
Abstract
The biomechanical interaction between the leg stump and the prosthetic socket is critical in achieving close-to-normal ambulation. Although many investigations have been performed to understand the biomechanics of trans-tibial sockets, few studies have measured the socket interface pressure for trans-femoral amputees. Furthermore, no report has examined how the residual muscle activities in the trans-femoral stump affect the socket interface pressure characteristics during gait. In this study, an experimental method was developed to measure the trans-femoral socket interface pressures and EMG of muscles in the stumps of two trans-femoral amputees. Also, the measurement of three-dimensional prosthetic locomotion was synchronized to understand detailed socket biomechanics. Based on the experimental results, a significant correlation (P 50.05) was found between the measured temporal EMG amplitude and the interface pressure at the knee flexor (biceps femoris) and extensor (rectus femoris). Therefore, the residual muscle activity of a trans-femoral amputee's stump could be an important factor affecting socket-interface pressure changes during ambulation.
Introduction
In developing the products for rehabilitation, measuring techniques to obtain interface pressure distributions close to the human body become important. The most frequent application of the measured interface pressure is the assessment of rehabilitation engineering products, and the evaluation and development of prosthetic or orthotic devices. For example, the evaluation of interface pressure distributions is essential in the development of seat cushion orthoses for the disabled and elderly in order to prevent decubitus ulcer formation. For a normal-like ambulation, the dynamic interface pressure changes during gait also need to be understood for the design of comfortable trans-femoral and trans-tibial sockets for amputees.
Unlike measuring quasi-static interface pressure distribution such as the interface pressure on the buttocks, the interface pressure characteristics between the prosthetic socket inner wall and the soft tissue in a stump could have a dynamic interaction between the socket interface pressure and muscle activities during gait. Previously, the socket design was usually performed based on the static interface pressure distribution. As a result, amputees could experience severe pain caused by uneven dynamic interface pressure distributions during prosthetic walking. In addition, possible contractions of muscles in the stump could cause a more severe concentration of interface pressure than that in the static condition. However, the interaction between the socket interface pressure and muscle contraction in the stump during an amputee's gait has not been analyzed, since such an experiment would require the synchronized measurement of three different data sets: the socket interface pressure, the surface EMG from residual muscles, and the three-dimensional (3D) motion of the lower limbs.
EMG, a bioelectric potential, is frequently measured to understand muscle biomechanics in vivo. A recent study (Guimaraes et al. 1995) using an animal model showed that EMG has a strong correlation to the dynamic muscle contraction and force in vivo. Since EMG is usually measured using relatively thick electrodes, of more than 5-mm thickness, which should contact the human skin for measurement, locating the electrodes on the inner wall of the prosthetic socket is difficult. In addition, the thin interface pressure sensors should be located adjacent to the EMG electrodes, and both the sensors and the electrodes need to contact the skin of the stump during the amputee's locomotion.
For trans-femoral amputees, the biomechanical interaction between the stump and the prosthetic socket during the stance and swing phases of gait is critical for a normal-like ambulation. It is widely accepted that abnormal socket interface pressure distributions cause pathologies in the stump, which directly affect the gait of amputees. Although many investigations have been performed to understand the biomechanics of the trans-tibial socket, few studies have examined the static and dynamic behavior of the trans-femoral socket pressure. The results of these investigations suggested that the socket interface pressure changes during the gait of trans-femoral amputees were closely related to the prosthetic alignment, the socket shape, and the stump size (Lee et al. 1997). It is suggested that the temporal changes of hip moment during ambulation also affect the socket pressure distributions of trans-femoral amputees (Hong et al. 2001). Since knee flexor and extensor muscles act as assistants for the flexion and extension of the hip for normal gait, it could also be postulated that the residual muscles in the stump of trans-femoral amputees are still active to help the hip motions. As a result, the residual muscle activities could affect the socket interface pressure characteristics. However, the relationship between the residual muscle activities and the socket pressure is poorly understood, and the behavior of the knee flexors and extensors during the gait of trans-femoral amputees has not been studied.
In this study, an experimental method was developed to measure the socket interface pressure and EMG of muscles in the stump of trans-femoral amputees. The measurement of 3D prosthetic locomotion was also synchronized to understand detailed socket biomechanics. In addition, correlations between EMG and interface pressure of the stump were performed to understand the trans-femoral stump biomechanics. This was the first study to simultaneously measure the stump muscle activity using EMG, the socket interface pressure, and the 3D kinematics of the lower limbs during the gait of trans-femoral amputees. The purpose of this study was to analyze the relationship between the residual muscle activities and the socket interface pressure characteristics during the locomotion of amputees with trans-femoral prostheses. The developed experimental method for measurements of the trans-femoral socket interface pressure generation and EMG behavior could improve the trans-femoral socket design by minimizing stump pain and pathologies in a dynamic environment and may eventually help amputees to achieve a normal gait.
Materials and methods
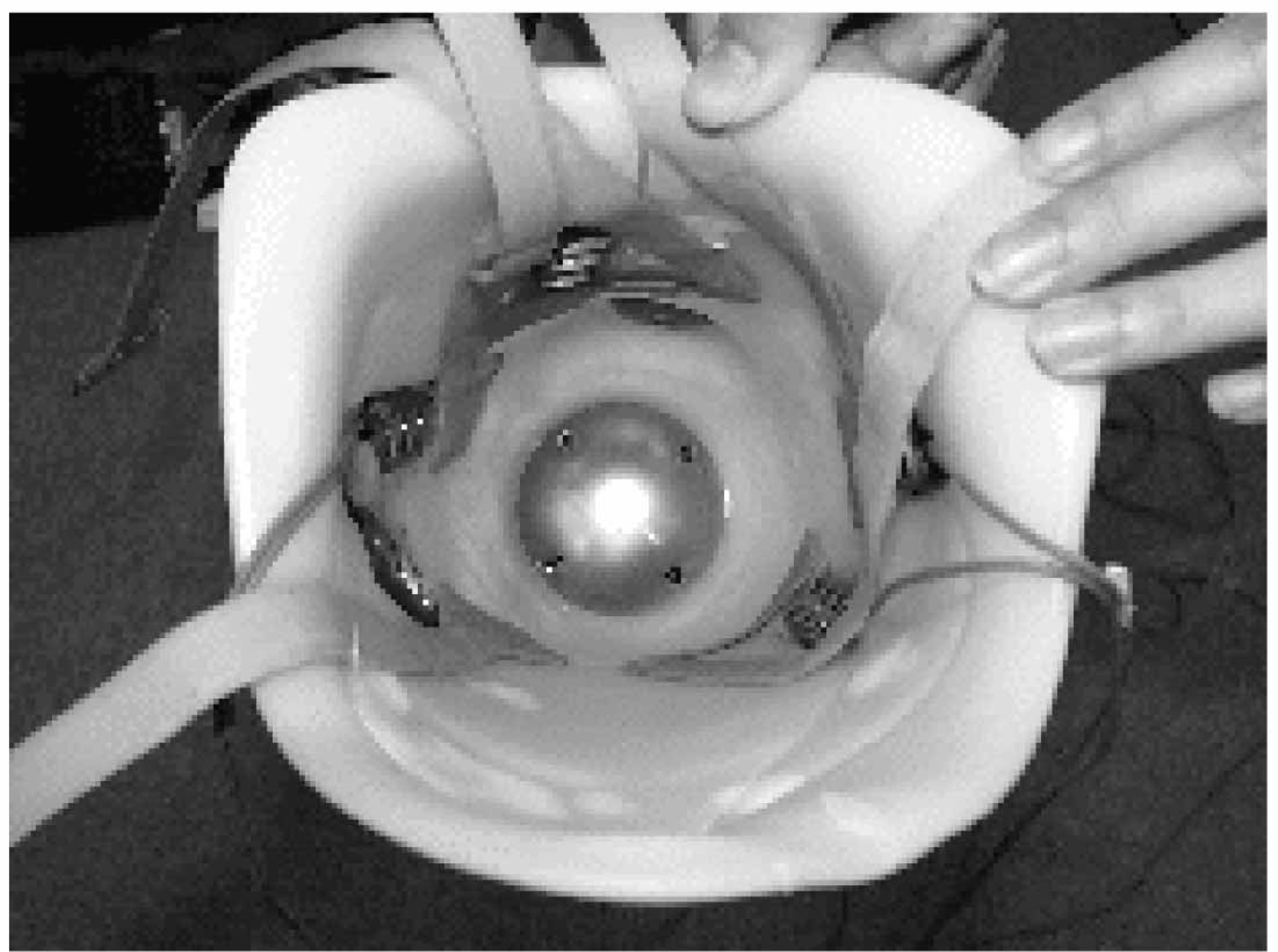
In this study, a 4-bar pneumatic knee trans-femoral prosthetic system (KOREC, Korea) was used, as shown in Figure 1. In addition, a quadrilateral suction socket based on brims (Otto Bock, Germany) was utilized. To measure the EMG of residual muscles in the stump, specially designed sockets allowing the EMG electrodes to be instrumented between the skin and inner wall of the socket were fabricated, based on the individual muscle anatomy of the subjects, as shown in Figure 2. The slots for the EMG electrodes were fabricated at two locations, the rectus femoris and biceps femoris. Figure 3 showed the electrode positions with respect to the stump.
