
Abstract
This is the first study to report on hip range of motion (ROM) among active prosthesis users, when wearing and not wearing a trans-femoral socket prosthesis and to compare with individuals rehabilitated with an osseointegrated bone-anchored prosthesis. In addition, discomfort when sitting with the prosthesis is reported in both groups. The study group all had a non-vascular amputation and were divided into those supplied with a socket prosthesis (S group) (n = 43, mean age 51 years, 74% men) or a bone-anchored prosthesis (OI group) (n = 20, mean age 46 years, 75% men). Active hip ROM was measured with a goniometer, and self-reported problems with discomfort when sitting were recorded. The hip motion decreased in all directions when wearing the socket prosthesis compared to without it (P < 0.001 for all directions), and 37% of the subjects had less than 90° of hip flexion when wearing their prosthesis. Discomfort when sitting was reported among 44% (n = 19) in the S group and was more common among individuals with less than 90° of hip flexion motion (P = 0.025). In the OI group, no restriction in hip motion was measured with the prosthesis, and no subject had less than 90° of flexion and 5% (n = 1) reported discomfort when sitting. This study shows that a trans-femoral prosthetic socket significantly reduces the ROM of the hip and that discomfort when sitting is common among individuals wearing such prostheses. Further, the study confirms that individuals using a bone-anchored prosthesis have no restricted hip motion with the prosthesis and report very few problems with discomfort when sitting.
Introduction
Adequate hip joint motion is needed to perform the activities of daily living. Johnston and Smidt (1970) reported on the pattern of hip motion needed for selected activities of daily living in normal subjects. They concluded that a successful result of hip surgery ‘should provide motion of at least 120° flexion, 20° abduction and 20° external rotation, so that common activities of daily living can be performed normally’. Further, a full range of hip extension is a prerequisite for gait with a normal stride length (Perry 1992).
A trans-femoral amputation influences the balance and strength of the muscles around the affected hip joint (Gottschalk 1999; Jaegers et al. 1995). Together with immobility and pain following the amputation, insufficient muscle strength increases the risk of muscle contractures (Gailey and Clark 2004). The risk of a contracture is greatest in hip flexion, but in the case of a shorter stump a contracture in abduction and external rotation could also be developed. If a contracture is present, this will prevent the proper alignment of the prosthesis as well as reducing the torque by involved muscles groups (Murnaghan and Bowker 2004) with decreased walking capacity as a result.
The conventional way to provide a connection between the stump and the prosthesis is by a socket. At the trans-femoral amputation level, the socket contains the total stump to the groin. There are two main socket designs used in the last decades: the quadrilateral socket (QL) and the ischial containment socket (IC) (Kapp 2000; Schuch and Pritham 1999). The most important differences between these sockets are the contours of the proximal brim in which the ischium is outside the QL socket and contained in the IC socket. There is a focus on antero-posterior pressure in the first, compared with a more medio-lateral pressure in the latter. Another feature of a socket is the material used. This could be rigid or flexible. Schuch and Pritham (1999) have declared that the basic goals for the fitting of a trans-femoral prosthesis are ‘comfort, function, stability and cosmesis’. The authors emphasize the importance of an evaluation of the range of motion (ROM) of the stump to be able to make proper alignment of the prosthesis.
Discomfort due to the prosthetic socket has been reported in several studies (Dillingham et al. 2001; Hoaglund et al. 1983; Pezzin et al. 2000). Legro et al. (1999) reported on prosthesis-related issues of importance identified by persons using a lower-limb prosthesis and found that comfort with the prosthesis while standing and sitting is of great importance. Clinical experience indicates that some patients make complaints about restricted hip motion, due to the socket, when wearing their prosthetic limb. Hachisuka and co-workers compared the self-reported comfort of the socket between patients supplied with a QL socket and an IC socket, and concluded that the latter was more comfortable (Hachisuka et al. 1999).
A new way to attach a prosthetic limb is by using the method of osseointegration (Branemark et al. 2001; Robinson et al. 2004; Sullivan et al. 2003). In this method, the prosthesis is attached directly to the bone, via a titanium fixture, inserted to the bone and connected to an abutment which penetrates the skin. This means that suspension of the artificial limb is provided without any socket. During rehabilitation of the first patients provided with a bone-anchored trans-femoral prosthesis, the authors noticed that the patients regained their range of motion in the hip joint when wearing the prosthesis. Further, problems with uncomfortable sitting seemed to decrease markedly when wearing the prosthesis.
