
Abstract
Given the importance of minimizing transverse plane shear stress on soft tissue, several transverse rotational adapters (TRAs) are available for incorporation in lower limb prostheses. This study compares kinetic and kinematic data from human subjects during straight and turning gaits to the mechanical performance of several TRAs. Physiological data were collected from three individuals walking straight and turning at self-selected speeds around a 1m radius circle. The average peak torques and range of motion for normal subjects while turning were 8.2 Nm and 26° (outside leg), 11.8Nm and 20° (inside leg), and 11.4Nm and 20° (right leg) during straight gait. Each TRA was mechanically tested without axial loading in a servo-hydraulic material testing system (MTS) over its rotational range at 0.5°/s and 60°/s. The TRAs with axial compression were also tested at 0.5°/s under a 736N (75kg mass) axial load. Applying these torques to the different TRAs yielded 3 to 35° rotation, depending on the elastomer installed. Some TRAs had nearly constant stiffness, while others stiffened with rotation. The TRAs also varied in their average maximum stiffness from 0.4Nm/°to 2.7Nm/°. Normal subjects exhibit interior vs. exterior asymmetrical torques and displacements; however, only one of the TRAs is designed to allow asymmetrical stiffness, and none have asymmetric ranges. Prosthetists and physicians can use these data to better interpret amputees' qualitative remarks and to prescribe the correct TRA and/or elastomer. This information also forms a basis for further design and development of novel torque absorbing prosthetic adapters.
Introduction
For intact subjects while walking straight or turning, the leg acts as a system of rotating elements coupled in series, each doing some combination of elastic energy storage and release, torque transformation into motion in other planes, and torque transmission. The net torque results in transverse rotation of the foot (if it overcomes static friction with the substrate, or slides within the shoe), ankle and subtalar joint, tibia and fibula, knee, and hip. For the amputee, portions of this kinetic chain are replaced with the prosthesis. Whatever torque was applied to the biological structures that were removed, are now applied to the prosthesis and its interface with the stump. An intact leg is free to rotate in the transverse plane as described above, or to transmit the transverse rotation into motion in other planes; however, with the exception of the prosthetic foot rotating in the shoe, few lower limb prostheses allow for transverse rotation. Constrained rotation can increase stump shear stresses and, for some amputees, may be sufficiently uncomfortable to necessitate an altered gait. Given that discomfort and injury due to shear forces between the stump and the prosthetic socket are major complaints of amputees (Dillingham et al. 2001; Ehde et al. 2000; Hagberg and Branemark 2001; Legro et al. 1999; Marshall et al. 2002; Nielsen 1991; Schoppen et al. 2001), it is important to minimize the shear forces in all planes of the socket/lining with respect to the stump.
While several products are currently available to reduce tissue loading in the transverse plane, little objective data exists documenting the effects of these devices during turning gait or during typical activities of daily living. Lamoureux and Radcliffe (1977) explored several designs for a pylon device that allowed axial rotation. Using a prototype device, they conducted a treadmill experiment (n=2 trans-femoral amputees) and found that pelvis rotation increased 68, step length increased, and the shank externally rotated 88 over the foot during stance with the prototype in comparison to a standard pylon. In another study, Van der Linden et al. (2002) researched rotation adapters on two subjects walking at their self-selected speed. One subject showed greater axial rotation of the socket relative to the foot with the transverse plane rotation adapter. They concluded that the rotation adapter allowed the socket to rotate with the stump, which may imply that motion between the stump and socket was reduced. These studies illustrate some of the effects of rotation adapters; yet, except for manufacturers' claims, there are no published reports on the influence of rotation adapters during more complex gait activities where torsional loads are expected to be higher than for linear walking. Aside from the manufacturers' product documentation, there is also no way to ascertain the differences between adapters or between different elastomers used in the same adapter. This study was conducted, with prosthetists in mind, to characterize the mechanical properties of the available adapters and to raise the question of how exactly should a TRA respond to torque.
