respectively.
Mean score out of 10 for each aspect of each man's shoe given by RA and diabetes (DB) patients.
Mean score out of 10 for each aspect of each woman's shoe given by RA and diabetes (DB) patients.
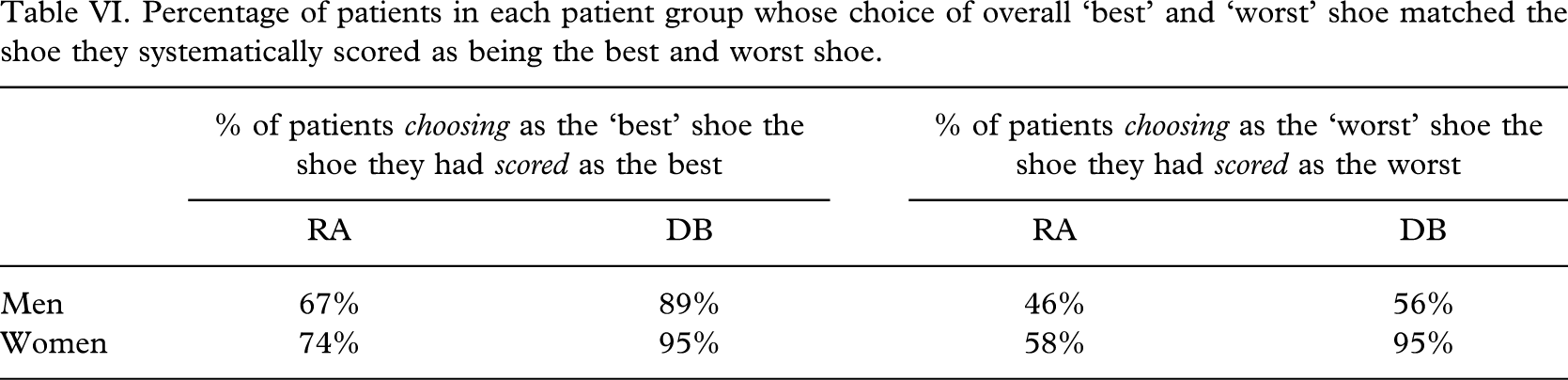
The visual analogue scale scoring of the shoes was completed prior to the patients having chosen a ‘best’ and ‘worst’. The shoe which was rated as the ‘best’ and ‘worst’ by each patient according to the scores derived from the visual analogue scales was compared to