Two unilateral trans-femoral amputees fitted with a knee prosthesis with a fixed ankle, energy storing foot, and quadrilateral suction socket (Figure 1) participated in the gait experiments for measuring the socket interface pressure near the EMG electrodes. Interface pressure sensors with a measuring system (Novel, Germany) were utilized. The interface pressure measurement system had 16 data channels. A 4 × 4 sensor matrix with plane dimensions of 20 mm × 20 mm was connected to each data channel via a data strip of custom designed length to meet the experimental condition. Thus, the data channel had a total of 16 piezoelectric pressure sensors of 0.2-mm thickness. Previously, interface pressure sensors using capacitance were mostly used. However, the measurement error due to the hysteresis, creep, drift, and effects of curvature is up to 33% (Polliack et al. 2000). As a result, interface pressure measurement in a dynamic environment using capacitance transducers was not reliable. The interface pressure sensors used in this study employed piezoelectric transducers with a measurement error of less than 3% with a measurable pressure range of 20–600 kPa. Before the experiments, a calibration was performed using a specially designed hydrostatic air pressure chamber.
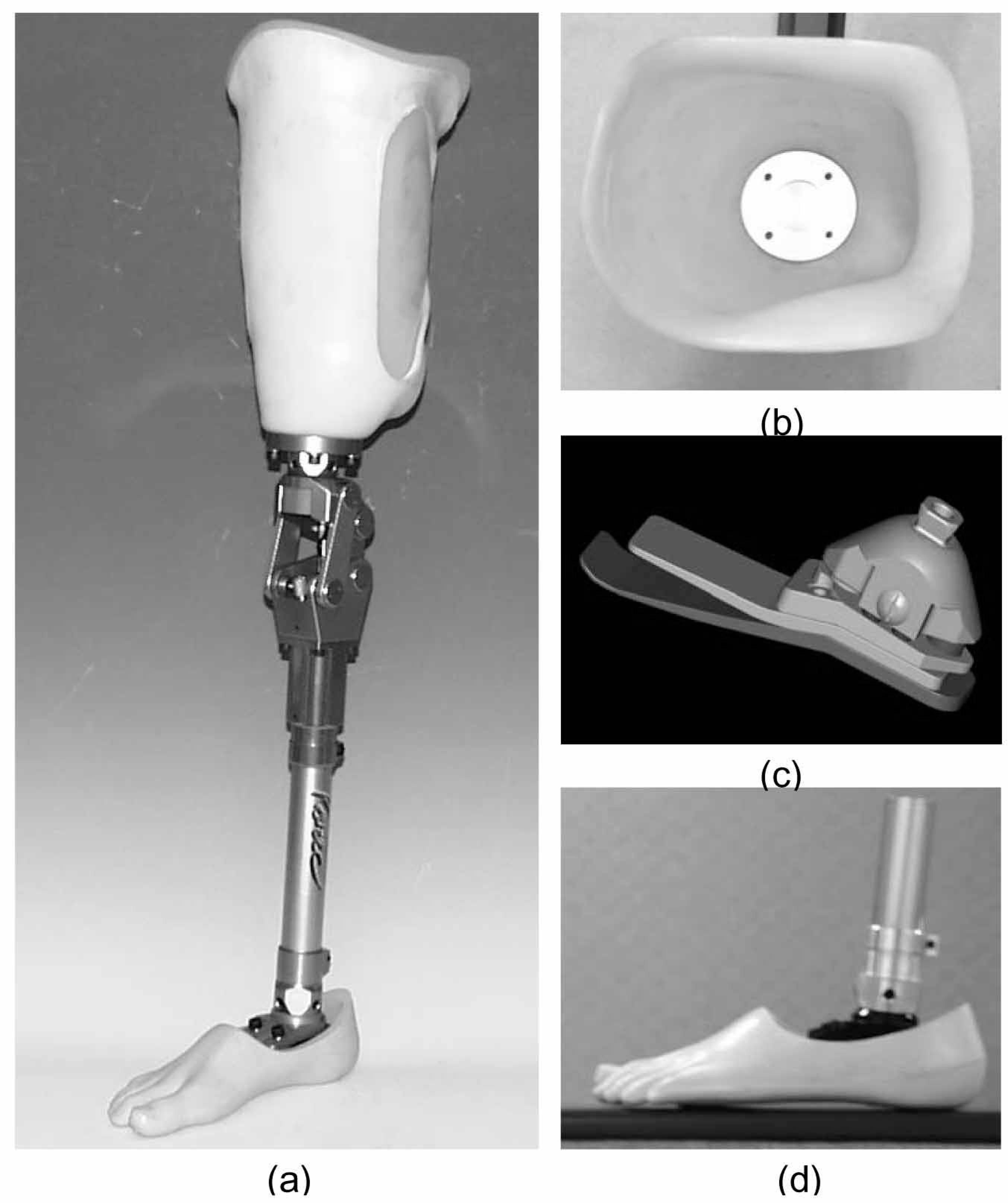
Four-bar pneumatic knee trans-femoral prosthetic system (a), which is composed of a quadrilateral suction socket (b), energy storing foot (c), and fixed ankle (d).
Specially fabricated trans-femoral socket for this study. The inner wall of the socket has slots for inserting MES electrodes. The locations of MES electrodes were determined based on individual stump muscles. The slots for the wires of the electrodes were also made for accurate socket-interface pressure measurement.
The 3D kinematics of the lower limbs during locomotion were measured using a stereo photogrammetric system, shown in Figure 4, that consisted of seven infrared emitting CCD cameras having 800 × 490 pixels (VICON, UK). Figure 5 shows the completed instrumentation and location of the markers in the trans-femoral prosthetic system. Two force plates (Kistler, Switzerland) were used to measure the ground reaction 3D forces and moments between the feet and the ground. Using the inverse dynamics method, the hip moment during prosthetic locomotion was calculated using the measured forces and moments, and the kinematic data. The modeling process to determine the hip moment, the body builder (VICON, UK), was utilized.