Materials and methods
The kinetic and kinematic data are taken from three intact subjects, each of whom performed five trials walking straight and turning to the right around a 1m radius circle at their self-selected speeds. All subjects gave their informed consent to participate in this study after the human subjects institutional review board governing the institution approved the protocol. All were free from musculoskeletal and neurological problems by self-report. Thirty-six reflective markers were placed on each subject according to the Plug In Gait model (Vicon, Oxford Metrics, Oxford, UK). A ten-camera Vicon 612 system recorded the three-dimensional coordinates of the markers at 120 Hz. A Kistler force plate (Winterthur, CH) mounted flush with the laboratory floor recorded the kinetic data at 600 Hz. Using the Vicon generated embedded coordinate axes, foot angle was defined as the angle between the heel to second ray axis and the axis through the ankle centre perpendicular to the trans-malleolar axis (Figure 1). Zero foot angle was recorded with the subject standing still, after receiving instructions to look straight ahead and to stand evenly on both feet. Internal rotation and torque are positive and external rotation and torque are negative. Torque is reported as moments generated by the subjects to counter environmental moments. The data include three conditions: right footstrikes during straight walking, right turns on the left foot, and right turns on the right foot. While it is becoming clear that there are asymmetries in lower limb function in able-bodied gait, there are no studies definitively linking symmetry to limb dominance or laterality in turning gait (for review, see Sadeghi et al. 2000). For the purposes of this study, the authors assume that the functional roles of the inside and outside legs during turning are the same, regardless of turn direction. To ensure a constant velocity, the subjects walked 5 to 6 steps (either straight or around the circle) prior to stepping on the force plate. The data were analyzed with Vicon's Workstation and Polygon software.
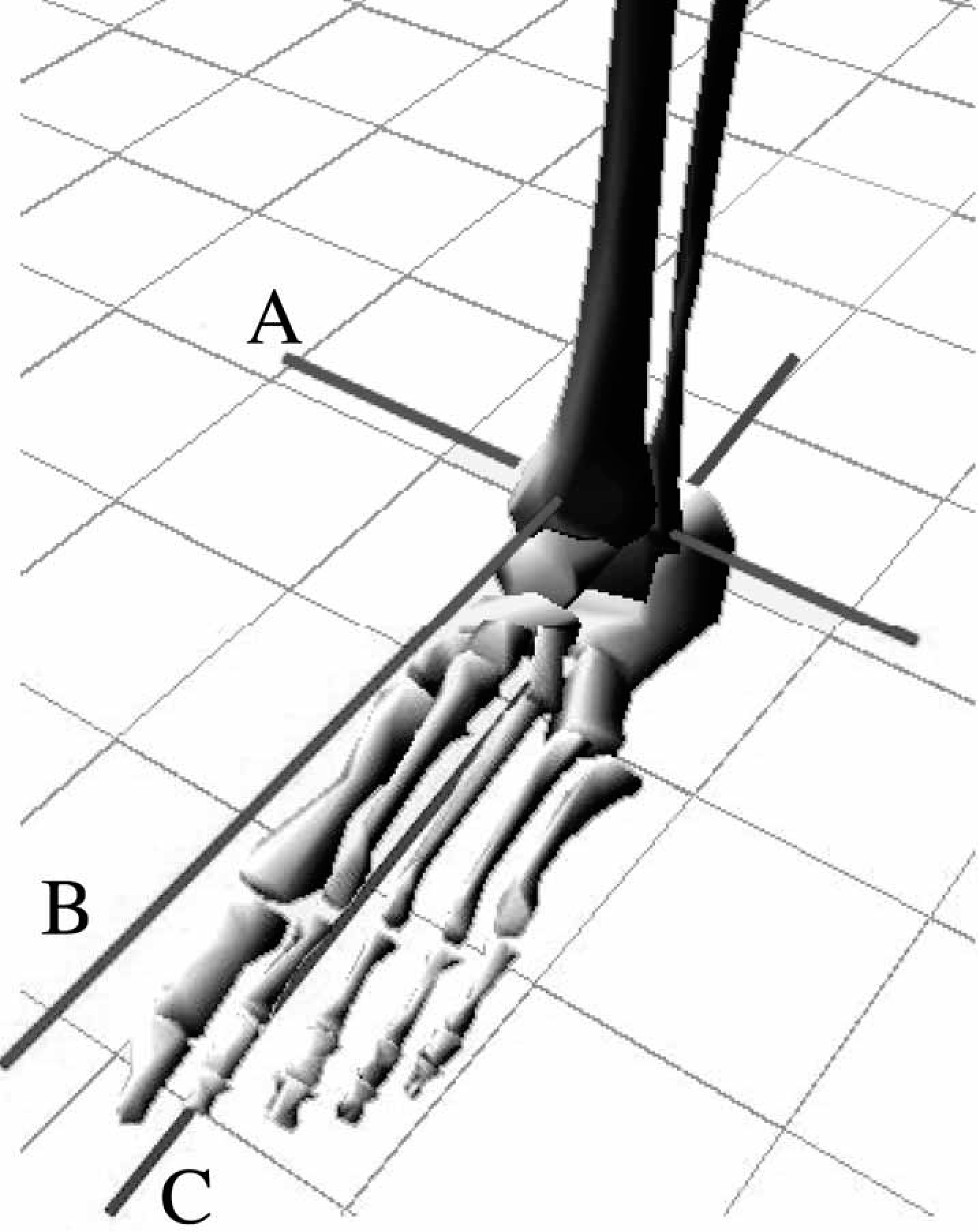
Diagram of axes used in calculating foot-tibia angle. The foot-tibia angle is the angle between (B) and (C) in the transverse plane. A: trans-malleolar axis, B: axis perpendicular to (A) through the ankle centre, C: axis from heel to second ray
