
Abstract
Prior research involving persons with drug-resistant epilepsy has demonstrated that listening to some music decreases the probability of clinical seizures and their related comorbidities. This article reviews recent research designed to elicit the neural mechanisms behind positive outcomes on biomarkers of the disease. Using novel music analytical and neurophysiological experimental methods, our results showed positive effects on epilepsy using 15-second gamma-band (40-Hz) complex tones as well as Mozart's Sonata for Two Pianos in D Major (K448). We also observed greater effects with increased stimulus duration. Further analysis elicited effects localized to bilateral frontal brain regions due to transitions between musical phrases. Finally, music matched for patient preference from a range of musical styles was not as effective as 40-Hz tones or Mozart's K448. Understanding these results required expertise in both music and neuroscience, and could yield reliable music-based interventions for epilepsy that may also be transferable to other brain disorders.
Introduction
The propensity of music to play the body and the mind has been recruited for millennia to treat a wide range of illnesses and maladies. Early examples come from the ancient civilizations of China, India, Iran, Greece, and Rome, and music therapy notably flourished in the so-called Golden Age of Islam centred in medieval Baghdad. Such ancient therapeutic uses of music were often tied to myriad local forms of pre-scientific knowledge about music and healing nowadays generically gathered under the label of shamanism. Supported by public funding agencies and private foundations, an increasing number of researchers, physicians, and clinicians working in adjunctive therapeutic practices are conducting new evidence-based research on the healing powers of music and integrating tools and techniques that stem from traditional cultures and indigenous peoples as well as from Western music. However, the neural and physiological mechanisms that underlie music's medicinal effects remain elusive because scholars and practitioners around the world are separated by disciplinary and physical boundaries.
Despite this disparate knowledge, the growing field of music medicine has garnered increasing advocacy among neurologists, cardiologists, physiotherapists, psychiatrists, and psychotherapists for clinical use – either in parallel with or as an alternative to, pharmaceutical treatments and invasive surgeries. Music medicine includes interventions for chronic pain (Garza-Villarreal et al. 2017), anxiety (Ainscough, Windsor, and Tahmassebi 2019), burnout syndrome (Fares et al. 2016), post-traumatic stress disorder (Baker et al., 2018), depression (Aalbers et al. 2017), autism spectrum disorders (Sharda et al. 2019), dementia (Baird and Samson 2015), motor disease (Thaut et al. 2019), heart disease (Chew, Orini, and Lambiase 2021), and many other conditions. But how do we know which music will be effective? Can music's effects be isolated and measured separately from pharmaceutical, psychodynamic, and the other components of multi-faceted treatments? The gold standard in medicine is the Randomized Controlled Trial (RCT), clinical experiments with random assignment of treatment and controls (placebos) to measure the extent of effects due to music versus other non-musical factors. Although there has been much progress in the design and documentation of RCTs for music medicine, the consensus from scientific reviews is that more are needed to catalyze widespread adoption of music medicine (McFerran et al. 2020).
Knowing if music will help in a given situation means being able to predict when, and how, specific sites in the body and brain will respond beneficially, and which combinations of musical features, musical works, and personal traits will elicit those responses. Gathering the necessary expertise to acquire such knowledge requires collaboration between practitioners in the arts and sciences, blending disciplines that on the surface do not ordinarily share languages, experiences, or perspectives. However, despite the oft-cited rifts between arts and sciences (Bill 2018), and as evidenced by numerous books and memoirs recounting personal experiences in music and medicine, many physicians and scientists are themselves musically proficient, and highly-accomplished musicians are often proficient at, and many are professionals in, mathematics and the sciences. Ultimately, connecting these seemingly distant domains enables new generations of practitioners and thinkers to join forces in the search for music to treat disease.
Engagement and entrainment
As a team of composers, data scientists, neurologists, and neuroscientists, our work brings together expertise in multiple perspectives to investigate how sound and music affect us and to discover new knowledge about the neural underpinnings of music effect and affect. Two complementary neural processes that are of particular interest in our work on music medicine are physiological entrainment and emotional engagement. Physiological entrainment effects arise from synchronization in the firing of neural circuits in different sites of auditory perception and cognition, including during the processing of musical features such as rhythm, tempo, dynamics, harmony, melody, timbre, and form. Neural correlates of many of these features have been mapped to wide-scale brain networks, including temporal, parietal, cingulate, and prefrontal cortices (Vierling-Claassen et al. 2008; Adaikkan et al. 2019; Thaut et al. 2019; Adaikkan and Tsai 2020). Emotional engagement, or music affect, is known to be modulated by personal traits, such as familiarity, preference, and autobiographical memories (Janata 2009), and it is generally considered to be processed by the brain's medial prefrontal and limbic regions (Tillmann, Janata, and Bharucha 2003). Understanding these neural correlates of musical experience, and how they interact, can lead us to new insights into the use of sound and music in medicine.
The origins of emotional engagement with and entrainment to music may be traced back to antiquity. At the beginning of his seminal book The Tuning of the World (Schafer 1977), the late R. Murray Schafer cites two Greek myths representing Dionysian (i.e. intuitive, emotional, right-brain), and Apollonian (i.e. analytical, logical, left-brain) views on the origins of music:
Pindar's twelfth Pythian Ode tells how the art of aulos playing was invented by Athena when, after the beheading of Medusa, she was touched by the heart-rending cries of Medusa's sisters and created a special nomos in their honor. In a Homeric hymn to Hermes an alternative origin is mentioned. The lyre is said to have been invented by Hermes when he surmised that the shell of a turtle, if used as a body of resonance, could produce sound. (Schafer 1977)
Athena's empathy towards the pain of loss describes emotional engagement with the voices of others. On the other hand, Hermes’ discovery of the acoustical fact of resonance reveals a physical property of voices and musical instruments which, when transduced via biophysical coupling, may result in physiological entrainment – synchronized firing of neurons to specific sonic frequencies. These proclivities cooperate so that conscious engagement with others’ vocal utterances – the music of the voice – also recruits frequency-following responses and rhythmic entrainment in the early stages of auditory neural processing (Coffey et al. 2021; Thaut, McIntosh, and Hoemberg 2015). The process of physiological entrainment feeds higher-level networks of language, cognition, sensory integration, and music understanding, which are sites of the neural correlates of social and emotional engagement (Huron 2006).