To learn more about restriction of hip ROM among persons with a trans-femoral amputation, a literature search was conducted. However, no study was found describing measurements of hip ROM among established prosthesis users while wearing or not wearing their prosthesis. The aim of this study was threefold: (1) to study hip joint motion, when wearing and not wearing a trans-femoral socket prosthesis; (2) to study the phenomena of uncomfortable sitting when using the prosthetic limb; and (3) to compare the results with individuals provided with a bone-anchored trans-femoral prosthesis.
Method
Material
Inclusion criteria in the study were: to have a unilateral trans-femoral amputation, for at least 2 years, for reasons other than vascular disease; to be between 20 and 70 years old; and to be a prosthetic user, with the ability to walk continuously for at least 100 m. Persons using a socket prosthesis (S group) were recruited from all four prosthetic workshops in the Swedish county of Västra Götaland. This sample was contacted to participate in a mailed study of measurement properties by means of a targeted questionnaire (Hagberg et al. 2004), and those willing to participate in that study were also asked to take part in the current study. To be included, individuals were required to have a sufficient ability to read and understand the Swedish language. Persons using a bone-anchored (osseointegrated) prosthesis (OI group) were included if they fulfilled the same inclusion criteria and had had their surgery performed before March 1999 in Sweden or the UK. All assessments in the OI group were made at a regular follow-up visit to the Department for Prosthetics and Orthotics, Sahlgren University Hospital, Göteborg or to Roehampton Rehabilitation Centre, Queen Mary's Hospital, London, UK. The study was approved by the Ethics Committee at the Sahlgrenska Academy, Göteborg University, Sweden.
Measurements
Self-reported demographic data were collected, including the year and cause of amputation, weight (without wearing the prosthesis) and height. Calculation of body mass index (BMI) was approximated by adding 12% of the individual body weight in the formula to compensate for the loss of the limb (Winter 2004). A prosthetist collected data about the prosthesis, length of the stump, and the contralateral limb. Limb length was measured in centimetres from the ischial tuberosity to the end of the amputated femur, with soft tissues, and to the medial knee joint space, respectively.
Active hip range of motion was measured bilaterally and recorded according to the AAOS method (AAOS 1965). The affected limb was first measured when wearing the prosthesis and then without wearing it. One trained physiotherapist from Sweden and one from UK performed all measurements using the same standardized protocol. All measurements were performed on a firm treatment table. A goniometer with long lever arms was used and aligned as described by Norkin and White (2003). Measurement to the nearest 5° was recorded. Hip flexion, extension, abduction, and adduction were measured with the participant in the supine position. Hip flexion was measured with the examined knee flexed and the contralateral limb extended on the table. For extension, the participant was positioned diagonally on the edge of the table with the examined limb placed over the edge and asked to hold a firm grip around the flexed contralateral knee to minimize lordosis of the spine, i.e. in the Thomas Test position. Abduction and adduction were measured with the knee extended and with instructions not to lift or rotate the limb when performing the motion. For adduction, the contralateral leg was positioned in some hip and knee flexion to allow full motion. When those measurements were performed when wearing the prosthesis, a helper was sometimes needed to give light support under the prosthetic heel. Rotation was measured with the individual seated and with the whole femur supported by the table. Rotation was not measured when not wearing the prosthesis. Before starting the examination in the S group, the participants were asked if there was any risk of loosening the suspension of the prosthesis when performing certain movements. If so, the particular movement was performed last, before taking off the prosthesis.