The Transverse Rotation Adapter (TRA) performance data came from five transverse rotation adapters that were purchased for testing (Table I) and assembled as necessary with standard pylons and tube clamp adapters. Each TRA has the same basic elements: upper and lower tubes or tube clamp adapters that rotate with respect to one another and a deformable elastomer or spring within a housing that connects them. Both Endolite TRAs use a white Delrin rod that is fabricated with thicker or thinner walls to vary the stiffness. The Delta Twist compresses urethane elastomers, and can be set to a different stiffness for internal and external rotation, while the 4R39 uses bevel washers under adjustable spring tension. The Century XXII compresses an elastomer sleeve mounted around an internal radial arm. The Delta Twist, TT Pylon, and Century XXII compress axially, in addition to rotating in the transverse plane.
Each TRA was mounted in a servo-hydraulic material testing system (MTS; Model 858 Bionix™; MTS System Corporation, Eden Prairie, MN). The long axis of the pylon and TRA was aligned with the MTS axis of rotation, with the TRA oriented upward (as if installed distally to the knee). Each elastomer for each TRA was tested over the full rotational range (from the users manuals) with no axial load, at 0.58/s, 608/s, and at 0.58/s with the elastomer removed (where possible) to quantify friction. The Otto Bock 4R39 has a non-removable spring and bevel-washer system that is adjusted with a screw; this TRA was tested in the middle and at the extremes of its stiffness. For the Century XXII, the angular range was established by rotating the TRA with the elastomer removed, noting the angles at which contact between the internal metal elements of the adapter occurred. The full range, contact-to-contact, was +158, so +138 was used for testing to avoid damaging the elastomer. For the TRAs with axial compression, an additional test of the middle stiffness elastomer was conducted at 0.58/s while the adapter was axially loaded to 736N (75kg, a representative mass for subjects who would use this TRA and elastomer). For all tests, the MTS was programmed to rotate, using displacement control, from centre counterclockwise (from above) to the end of the range, then clockwise through the full range, then counterclockwise back to centre. Repeatability was ensured by visual comparisons of multiple tests of each TRA (data not shown). The MTS sampling rate was 10Hz for the 0.58/s trials and 1000 Hz for the 608/s trials. For the Endolite TRAs, an expected torque-deformation curve was generated by multiplying the published stiffness values over the range of angular deformation.