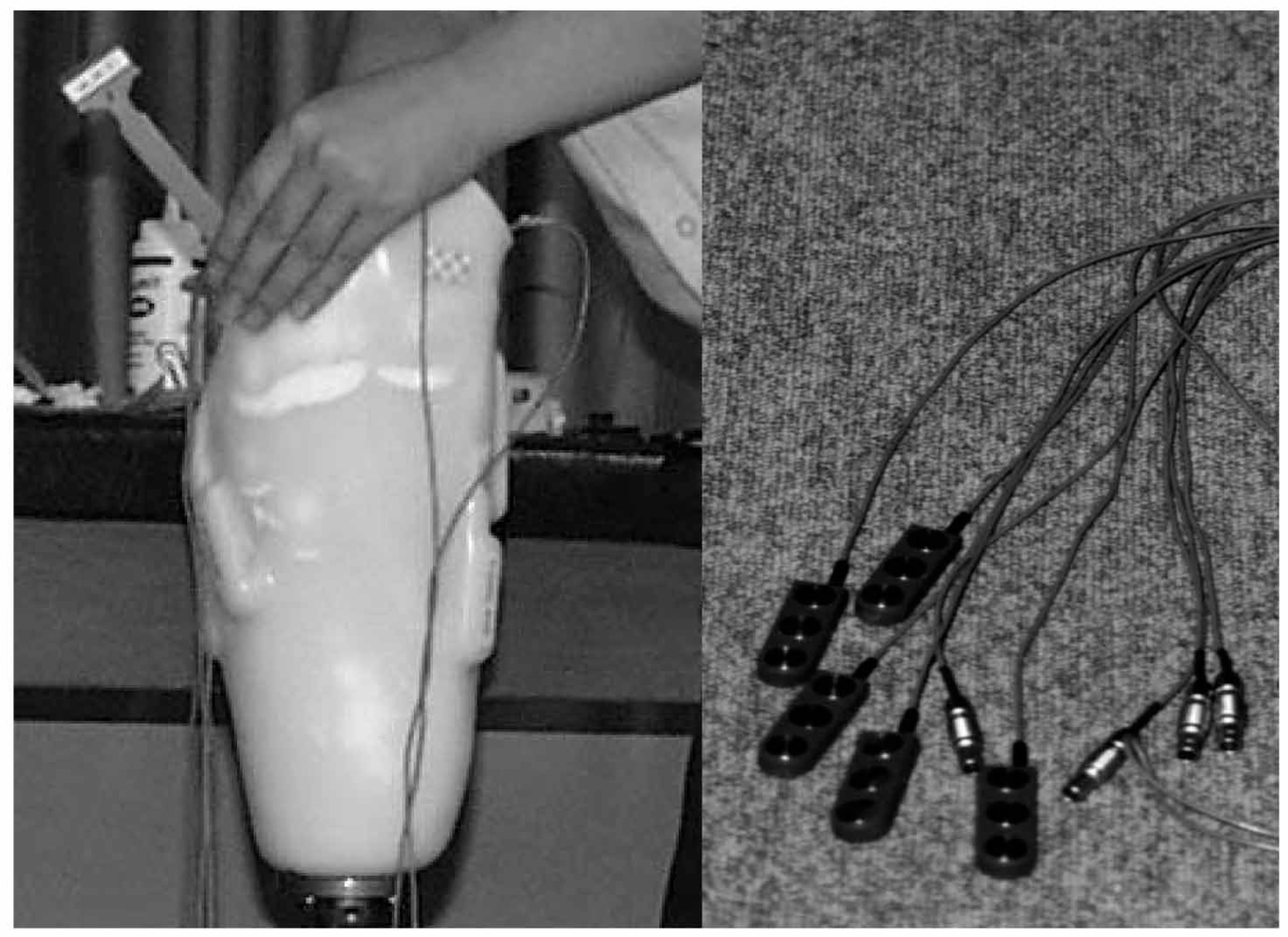
The EMG electrodes were inserted into the inner slots of the socket located on the rectus femoris, biceps femoris, knee extensor, and flexor. Figure 6 shows the complete instrumentation for measuring the socket interface pressure and EMG in residual muscles. EMG was measured at a sampling rate of 1200 Hz and processed using the adaptive filter algorithm (Alessio and Conforto 2001). Since the conventional EMG processing used a filter that always utilized a fixed number of consecutive data and a fixed order of polynomial, the resulting enveloped EMG was not sensitive to represent the dynamic changes of muscle activities. The applied EMG processing method could change adaptively the number of consecutive data used and the order of polynomials, depending on the time variation of the signal. As a result, the processed enveloped EMG could follow the dynamic variations of EMG sensitively over time.
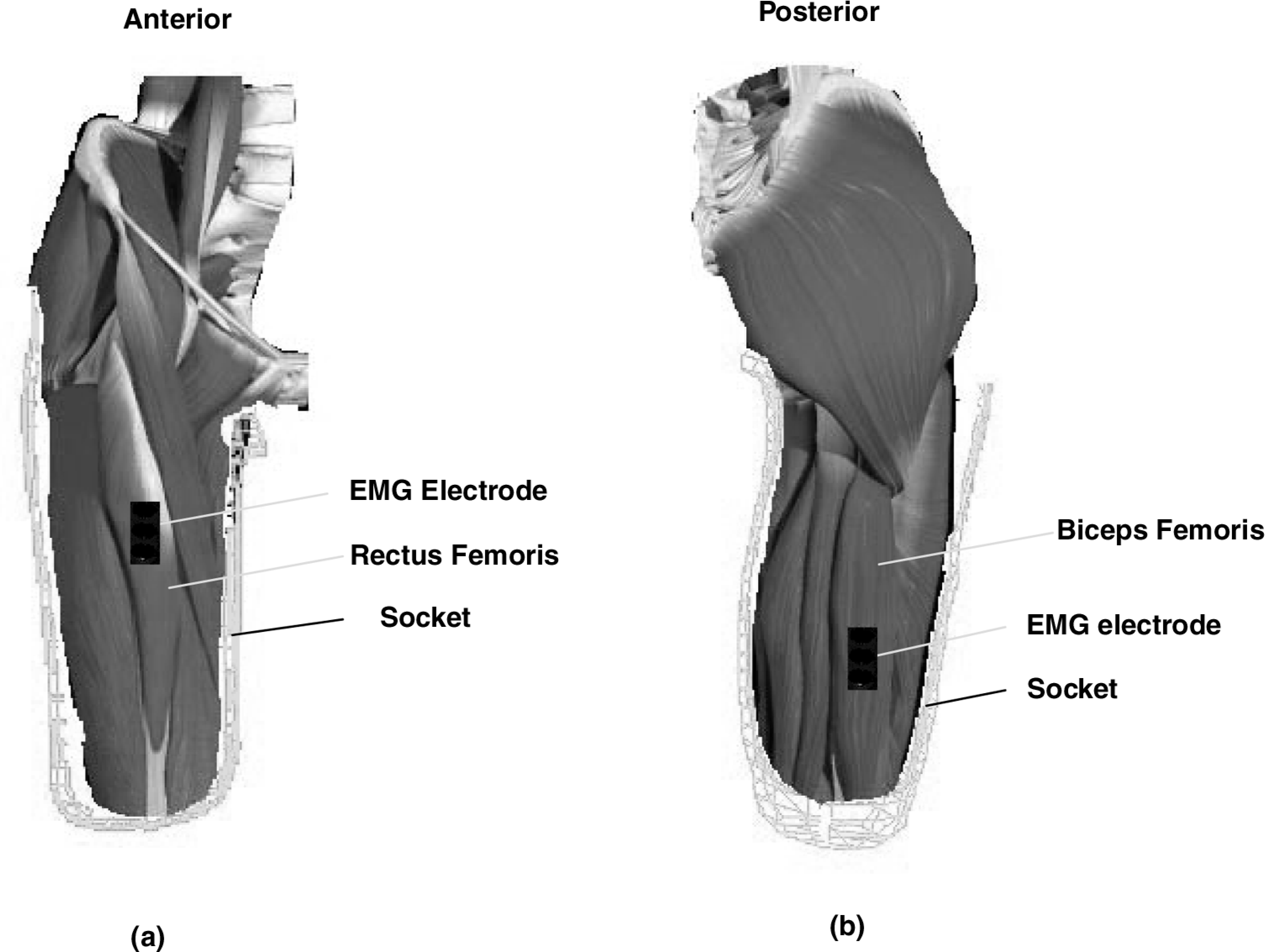
Electrode positions with respect to the stump. For the biceps femoris, the electrode was positioned at a point on a line between the ischial tuberosity and the amputated end (the fibular head for normal subjects). For the rectus femoris, the electrode was positioned at a point on a line between the anterior superior iliac spine and the amputated end (the patellar for normal subjects).