Questions concerning normal prosthetic use and uncomfortable sitting were taken from the Questionnaire for persons with a trans-femoral amputation (Q-TFA). Q-TFA is a targeted self-report questionnaire which has been shown to have adequate measurement properties (Hagberg et al. 2004). For sitting comfort, the individual was asked to answer the amount of trouble perceived in sitting when wearing the prosthesis during the last 4 weeks. Answers were given on a five-degree Likert scale (0 = no trouble, 1 = slight trouble, 2 = moderate trouble, 3 = considerable trouble, 4 = a great deal of trouble). Those cases who reported ‘moderate trouble’ to ‘a great deal of trouble’ with uncomfortable sitting (2 – 4) were grouped together to represent discomfort with sitting compared with those reported ‘no trouble’ or ‘slight trouble’ (0 – 1 = no discomfort with sitting). Further, the results were split into those cases having less than 90° of hip flexion ( = restricted hip flexion) and those having 90° or more motion in flexion ( = no restricted hip flexion) when wearing the prosthesis.
Statistical methods
Comparisons between variables of the S group and OI group were performed with the Mann – Whitney U-test for continuous variables and Fisher's exact test for dichotomous variables. According to between-group differences, analyses of logistic regression were performed to adjust for differences in motion when not wearing the prosthesis between the two groups. When comparing the groups, all tests were two-tailed and conducted at a 1% significance level to allow for type 1 errors.
Within the S group, hypothesis testing between the subgroups (category discomfort with sitting 2 – 4 versus 0 – 1 and category hip flexion < 90° versus 90°) was performed with the Chi-square test. Logistic regression was performed to analyse variables connected with discomfort with sitting when wearing the prosthesis. A forward stepwise method was used. Variables with a univariate P-value < 0.1 were included in the model as possible predictors (Table I).
Demographic data of the S group and OI group, and analyses of differences between the groupsa.
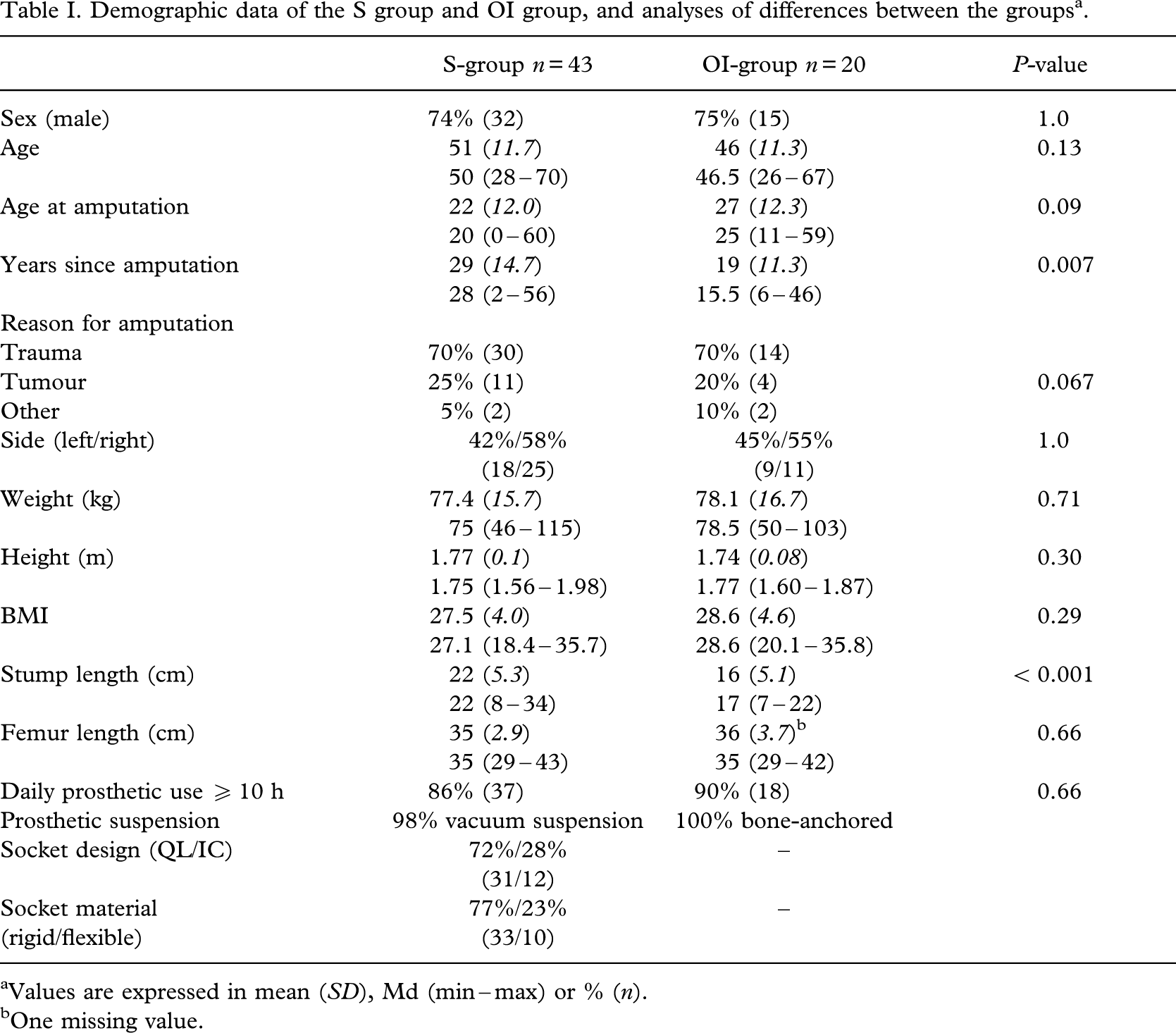
Values are expressed in mean (SD), Md (min – max) or % (n).