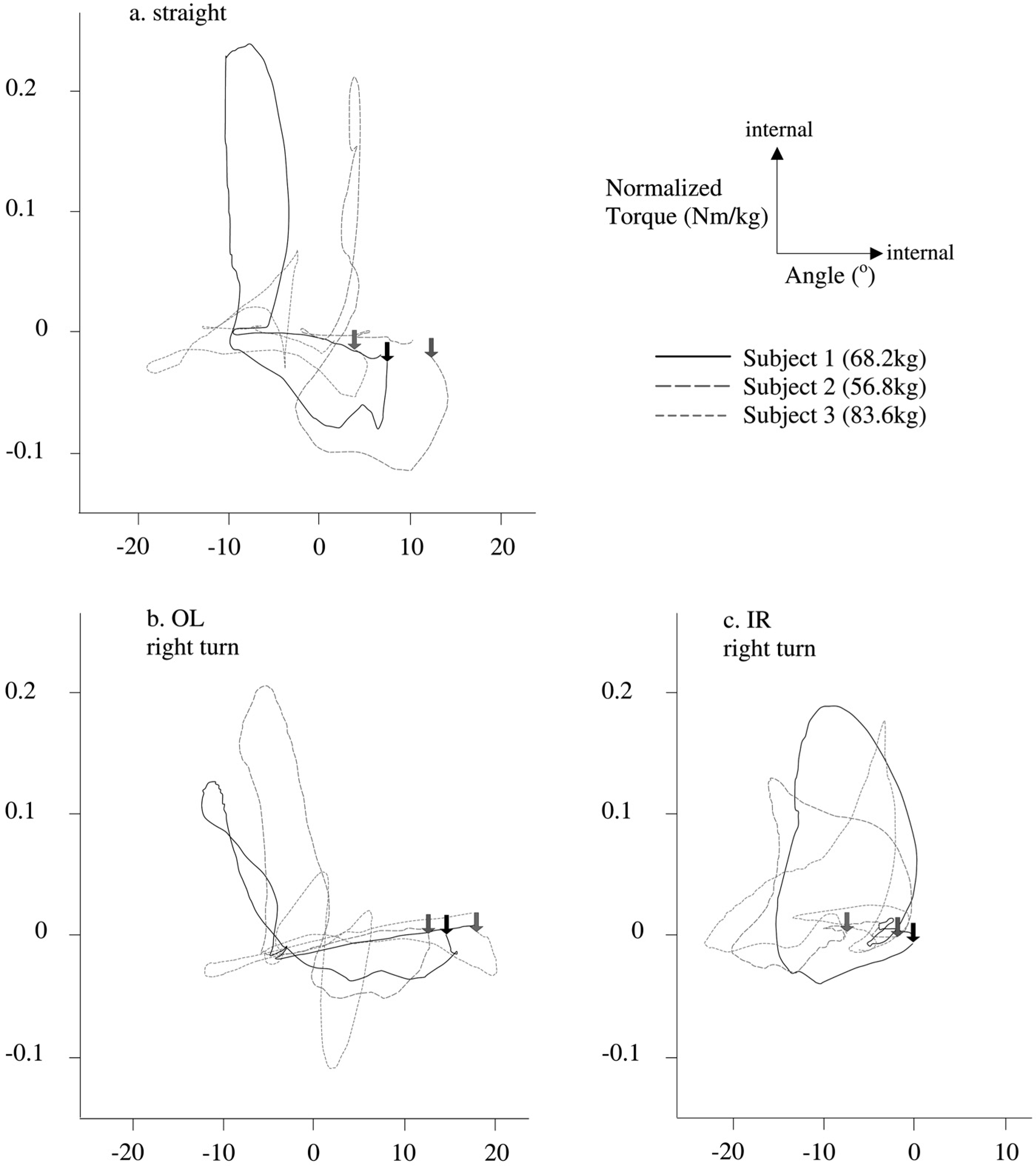
Documented performance properties from the users' manuals of all devices tested. The Delta Twist was the only device that came with a listed mass. The other devices were weighed in the lab without couplers.
tube cut to 70 mm
with 143 mm; carbon fibre tube and tube clamp adapter;
tube cut to 149 mm;
listed in users' manual;
tube cut to 95 mm.
Since the integral of the curve on the portions acting against the elastomer is greater than the integral on the portions relaxing with the elastomer, the area within the loop (hysteresis loop) on the torque vs. deformation plot represents the total energy lost per cycle. The area within the loop when the TRA is tested at 0.5 8/s without an elastomer represents the energy lost to friction. The energy loss calculations were done with the public domain NIH Image programme (developed at the US National Institutes of Health and available on the Internet at http://rsb.info.nih.gov/nih-image/) by measuring the digitized areas within the torque vs. deformation curves.