The prosthetic knee, foot, ankle, and socket were developed by the Korea Orthopedic and Rehabilitation Engineering Center (KOREC). The subjects had no prior stump pain and disorder. Before the tests, two subjects aged 48 and 52 years were instructed and trained for 4 weeks for a close-to-normal ambulation with the prosthesis. The prosthetic system, including the socket, was carefully aligned by the CP team, consisting of four personnel of KOREC, based on each individual subject to ensure a close-to-normal walking before the experiments. Data acquisition was performed in a manner that captured one complete gait cycle at a mean gait speed of 1.14 m/s. A minimum of five gait trials were performed for each subject for the statistical analysis at a rate of 60 frames per second. The pressure measurements, and ground forces and moments were synchronized to the gait experiments. Figure 7 shows a prosthetic gait experiment on a trans-femoral amputee measuring the socket interface pressure and EMG of the stump muscles.
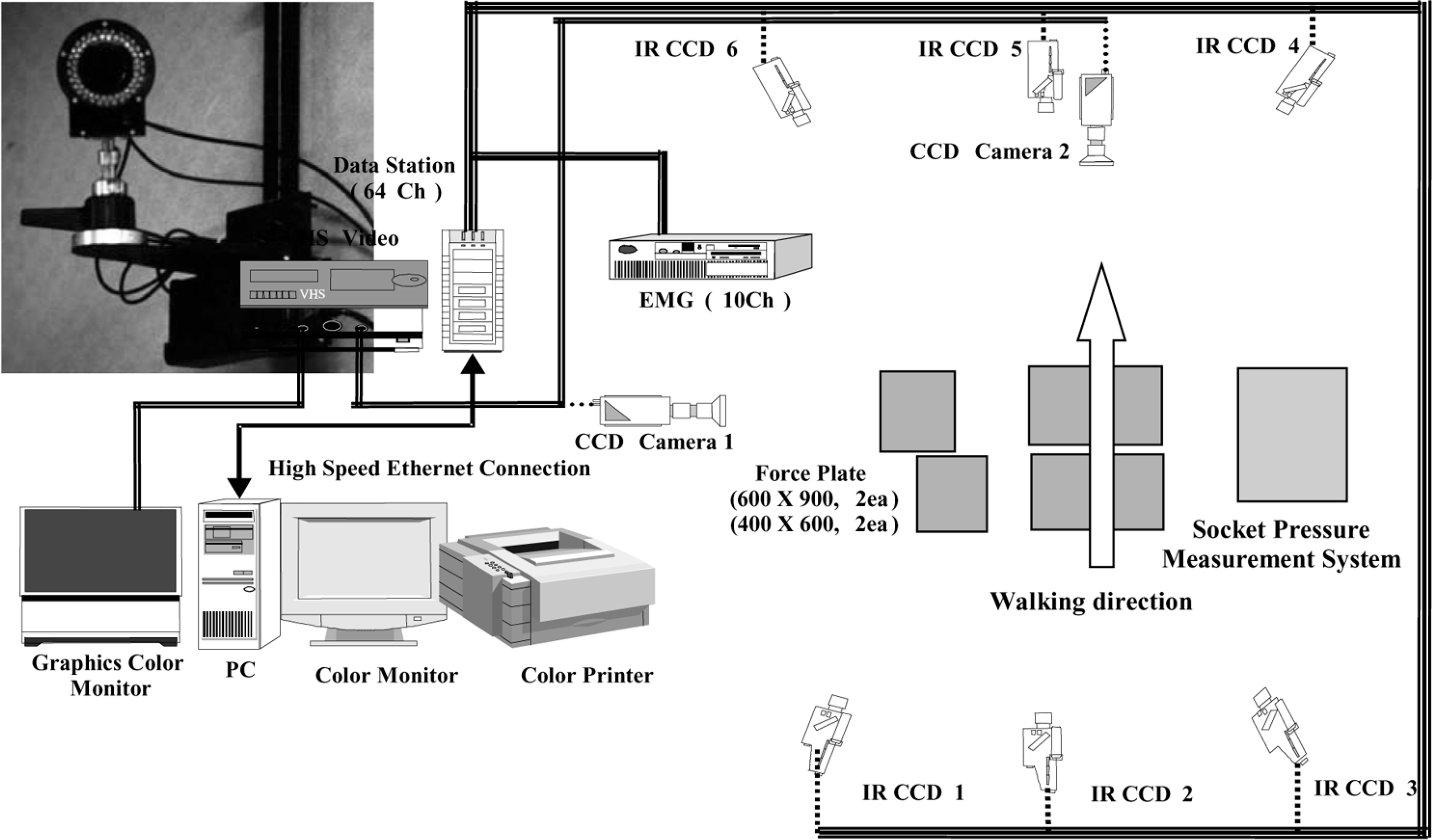
Schematic configuration of the stereo-photogrammetric system to measure 3D kinematics of lower limbs during prosthetic gait.
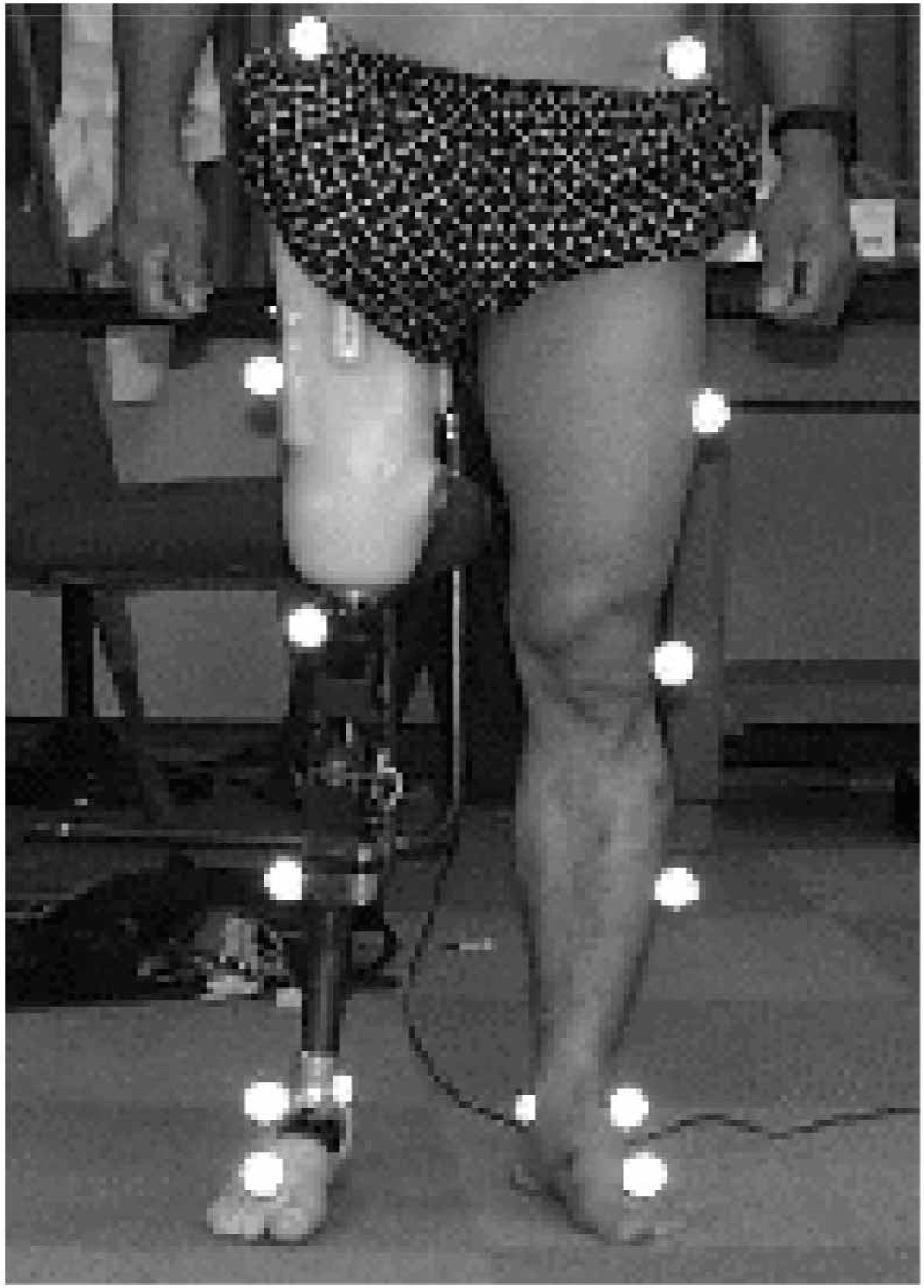
Reflective marker positions to measure the 3D kinematics of lower limbs during prosthetic gait.