the shoe chosen as the ‘best’ and ‘worst’ when patients were asked to choose (Table VI).
Percentage of patients in each patient group whose choice of overall ‘best’ and ‘worst’ shoe matched the shoe they systematically scored as being the best and worst shoe.
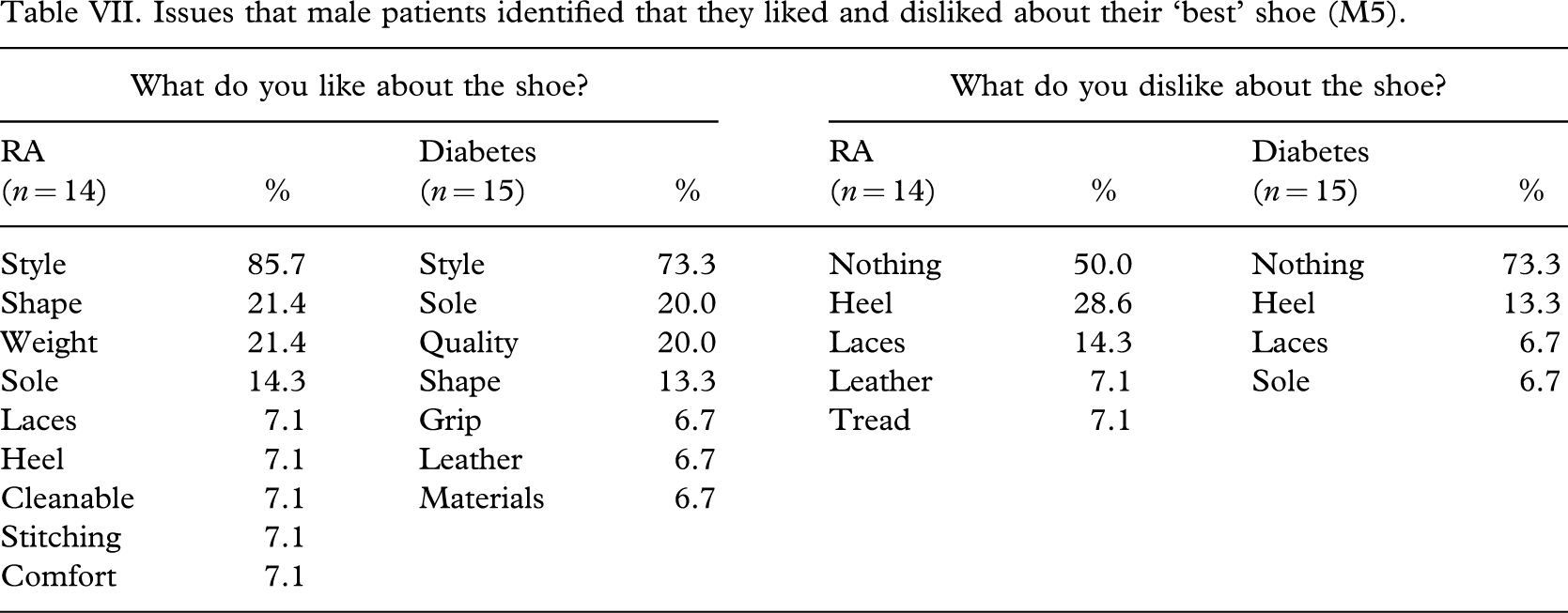
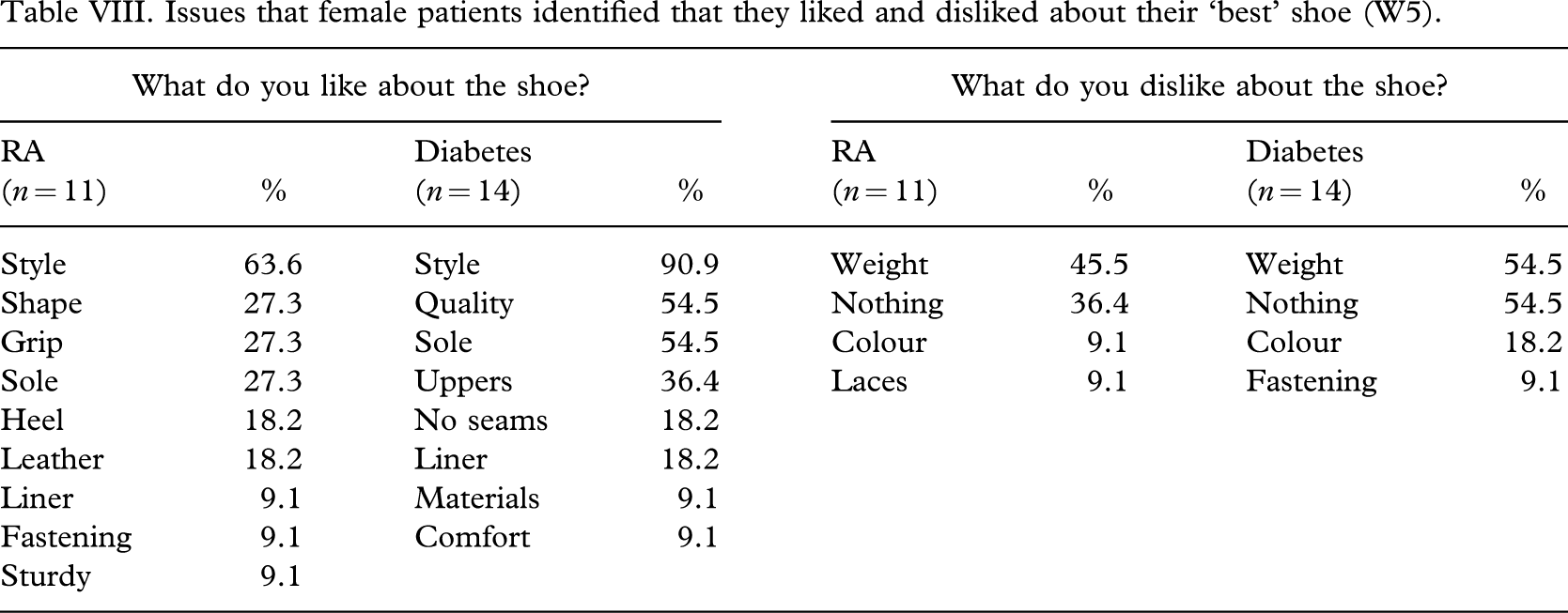
The breakdown of what patients liked and disliked about the favourite men's and favourite women's shoes (M5 and W5) are detailed for each patient group in Tables VII and VIII.