Results
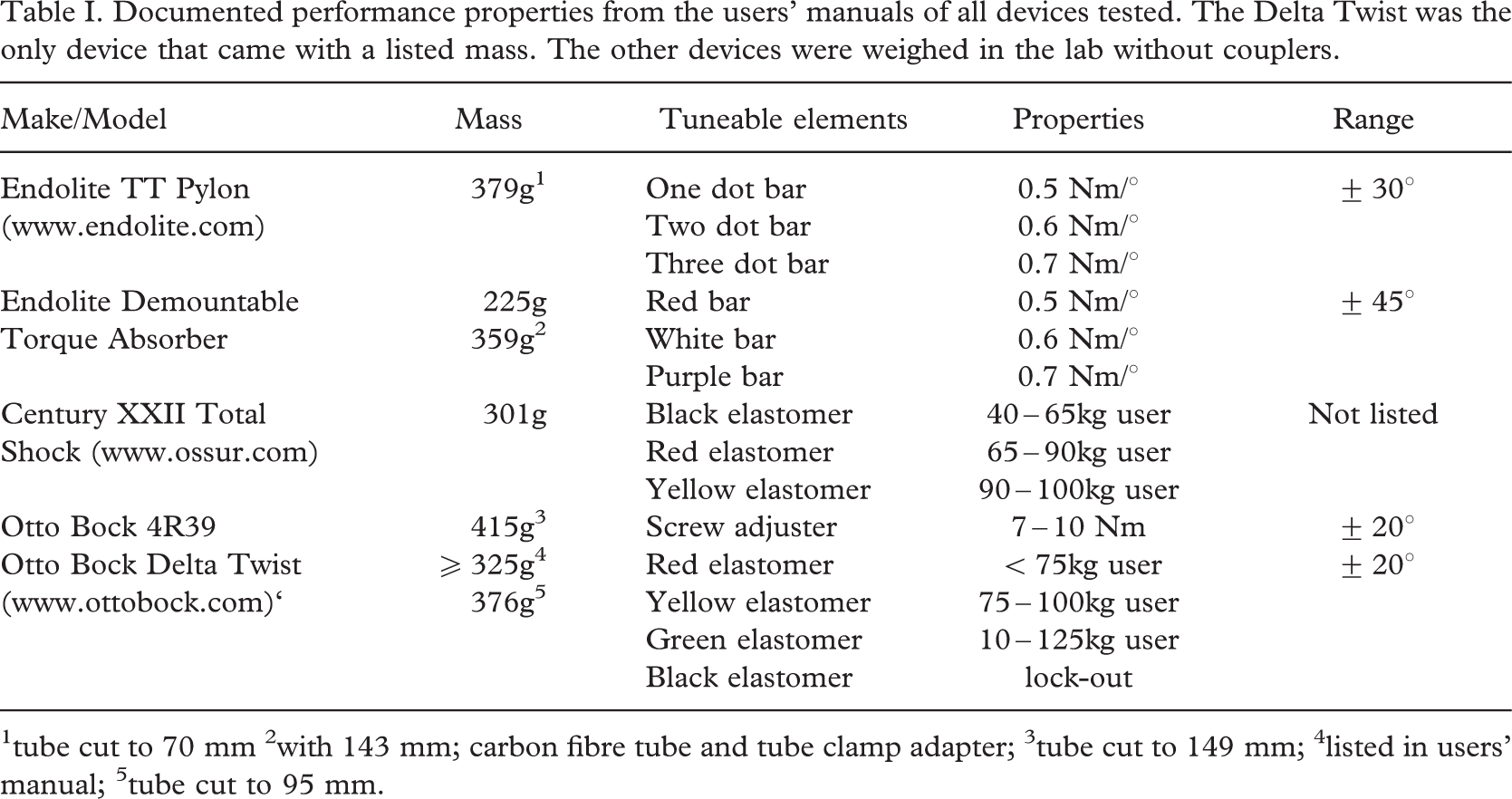
The average torque vs displacement curves for each subject over five trials were highly asymmetrical for all three conditions (Figure 2). The greatest torques were applied during stance in the direction of internal (positive) rotation. The general pattern is external rotation under small external torque post heel-strike to mid stance. At mid stance, the foot is relatively immobile in the transverse plane, but the torque reaches its maximum internal value. From mid-stance to toe-off, the torque declines, again with minimal angular displacement. During swing phase, the foot rotates internally back to its neutral orientation under no torque. The notable exception to this pattern is the inside-right foot (during right turns). In this condition, the foot angle changes at a more constant rate over the whole gait cycle. The ranges from the human data can be compared to the ranges of the TRAs, but the shapes of the loops cannot since the human subjects impose a different input time history. The average peak torques and maximum excursions during stance while turning are reported in Table II.