To determine gait events (initial contact: IC; foot flat: FF; push-off: PO; toe-off: TO; and terminal swing: TS), the 3D kinematics of the prosthetic lower limb were analyzed from the gait experiment results. EMG and socket interface pressure values were obtained at each gait event. The Pearson correlation method (Minitab, USA) was applied to understand the relationship between the EMG amplitude of the stump muscles and the measured socket interface pressure changes.
Completed instrumentation for measuring socket interface pressure and EMG of stump muscles during gait.

Prosthetic gait experiment on a trans-femoral amputee by measuring the socket interface pressure and EMG of stump muscles.
Results
Figure 8 presents examples of the temporal spatial distribution changes of interface pressure at the residual muscles in the stump for subject A during gait. The pressure was analyzed using the maximum pressure, since the concentration of interface pressure could be a major factor to cause stump skin pathologies and pain (Ryu et al. 2001). Figure 9 shows examples of measured trans-femoral amputees' EMGs from the biceps femoris and rectus femoris for the two subjects. Figures 10 and 11 are the plots of averaged EMG and interface pressure for five trials with respect to each gait event for the biceps femoris and rectus femoris in the stumps of the subjects A and B. Figure 12 presents the averaged variations of hip moments (for five trials) for the amputated limb during prosthetic locomotion. The prosthetic hip moments were compared to the averaged hip moment of normal persons, which had been previously performed at KOREC with subjects, aged 40–50 years.
For all events in the gait cycle such as IC, FF, PS, TO, and TS, the socket interface pressure values of the rectus and biceps femoris were significantly correlated with the EMG behavior for both subjects (P < 0.05). Pearson correlation coefficients were 0.92 and 0.86 for the rectus femoris, and 0.72, and 0.61 for the biceps femoris, for subjects A and B, respectively.
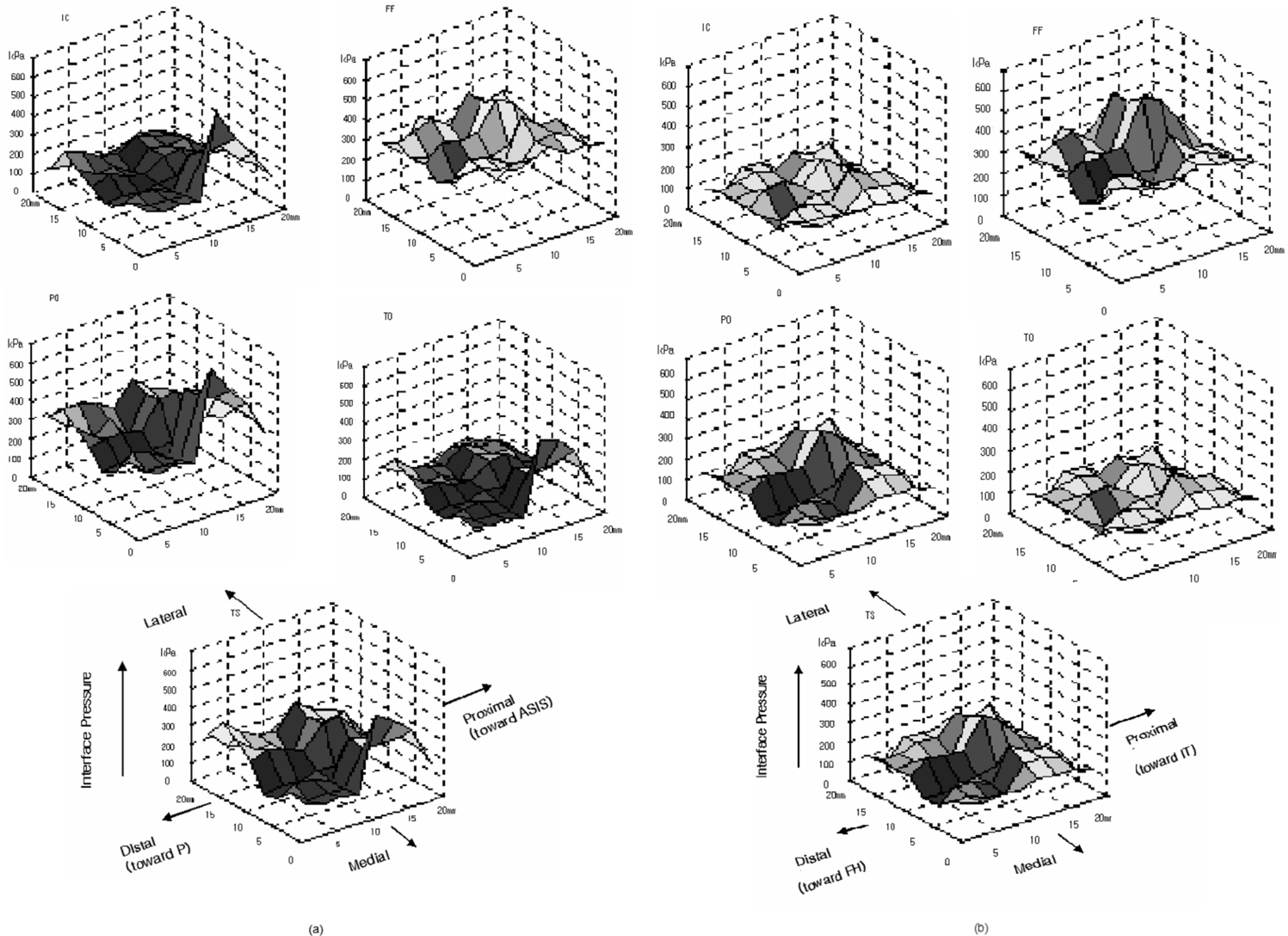
Examples of interface pressure distribution at each gait event for subject A. The vertical axis represents pressure value, the transverse plane shows the spatial dimension of sensor matrix (4 × 4), and (a) and (b) represent the temporal variations of the pressure for the rectus and biceps femoris, respectively.