Issues that male patients identified that they liked and disliked about their ‘best’ shoe (M5).
Issues that female patients identified that they liked and disliked about their ‘best’ shoe (W5).
Discussion
Whilst the authors did not explicitly ask patients to rank in order of importance the issues raised with regard to their footwear, it was assumed that the first response given would be that of greatest importance to the patients. In this respect there was a stark difference between patients with RA and diabetes, with ‘comfort’ a priority for patients with RA and ‘style’ a priority for patients with diabetes. Responses from patients with diabetes suggested that they do not focus in the first instance on practical issues, such as fit or comfort, which in reality relate closely to their clinical need, but are focusing on the more common and ‘lay’ issue of footwear cosmesis. Not focusing on practical aspects of the footwear may in part be due to the fact that in diabetes normal foot structure is broadly maintained and more easily accommodated in retail footwear. Also, any failure in sensory function in the foot due to diabetes would reduce a patient's ability to sense poorly fitted shoes, and in fact all shoes may feel relatively comfortable. This being the case, their attention would justifiably be elsewhere, namely on the style/look of the shoe. In contrast, for those with RA, practical issues such as fit and appearance of comfort are more likely to be of more importance since they are likely to have greater difficulty due to the foot deformities and pain associated with RA.
In the analysis of the issues raised by patients in addition to those issues raised first, further but small differences between RA and diabetes groups exist. Shoe fastenings and weight were mentioned more often by patients with RA than those with diabetes. Fastenings are likely to be important for patients with RA since the hand function is also commonly affected, as is their general mobility. The fact that lighter weight shoes and heel height (low heels) were highlighted by the patients with RA and not diabetes might also reflect the fact that mobility is generally a greater issue for those with RA than with diabetes. Only two patients mentioned outcomes due to the footwear (improvements in walking, and reduction in pain), and both were patients with RA.
For the men with RA there was a clear distinction between the best shoe, M5, and shoes M1 – M4, with the difference in score between the first and second shoe (75.9% compared to 59.5%, difference of 16.4%) being greater than the difference between the shoes ranked second and fifth (52.9 – 59.5%, difference of just 6.6%). For the men with diabetes, there was much wider dispersion of scores for the shoes ranked second to fifth (45.0 – 65.4%, difference of 20.4%). The same was also the case for the ranking of the women's shoes in the RA and diabetes groups. Scores suggest that the patients with RA were less able to distinguish between the shoes ranked second to fifth when compared to patients with diabetes. It might be that the patients with RA did not consider any of these shoes as realistic options for themselves, and therefore branded them together collectively as failures, and then the difference between individual shoes may be lost since they are seen as a collective. Also, patients with RA prioritized ‘comfort’ as the main issue for their footwear and this is perhaps a difficult issue for them to gauge visually and thus difficult for them to distinguish between the appearances of comfort levels of different shoes. Nevertheless, the appearance of comfort is an important issue for this group and reflects the impact of the disease on the patient with the ‘look’ of comfort being the factor in engaging the patient in the use (or choosing) of the footwear in the first place. In contrast, the principal issue for patients with diabetes was style, and patients are likely to have a clear picture of what they expect, and therefore are more able to rank shoes at least in respect of this issue.
Ideally, when the patient was asked to choose what they considered to be their overall choice of best and worst shoes, all would have chosen the shoes they had previously scored as being the best and worst shoes indicating that patients may not have been clear as to which was the best or worst, or were in fact changing their mind during the process. Certainly, in some instances, the failure to match the scored and chosen best/worst shoes was a product of the fact that some patients scored shoes very closely, and thus the difference between the shoe ranked first or second based on the scoring might only have been a few percent. Subsequent questioning by the researcher and being asked to choose one shoe as the best and worst may have falsely contrived a rank order of the shoes to the patient, when in fact they may not have perceived a tangible rank order. In hindsight the authors should have allowed patients who had difficulty in choosing a best or worst shoe to state more than one shoe. Finally, the systematic breakdown of the shoe qualities into nine different aspects is quite foreign compared to the relatively ‘face value’ assessment of shoes undertaken by most people in a retail or typical clinical setting. This approach may in fact have been overly systematic and failed to correctly capture the ‘instinct’ that is used when choosing shoes. Implicit in this, however, is the assumption that the face value assessment of the patient's footwear choice is the gold standard, which it may not be. A more systematic approach to choosing footwear in clinical practice might improve outcomes since it would force patients to consider their footwear options in more depth and also their footwear needs. More informed choices would hopefully lead to better choices and hence improved outcomes.