The mechanical test torque vs. displacement curves exhibited both linear and non-linear characteristics (Figure 3). All of the curves start at the origin and proceed in a clockwise direction. The Endolite TT, Endolite Demountable, and Century XXII Total Shock torque was nearly directly proportional to displacement indicating a linear response (Figures 2a, b and e). The Otto Bock Delta Twist and 4R39 torque increased rapidly at the initial position and at the extreme range of motion indicating a non-linear response (Figures 2c and d). The trials at the higher rotational velocity (608/s) and with axial loading generated plots nearly identical to the unloaded pseudo-static trials (data not shown).
Normalized Torque (Nm/kg) vs Displacement (8) for human subjects. Average data from five trials are presented for each subject. Each trace begins at the heel strike (arrow) and proceeds clockwise. Internal angles and torques are positive. 1a.) data taken from the right leg while subjects walked in a straight line 1b.) data taken from the outside left (OL) leg while subjects initiated right turns 1c.) data taken from the inside right (IR) leg while subjects initiated right turns. Additional data are not shown for clarity.
Mean Peak internal and external torques and angular ranges for human subject data. Each value is the mean of the three subjects. (Ti: internal torque, Te: external torque, range: jmax internal anglej + jmax external anglej)

The curves from the same manufacturers comprise a family of curves differentiated by the spring constant. Despite the narrower range, the Endolite TT pylon data lie on top of the Endolite Demountable TRA. These two TRAs also display the same nearly linear behaviour over the range of travel, but differ from the performance listed in the users' guide. Additionally, there is little performance difference between the different Endolite elastomers. The Otto Bock TRAs are likewise similar to each other but notably increase in stiffness towards the limits of the range and have high stiffness values near the neutral position.
Total energy lost and the percent of energy lost to friction are given in Table III. The total energy lost per cycle cannot be compared between adapters under this experimental design since each adapter was rotated through its maximum range. Adapters with larger ranges will have larger energy losses simply because the distance term in the energy equation is larger. The percent of total energy loss due to friction, however, can be compared since the method was the same for each adapter. The Endolite TT pylon had by far the highest percentage of energy loss due to friction with the rest of the adapters clustered around each other.
Discussion
This study establishes the baseline performance for TRAs from human subject testing and compares them to the mechanical behaviour derived from the MTS testing on currently available TRAs.
The main difference between human performance and TRA mechanical performance lies in the asymmetry of the physiological data. The maximum physiological range of rotation is 268 (Table II). However, the foot rotates internally very little beyond the angle at heel strike. Nearly all of the foot rotation occurs externally relative to the angle at heel strike (Figure 2). The physiological range of torques is also highly asymmetric, with higher internal torques for all activities. Internal torque ranges from 1.7 times greater than external torque for the left leg during right turns to 6.6 times greater for the right leg during right turns. During linear walking, this asymmetry persists, with internal torque 2.2x higher than external torque (Table II).
In order to accommodate the asymmetrical rotation, the device would need to rotate at least 268 externally from its angle during the swing phase. Other manoeuvres may necessitate more rotation or may involve more internal rotation from the angle at heel strike. All the adapters tested have equal rotation, both internal and external, relative to their resting position (where the device would be at heel strike). Given this, the necessary full range for the manoeuvres tested in this study would be 528 (twice the maximum external rotation of 268). If matching the physiological rotational range is the critical performance measure, then only the Endolite adapters meet the needs indicated by this study.