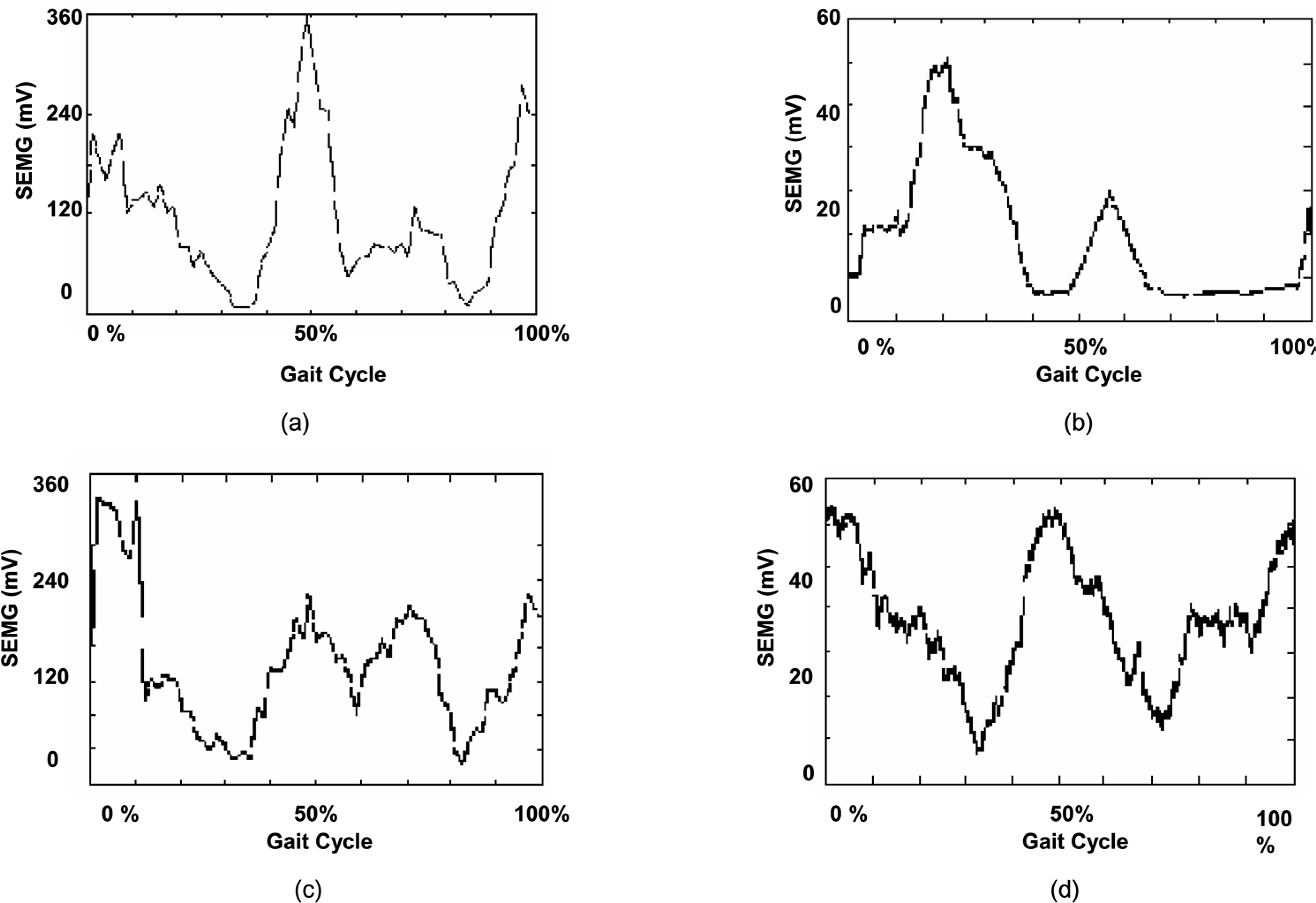
Examples of trans-femoral amputees' stump muscle activities of the biceps femoris and rectus femoris plotted as a function of the gait cycle. (a) EMG of the biceps femoris, subject A; (b) EMG of the rectus femoris, subject A; (c) EMG of the biceps femoris, subject B; and (d) EMG of the rectus femoris, subject B. SEMG is the surface electromyograph.
Discussion
Figure 13 shows EMGs of the rectus femoris and biceps femoris, and hip and knee moments from a normal person's gait (Vaughan et al. 1999). For the purpose of comparison with the kinematics of the lower limbs, the hip and knee moments obtained from normal subjects were plotted with the normal person's EMGs as shown in Figure 13. Although the biceps femoris is the main knee flexor, it was observed that the activity of the biceps femoris is close to the change in the hip extension moment at the early stage of the gait cycle (IC to about FF). Meanwhile, the rectus femoris contributes as a hip flexor from near PO to TO (Winter et al. 1995). For the last stage of the gait cycle (TS), the biceps femoris partly works as a hip extensor.
The trans-femoral amputees who participated in this study showed a good stump condition. On MRI, subject A had relatively well-preserved hamstrings and quadriceps. Subject B had good hamstrings, but the vastus lateralis was nearly lost.
As can be seen in Figures 10 and 11, the biceps femoris activity levels of the trans-femoral amputees were low at IC. EMGs of the biceps femoris increased at FF (about 10% of gait cycle). Figure 12 shows that the extension moments of the trans-femoral amputees were much lower than those of normal persons at IC. As the biceps femoris activities of the trans-femoral amputees increased, the hip moments increased up to the normal person's moment value from FF. EMG of the trans-femoral amputees decreased gradually to TO and then increased to TS. As a result, the hip-extension moments of the trans-femoral amputees increased at the last stage of the gait cycle. Thus, the biceps femoris of the trans-femoral amputees was able to remain active, even though it was damaged because of the amputation. This could mean that the biceps femoris in the trans-femoral stump was still working as an assistant for the hip extensor.
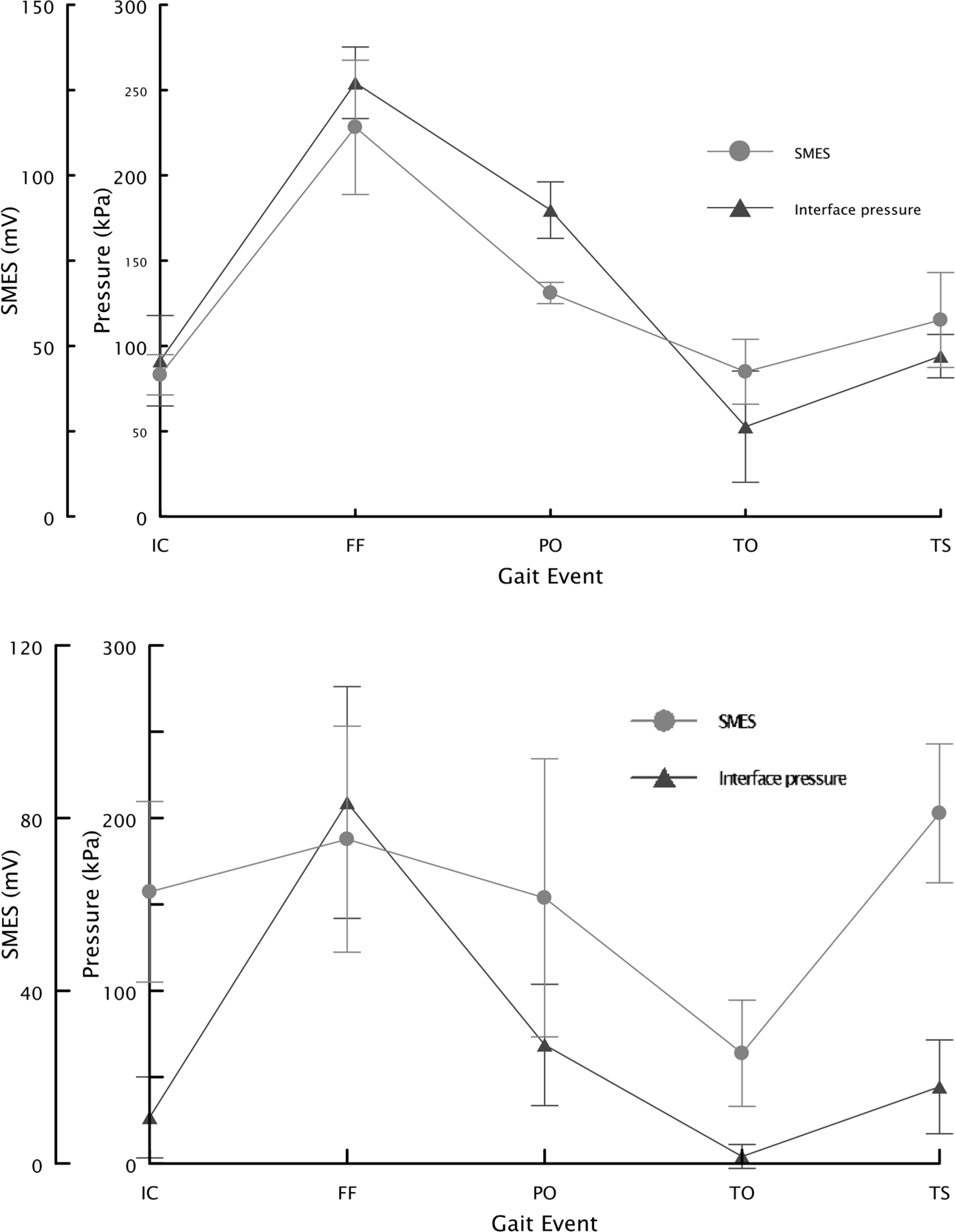
Socket-interface pressure and EMG for gait event (subject A). The upper figure is for the rectus femoris (knee extensor) located at socket anterior. The lower figure is for the biceps femoris (knee flexor) located at socket posterior. SMES is the surface myoelectric signal that is synonymous to the surface electromyograph.