One missing value.
Results
In the S group 70 persons were identified as potential participators fulfilling the inclusion criteria. Three cases were not reached, and 23 did not want to participate in the current study. One case had to be excluded due to multiple fractures of the pelvis at the time of the amputation still causing limited hip motion. The S group consisted of 43 persons. The OI group consisted of 20 persons, of whom three cases were followed in UK and all others in Sweden. The median follow-up time since receiving the bone-anchored prosthesis was 5 years (range 3 – 10). Demographic data of each group are presented inTable I. The mean time since the amputation was longer in the S group than in the OI group (29 versus 19 years, P = 0.007) as well as the mean stump length (22 versus 16 cm, P < 0.001). No other demographic variable differed between the groups.
Hip range of motion
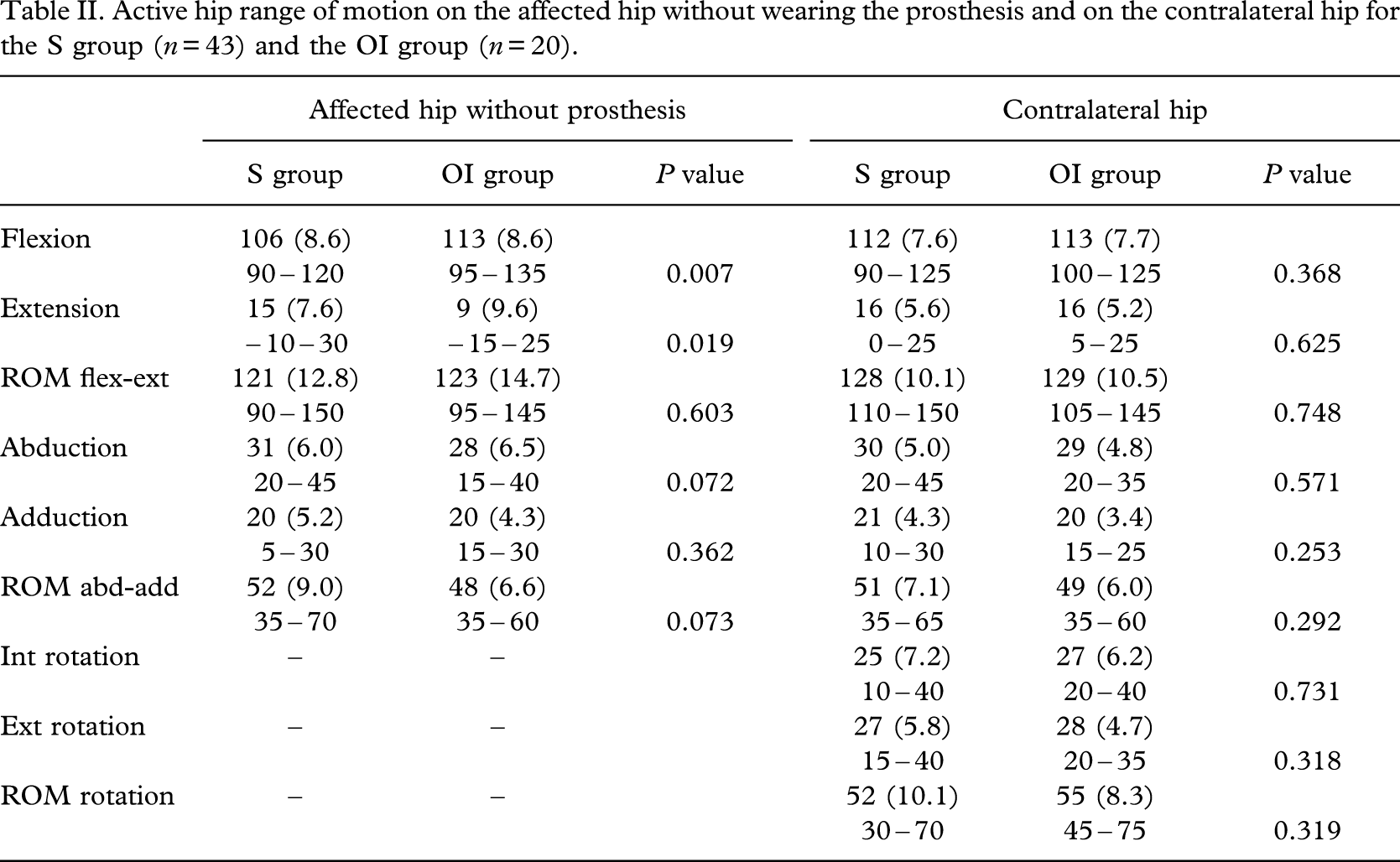
Measurements of active motion on the affected hip when not wearing the prosthesis as well as the contralateral hip are presented inTable II. The S group had less motion, on the affected side, in hip flexion (mean difference 7°, P = 0.007) and larger motion in extension (mean difference 5°, P = 0.019) than the OI group. There were no differences in motion on the contralateral hip between the groups.
Active hip range of motion on the affected hip without wearing the prosthesis and on the contralateral hip for the s group (n = 43) and the OI group (n = 20).
Hip motion on the affected hip with the prosthesis and figures of the difference in motion compared with when not wearing it, for each group, is shown inTable III. In the S group, mean hip motion when wearing the prosthesis was decreased in all measured directions (P < 0.001 for all motions) with the greatest single difference shown in hip flexion (mean difference − 15°) and ROM flexion-extension (mean difference − 24°). Analyses of differences of every separate motion within each case showed that 86% (n = 37) in the S group had at least 10° decreased motion in flexion, 56% (n = 24) in extension, 23% (n = 10) in abduction and 16% (n = 7) in adduction in the ipsilateral hip joint when wearing the prosthesis. The total ROM in flexion-extension in use with the prosthesis was decreased 20° or more in 63% (27/43) of the sample. Some 37% (16/43) of the S group had less than 90° of hip flexion motion when wearing their socket prosthesis.
Comparisons within groups and between groups regarding hip motion when wearing and not wearing the prosthesisa.