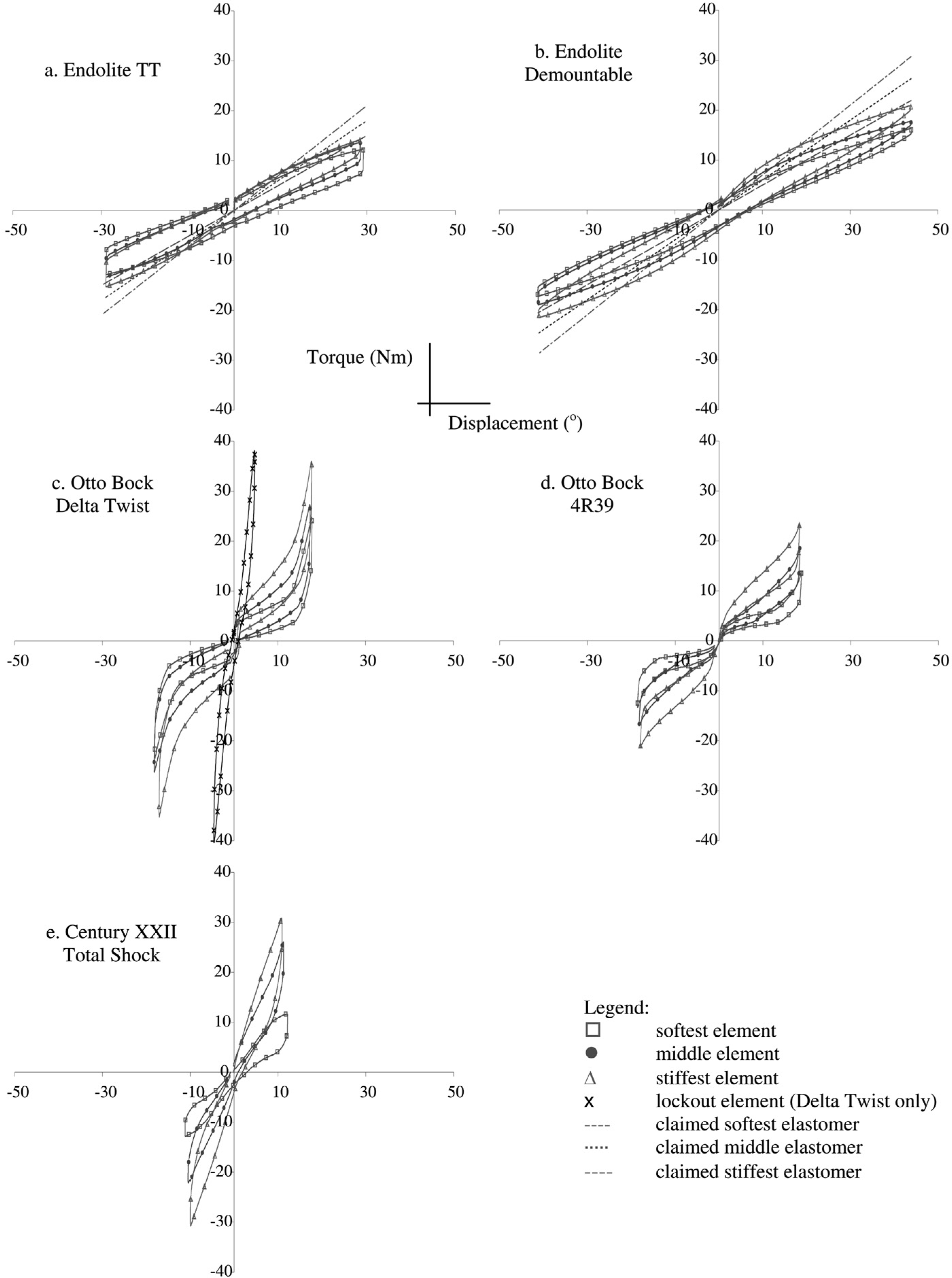
Torque (Nm) vs. Displacement (8) for all adapters and all elastomers. Each trial begins at the origin and traces clockwise.
Another performance measure is the adapters' response to the torque generated by the human subjects. It is important that the amputee never reaches the end of the rotation, at which point an abrupt stop and a torque spike would occur. The physiological mean peak torque is 11.8Nm internally. If this torque were applied to the adapters with the middle or stiffest elastomers installed, none would reach their maximum rotation. With the softest elastomers installed, the Endolite TT and the Century XXII reach the end of their rotation at that torque value. The Delta Twist allows for different elastomers on the internal and external sides of the adapter. This may be of value in matching the corresponding asymmetry in the physiological torque data.
Total energy loss per one complete cycle through the maximum range and the percent contribution of friction.