For the rectus femoris (Figures 10 and 11) of the trans-femoral amputees, the activity could still be observed, as seen in the normal gait (Figure 13). Generally, the maximum EMG from the rectus femoris appears near FF for normal persons to stabilize the hip during the middle stage of the gait cycle (Vaughan et al. 1999; Winter et al. 1995). However, the activity of the rectus femoris for subject B occurred at PO, although a close-to-normal hip flexion moment was observed. This might have been caused by the absence of subject B's vastus lateralis. At the last stage of the stance phase, the amputees' rectus femoris could assist the hip flexion, based on the variations of near-normal EMGs and hip moments (Vaughan et al. 1999; Winter et al. 1995). Therefore, the residual muscles in the trans-femoral stump remained active to assist the gait of the trans-femoral amputee.
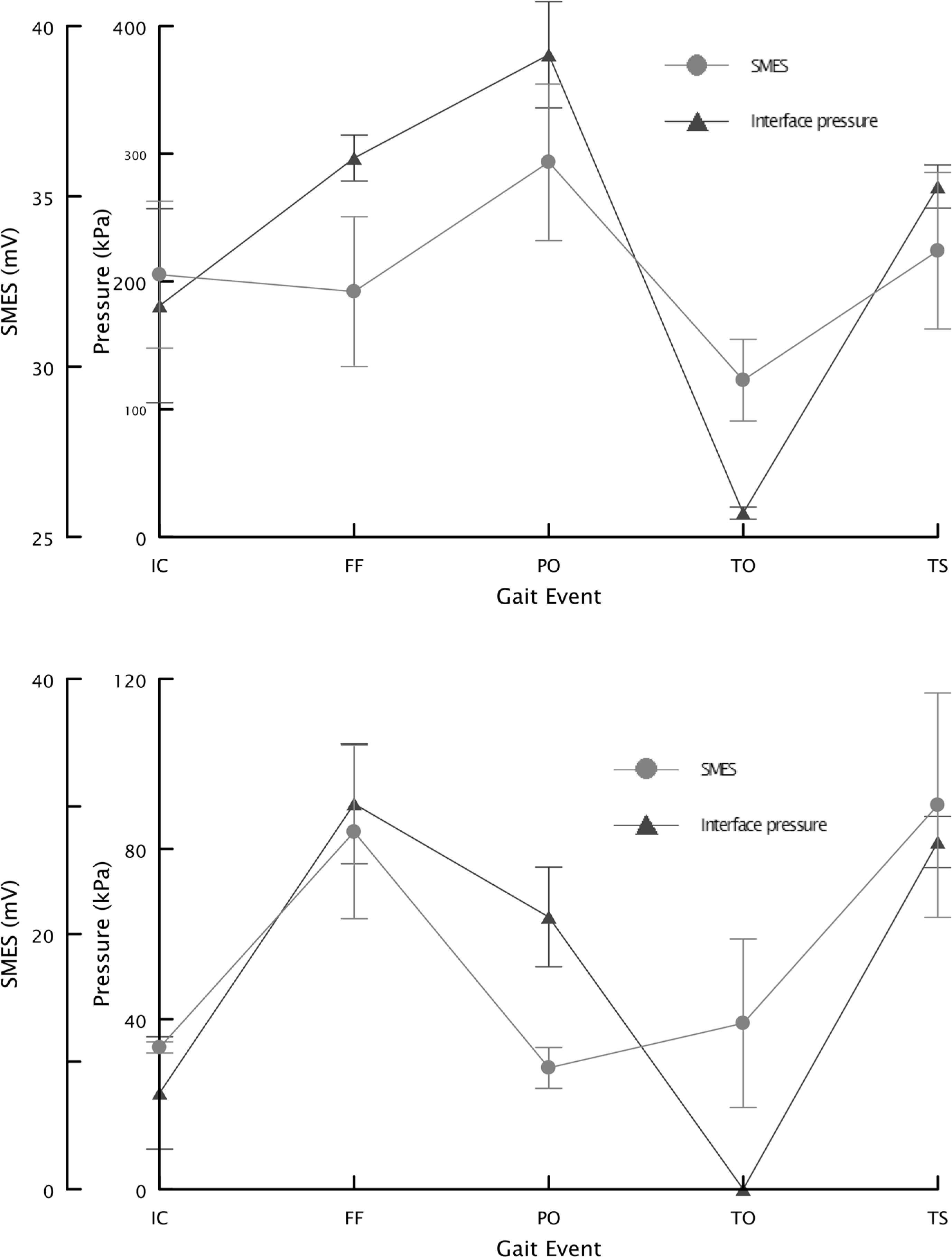
Socket-interface pressure and EMG for gait event (subject B). The upper figure is for the rectus femoris (knee extensor) located at socket anterior. The lower figure is for the biceps femoris (knee flexor) located at socket posterior. SMES is the surface myoelectric signal that is synonymous to the surface electromyograph.