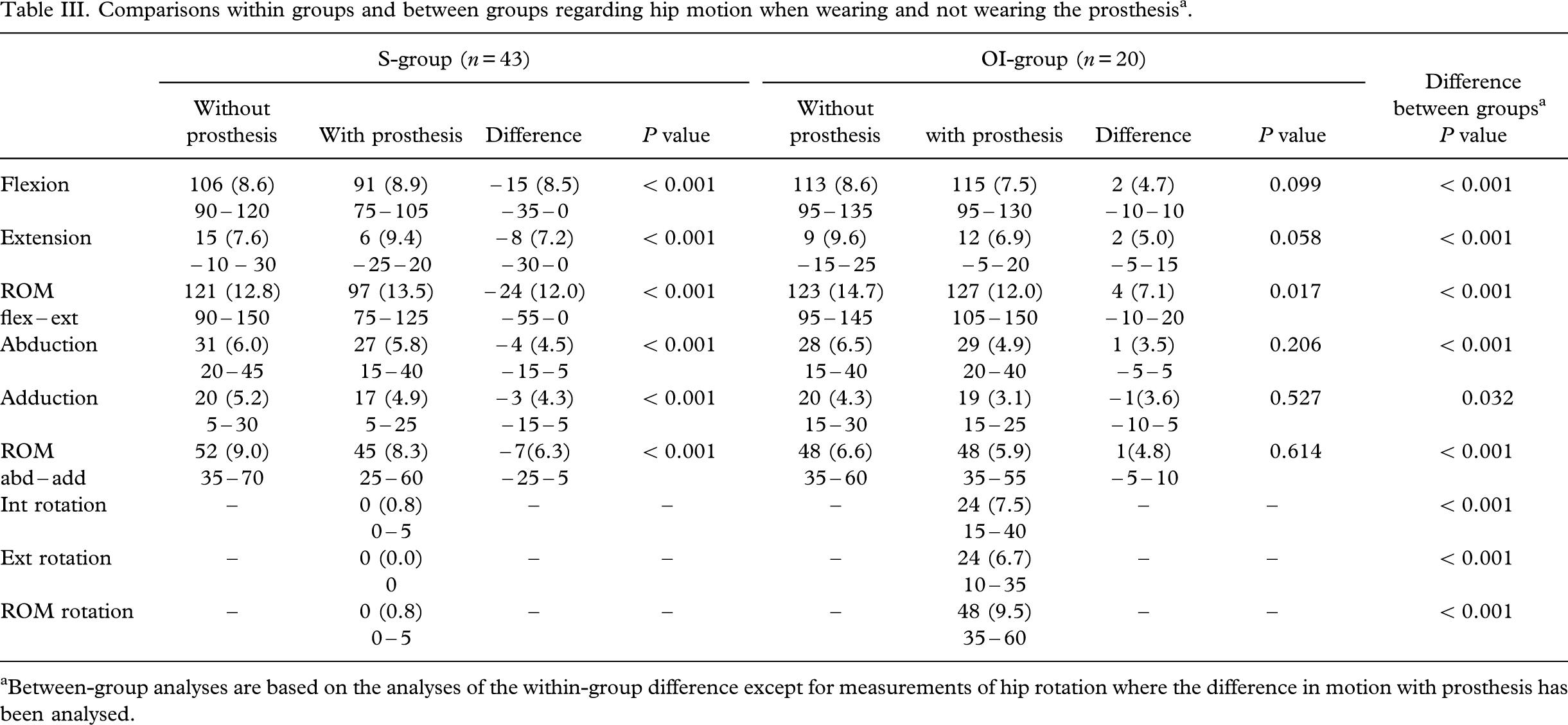
Between-group analyses are based on the analyses of the within-group difference except for measurements of hip rotation where the difference in motion with prosthesis has been analysed.
Within the OI group, the ROM in flexion extension was increased compared with when not wearing the prosthesis (4°, P = 0.017). No case in the OI group had less than 90° of hip flexion motion when wearing the prosthesis.
Analyses of between group differences showed that the OI group had statistically significant larger hip motion in all movements in use with the prosthesis compared with the S group (Table III), and the differences lasted even when adjusting for baseline differences in motion when not wearing the prosthesis (difference in flexion P < 0.001, difference in extension P = 0.002).
Sitting comfort
Discomfort when sitting, i.e. moderate to a great deal of trouble when sitting wearing the prosthesis, during the last 4 weeks was reported among 44% (19/43) of the cases in the S group and 5% (1/20) in the OI group.
Within the S group, discomfort when sitting was reported among 69% (11/16) of the participants that had less than 90° of hip flexion motion compared with 30% (8/27) of those having an active motion of 90° or more (P = 0.025). Discomfort when sitting was not reported more often among those having a QL-socket than those with an IC-socket (P = 1.0) or a flexible socket material compared with a rigid socket (P = 0.7). Logistic regression showed that the risk for discomfort when sitting with the socket prosthesis increased more than six times if the individual had less than 90° of hip flexion motion in use with the prosthesis (odds ratio 6.59, P = 0.014, CI 1.48 – 29.60), and the risk increased almost seven times for male compared with female cases (odds ratio 6.90, P = 0.044, CI 45.45 − 1.05). Variables included in the stepwise regression as possible predictors (with P < 0.1) were sex, stump length, degree of hip flexion without wearing the prosthesis, degree of hip flexion when wearing the prosthesis, and category of hip flexion when wearing the prosthesis ( < 90° / 90°).