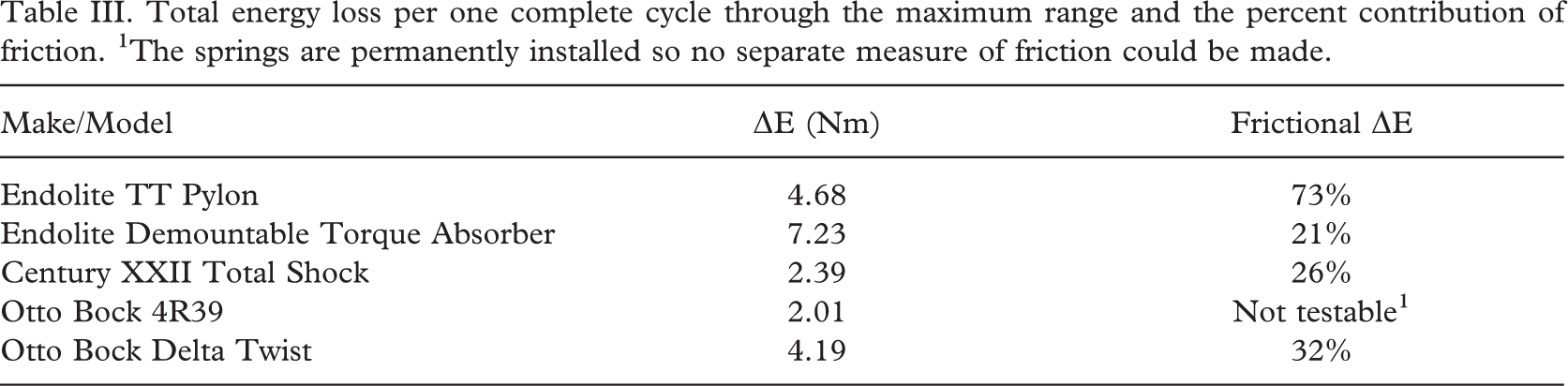
The springs are permanently installed so no separate measure of friction could be made.
The angle of the prosthetic foot in the transverse plane also affects the torque generated in the pylon. Transverse plane prosthetic foot alignment modulates transverse torque since the moment is generated from the instantaneous centre of pressure of the foot during stance. If the foot is angled externally, an environmental external torque will result (as will a balancing, subject generated, internal torque) due to the moment created as the foot contacts the floor. This effect is as yet unexplored, so it could not be included in this estimate of the actual rotation and torque required in a TRA.
The energy absorption values may also translate into tangible effects for the amputee. It is important to remember that the absolute energy lost is over the entire range of the device. Thus, devices with greater angular range will necessarily have greater energy losses at the same friction values. However, the higher the percentage of energy loss due to friction, the greater the resistance in the adapter to changes in direction. If the friction is sufficiently high, the motion will be stepped (resulting in a “sticky” feeling) since a minimum torque must be applied before the adapter begins to rotate. The MTS in this study was under displacement control, so the torque was always sufficiently high to keep the adapters rotating. Further tests under low torque would verify the presence or absence of stepped motion.
Several other conclusions can be drawn from the data that may be of interest to the prosthetist. Firstly, the Endolite adapters differ from the performance listed in the users' guide, and there is very little performance difference between the elastomers. Secondly, the non-linear (Otto Bock adapters) vs linear (all other adapters) profiles may have clinical significance. It is possible that increased stiffness near the ends of the range serves to help prevent an abrupt stop when the amputee reaches the end of the rotation. And lastly, the high stiffness values of the Otto Bock adapters around the neutral position (Figures 3c and d) may reject small moments and help to keep the foot centred in a neutral position with respect to the socket.
Conclusion
Data that describe the mechanical performance of prosthetic components create a structure for conversations between amputees and prosthetists. These data allow the prosthetist to interpret qualitative issues raised by the amputee and direct him/her to the correct rotation adapter and/or elastomer setup. While, for these reasons, this study will be helpful to prosthetists seeking the correct prescription for TRAs, it also points us in the direction of considering transverse-plane controllable rotation adapters. The patterns of torsion and torque generation from the human subject data illustrate not only the range of stiffness values, but also consistent changes in the hysteresis loop pattern with turning. Ultimately, the performance criteria of interest are the tissue shear on the stump and the ability to perform desired manoeuvres. The data from this study will be useful in addressing these criteria and in modeling a controllable TRA that can respond appropriately as the amputee manoeuvres within their environment.