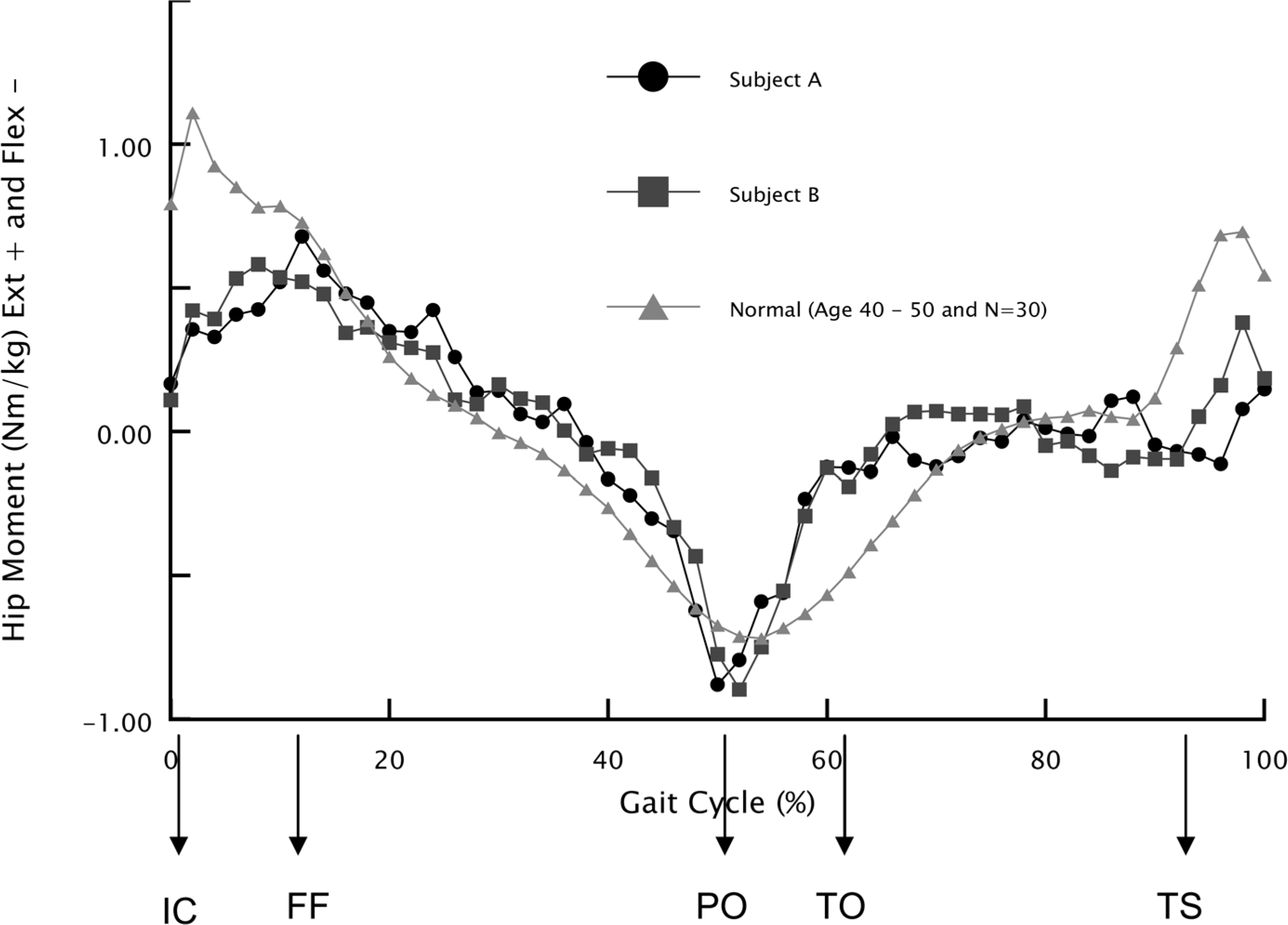
Temporal variations of hip moment for subjects, and normal person.
In Figures 10 and 11, the measured socket interface pressure and EMG of the rectus femoris and biceps femoris (subject A and B) in the trans-femoral stump were plotted for all gait events. As indicated by a previous study (Lee et al. 1997), the interface pressure at the rectus femoris located at the anterior socket wall was higher than that at the biceps femoris located at the posterior socket wall for both subjects. The differences in maximum interface pressure between this study and the previous study (Lee et al. 1997) might have been caused by the individual characteristics, the use of a different prosthetic system, and a different fabrication method for the trans-femoral socket.
As shown in Figures 10 and 11, the interface pressure values at the rectus and biceps femoris were significantly correlated with the EMG behavior for both subjects (P < 0.05) for all events in the gait cycle such as IC (initial contact), FF (foot flat), PS (push-off), TO (toe-off), and TS (terminal swing). Based on the test results, it was suggested that the residual muscle activities of the amputee's stump are important factors affecting socket interface pressure changes during locomotion. Therefore, it is important that the dynamic activities of residual muscles in the trans-femoral stump be considered in the design of a more comfortable and physiological prosthetic socket. Further study with a larger population is required for a complete understanding.
Acknowledgments
This work was supported by the Grants for Upcoming Researchers (003-D00591) in the programme of Supports for Outstanding Researchers planned by Korea Research Foundation.
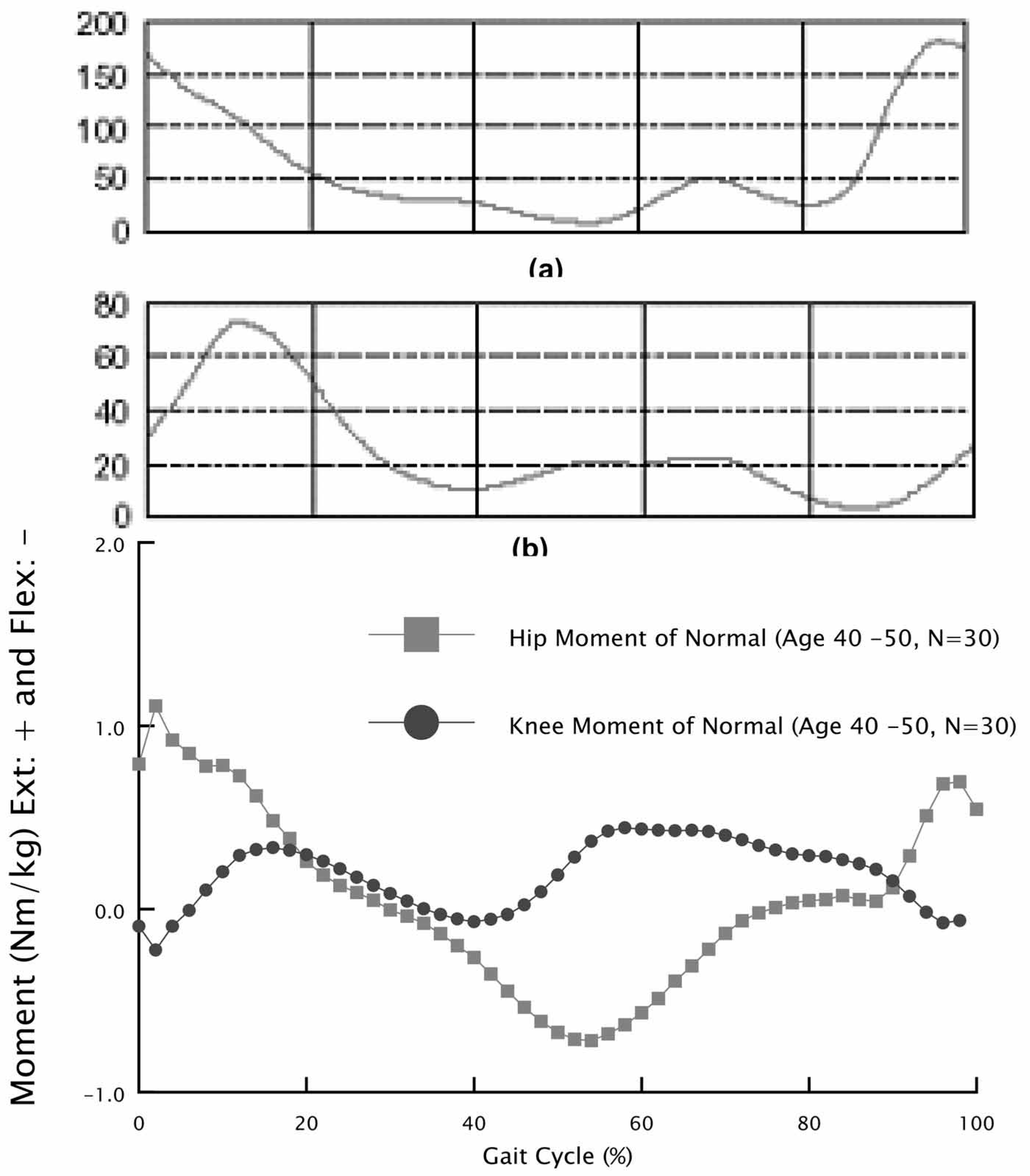
Normal person's muscle activities (the vertical axis is EMG in millivolts) of the biceps femoris (a) and rectus femoris (b) plotted as a function of the gait cycle (Vaughan et al. 1992). The normal person's hip and knee moment is plotted as a function of the gait cycle.