Discussion
The results from this study show that a conventional trans-femoral socket prosthesis reduces the active hip range of motion among established prosthetic users. Further, the results confirm the clinical experience that restricted motion in hip flexion with the prosthesis increases the risk of discomfort when sitting; that individuals supplied with a bone-anchored prosthesis have no restricted hip joint motion in the affected limb in use with the prosthesis; and that this group report very few problems with discomfort when sitting with the prosthesis.
For this study, the authors' intention was to examine hip ROM among active prosthetic users to reduce the risk of measuring restricted motion due to immobility. Thus, all cases with an amputation due to vascular disease or a bilateral lower limb amputation were excluded. In addition, all should be able to walk continuously for at least 100 m to ensure that they also were active prosthetic walkers. In the S group, 43 of those 70 identified to fulfil the inclusion criteria were investigated. Treatment of amputation patients according to the osseointegration principle has now been performed for more than 14 years in Sweden, but the number of patients treated is still limited. The OI cases included in this study are all cases that fulfilled the inclusion criteria and who had their surgery performed before March 1999. This date was set due to the start of a prospective study on patients treated with osseointegration on the trans-femoral amputation level and from which results of change in hip ROM will be presented in the future. Although the number of participants in the OI group (n = 20) is less than half of the number in the S group (n = 43), the majority of the demographic variables showed similarity. Thus, comparisons between the groups according to the study protocol could be made. The difference in mean years since the amputation (29 and 19 years, respectively) should be noted, however. The difference in stump length confirms that the osseointegration procedure has been performed mainly on cases with a high-level amputation. From the clinical perspective, a shorter stump length is expected to result in less motion, and from this perspective the OI group had a somewhat poorer baseline condition.
To minimize the measurement error in examination of joint motion, recommendations have been made to use a standardized protocol and to have one trained staff member performing all the measurements (Lea and Gerhardt 1995). The authors used a standardized protocol but had two trained physiotherapists performing the measurements, one in Sweden and one in UK. Since all individuals in the S group and 17 of 20 in the OI group were investigated in Sweden, most of the measurements were performed by the same investigator (KH). The protocol used in the current study was adapted to the specific group of individuals using a prosthesis and differs somewhat from other studies. Measures on joint motion could be on a passive or active motion (Boone and Azen 1979; Ekstrand et al. 1982; Lea and Gerhardt 1995; Roaas and Andersson 1982; Roach and Miles 1991). The authors' choice to measure active motion was taken since the force of a passive motion could possibly hurt the individual by the pressure from the brim of the socket as well as causing loosening of the suspension of the socket. Moreover, hip extension was measured in a supine position instead of a prone position, which has been reported in most studies (AAOS 1965; Roaas and Andersson 1982; Roach and Miles 1991); lying prone when wearing a trans-femoral prosthesis and performing an active extension in that position could not be considered as either clinically relevant or comfortable. The supine position has however also been reported earlier and is recommended when a hip-flexion contracture could be assumed (Ekstrand et al. 1982; Greene and Heckman 1994). In the author's protocol, rotations were measured in the seated position, which has also been recommended previously (Hollman et al. 2003; Norkin and White 2003). No measurements of rotation were performed when not wearing the prosthesis, since there are no useful reference points on the stump.
In this study, the range of motion was assessed on the affected side with and without wearing a prosthesis. Though all movements when wearing the prosthesis were performed first, to avoid loosening of the suspension of the socket, this happened in a few cases in the S group, and the prosthesis had to be put on correctly again. Measurements of the contralateral or the sound limb were performed for descriptive purposes and comparisons with the motion of the sound limb with the affected side have been shown to be adequate (Boone and Azen 1979; Roaas and Andersson 1982).