The responses to the question ‘what are the most important things with regard to your footwear?’ have illustrated some differences between patients with RA and diabetes with regard to their perception of their footwear needs and what good footwear is. In contrast, the scoring of the different shoes on offer using visual analogue scales offers some insight into whether these differences between patient groups were put into practice when evaluating and choosing footwear. The fact that for both the men and women, and despite having different footwear priorities, the RA and diabetes group rated the same footwear (M5 and W5) as the best suggests that either these shoes met the different criteria of both groups or that the differences in perceptions of what is important in terms of footwear to the two groups were not implemented when choosing footwear. In the latter instance, the choice of footwear offered in the study might have been so narrow that the criteria for ‘ideal footwear’ for one or both groups could not be met by any of the five shoes, and some compromise by either or both groups led to both choose the same footwear as the best. Regardless, there is clear evidence within the results that patients were compromising on their choice of footwear, even with those shoes chosen as the best. For example, with the shoes chosen as the ‘best’ shoes (M5 and W5) there were compromises (Table VI and VII). For the women with RA, 45% stated that they disliked the weight of the ‘best’ shoe. For the men with RA, 50% stated there was nothing they disliked with the shoes, which means that 50% did identify something they disliked, and one assumes that wearing the shoes would therefore be a compromise. A small number of patients did not compromise and instead stated that they could not choose a ‘best’ or ‘worst’ shoe because all shoes were ‘awful’ or ‘unsuitable’. Perhaps then patients are compromising on their footwear needs because the choice of shoes does not match their needs, or their perception of their need. If patients are having to compromise on their choice of footwear, it is possible that the compromise is too great and one outcome of this would be low levels of usage of the footwear, which is known to be problem (Knowles and Boulton 1996; Stewart 1996). The problem still exists that achieving the desired health benefits from prescribed footwear is a case of meeting both clinical and patient criteria. The results and the compromises made by patients in the study are indicative of existing footwear not meeting the patients' criteria totally, and this is likely to have a negative impact on patient engagement with the use of this footwear and ultimately clinical outcomes. Patient involvement in the design process may well help, but better patient awareness and understanding of their foot and footwear needs would also be advantageous. These factors in conjunction with more patient choice and offered options during the consultation process and more time allocated for patient assessment and the establishment of a positive ‘therapeutic relationship’.
Summary
Patients have different perceptions with regard to what is important to them in terms of footwear requirements. This study has demonstrated that some of these differences are because of the influence and impact of diseases such as RA and diabetes and gender. This is in addition to the other factors such as age, previous experiences of footwear, influence of the therapeutic ‘patient/practitioner’ relationship and service structure but these were not explored in this study. Previous studies and reports (Bowker et al. 1992; Disabled Living Foundation 1991) have identified that the attempt to provide a patient-centred service is restricted by the service contracts in many NHS orthotic services and the benefits of the service being delivered in a multiprofessional setting have been demonstrated (Williams and Meacher 2001; Baker and Leatherdale 2002). Achieving the desired health benefits of prescribed footwear requires that clinical criteria are met through good footwear design and prescription; however, it also requires that a patient wears the shoes. To ensure this, the patients' footwear criteria must be met, which appears to be different for the patients with diabetes and those with RA. The authors would suggest that insufficient attention has been paid to addressing patient perceptions of footwear in footwear design, patient education, the therapeutic relationship and footwear service delivery in respect of clinician time.
Involvement of patients in the design process and specific diseases being taken into account during this process ensures that a patient-centred approach is evident throughout the whole process of specialist footwear provision. The National Health Service in the UK generally is supporting the involvement of stakeholders in the delivery of effective healthcare and benefits of this consultation are expected. Consultation with patients at the design stage may contribute to the development of footwear designs which enable clinicians to provide patients with what they need to maximise their potential foot health benefits.