The measurement error for joint motion, reported in the literature, varies between the different movements measured and the position of the subject (Bierma-Zeinstra et al. 1998; Boone et al. 1978; Ekstrand et al. 1982). Boone et al. (1978) reported an average measurement error of 3.7° and concluded that individual variation in active lower limb motion should exceed 4° when the same tester measures the same movement and 6° when more than one tester measures the same movement, to claim a real difference. The authors recorded measurements to the nearest 5° in concordance with earlier studies (Roaas and Andersson 1982; Roach and Miles 1991). This rounding up is commonly performed in clinical practice, but might lead to an increase in the measurement error. For this reason, the authors choose not to report intra-individual differences in a specific motion of less than 10°. Another risk of error in the current study is that the position of the prosthetic knee could differ somewhat from the human knee, due to the alignment of the socket, resulting in inaccuracy of the measurement. One limitation of the current study is subsequently the lack of test – retest reliability measures performed on individuals wearing a transfemoral prosthesis. When comparing the present results of hip motion measurements with those reported for healthy individuals or individuals with other disabilities, one must bear in mind which positions have been used and if an active or passive motion has been recorded.
Overall, the findings from this study demonstrate that the S group, with the prosthesis, had less hip flexion motion of the affected limb than the OI group. They also had reduced motion compared with that of healthy persons reported elsewhere in the literature (AAOS 1965; Boone and Azen 1979; Roaas and Andersson 1982). The OI group, on the other hand, had flexion motion in line with normal values. An average of 112 – 129° of hip flexion motion has been reported when performing activities such as tying a shoe, getting up and down from a chair, and picking up an object from the floor (Johnston and Smidt 1970). No single person in the S group had that much hip flexion when wearing their prosthesis. In hip extension, the S group showed better motion (mean difference 5°) when not wearing the prosthesis as compared with the OI group (Table I). This difference could be explained by the significantly shorter stump length in the OI group, which is known to increase the risk of developing a contracture in the hip flexor muscles. However, in the S group, hip extension was reduced when wearing the prosthesis. In the OI group, the situation was reversed (Table II), and the increased extension could be explained by the weight of the prosthesis. This made the measurement position more passive than active, as no socket was hindering the movement.
Comfort when sitting with a trans-femoral socket prosthesis can be assumed to be of high importance for the individual but has gained sparse attention in the literature. In a Swedish study, on established non-vascular trans-femoral cases (n = 97), 44% reported to have had moderate to a great deal of problem with the prosthesis making it uncomfortable to sit, so the quality of life was affected (Hagberg and Branemark 2001). In a more recent study, Pezzin et al. (2004) reported that nearly one-third of all major lower-limb amputees expressed dissatisfaction with their prosthetic comfort while standing and sitting. In the present study, 44% in the S group and 5% in the OI group reported at least a moderate degree of discomfort with sitting. The assessment of discomfort when sitting in the current study is, however, limited as no further questions on the perception on different aspects of sitting comfort were asked. Not surprisingly, less than 90° of hip flexion motion when wearing the prosthesis is obviously one factor affecting sitting comfort. When wearing a trans-femoral socket prosthesis, rotation of the hip in seated position is hindered by the socket. The lack of rotation could also be assumed to affect comfort when sitting, but this was not analysed further in this study. Contrary to Hachisuka et al. (1999), the authors did not find any relation between socket design (QL or IC socket) and discomfort with sitting; nor could they find any relation with regard to the socket material used. Other variables, not included in this study, seem to be related to discomfort with sitting when wearing a socket prosthesis. Additional research in this field is essential.
In the last couple of years, a new socket design, the Marlo Anatomical Socket (MAS), has been introduced for a trans-femoral socket prosthesis (Fairley 2004). The aim of this socket is to increase the range of hip motion, with the prosthesis, and to improve the comfort in sitting. No individual in the present study was supplied with a MAS socket, and no study was found in the literature reporting results on this new socket design. The authors welcome future studies of hip motion and sitting comfort with the MAS socket for individuals with a trans-femoral amputation.
Conclusion
This study shows that a conventional trans-femoral socket prosthesis significantly reduces the active range of motion of the hip joint and that discomfort when sitting is common among individuals wearing a prosthetic socket. The risk for discomfort when sitting increases if hip flexion motion in use with the prosthesis is less than 90°. In addition, the results confirm that individuals supplied with a direct bone-anchored prosthesis, using the method of osseointegration, have a normal range of hip joint motion when wearing the prosthesis and report very few problems with discomfort when sitting.
Footnotes
Acknowledgements
Thanks are given for financial support from Doktor Félix Neuberghs Stiftelse and Johan Janssons Stiftelse.