Music and physiology
Music vitalizes us, promoting increasing arousal of physiological systems such as heart rate, the concentration of stress hormones such as cortisol, secretion of endorphins (the body's own morphine), blood pressure, blood coagulation, and even activity in the immune system (immune globulins) (Khalfa et al. 2002). Conversely, other studies demonstrate physiological effects of music that can promote relaxation: decreasing heart rate, the concentration of stress hormones such as cortisol, blood pressure, and increasing heart-rate variation, which is correlated with the relaxed state of the autonomous nervous system known as vagal tone (Khalfa et al. 2003).
Given this wide range of physiological effects that can be measured in response to music exposure, how can we harness them for specific medical ends? The following sections describe the selection and development of musical stimuli for the treatment of epilepsy and experiments that aim to understand the mechanisms behind the observed positive benefits of music.
Auditory neurostimulation for epilepsy
Globally, more than 20 million people suffer from drug-resistant forms of epilepsy. In the US alone, care and treatment of epilepsy and associated convulsion diagnoses result in aggregated costs of more than $2.5 billion. A growing body of research seeks to identify promising and effective alternative therapies for patients that exhibit refractory epilepsy, ranging from nutritional interventions to biofeedback and more recently to music. If listening to music reduced the effects of epilepsy, both during and after stimulation, then this would be a discovery that can be easily implemented at low cost to augment medical treatments. Despite the findings that a few musical works and some specifically designed tones show promise as forms of non-invasive, non-pharmacologic epilepsy treatment, progress in the field has been impeded by a lack of fundamental understanding of the neural correlates of the musical features of effective stimuli.
Both EEG brain data and audio stimuli are expressed as digital signals representing electrical and acoustic time series, respectively. Computational techniques for both music and brain signals are used in the studies described below to pinpoint the effects on the brain of specific acoustic features – such as a tempo of 137 bpm played on a piano – and higher-order structural organization of music – e.g. sonata form vs song form. The results of the prior published studies discussed below show that music holds promise for augmenting epilepsy treatment – via low-cost smartphone-based listening programmes, for example – which would widen access to affordable treatments globally.
The gamma effect
Iaccarino et al. (2016), publishing in the journal Nature, discovered that pulsed light presented to mice with induced Alzheimer's disease reduced the presence of amyloid plaques – a biomarker of Alzheimer's disease – in the visual cortex (Iaccarino et al. 2016). Programmable LEDs were pulsed at different frequencies, and when pulsed at the specific frequency of 40-Hz, but not other frequencies, reductions in amyloids were observed. 40-Hz is within the frequency range known as the gamma band in electro-neurophysiology. After treating the mice for an hour a day for seven days, this gamma effect was shown to reduce plaque and free-floating amyloid. In a follow-up study using sound as well as light, gamma auditory stimulation at a frequency of 40-Hz was found to improve cognition in mice with induced Alzheimer's, and when combined with 40-Hz light pulses was found to significantly reduce Alzheimer's-associated pathology, namely widespread reduction of amyloid plaques, throughout neocortex (Martorell et al. 2019).
Subsequently, our groups at Dartmouth College in the USA began experimenting with auditory neuromodulation using 40-Hz gamma frequency to determine its effects on epilepsy, this time in humans instead of mice. Light was not used in our studies because of the significant risk of patients having reflex, or photosensitive, epilepsy (Fisher et al, 2005). In contrast to the experiments with mice, a positive effect was again observed when stimuli were delivered via sound only, the details of which are described below. This preliminary result suggests that gamma-band audio frequencies could potentially be used as auditory neurostimulation for non-invasive treatment of epilepsy, and, possibly, other neurological disorders too (Quon et al. 2021b).
The study cited above was the first to examine the influence 40-Hz auditory stimulation has on interictal and seizure activity. There are precedents in the neurology and neuroscience literature for the hypothesis of an auditory gamma effect on neuro-physiology. Previous work using 40-Hz stimuli showed that groups of neurons can be modulated to fire at a similar frequency (Adaikkan and Tsai 2020). Gamma entrainment, therefore, shows promise as a non-invasive treatment for refractory epilepsy which temporarily alters neural activity (Meisenhelter and Jobst 2018).
Interictal epileptiform discharges
One of the neural characteristics of persons with epilepsy is the presence of interictal epileptiform discharges (IEDs). IEDs are electrical spikes measured with electroencephalography (EEG) that arise from the brief, synchronous firing of neural populations that are typically involved with epileptic networks (Ayala et al. 1973; Gotman 1991; de Curtis and Avanzini 2001). These epileptic biomarkers are associated with seizure frequency and impaired cognition (Holmes and Lenck-Santini 2006; Holmes 2014). Furthermore, reductions in the number of IED spikes correlate with fewer seizures and improved cognition (Horak et al. 2017; Kleen and Kirsch 2017). Conversely, suppression of IEDs is also associated with improvements in those functions, and so IEDs are correlated with negative impacts of this disease. Hence, interventions that can suppress IED activity are considered to be effective neurological treatments (Quon et al. 2021a) (Figure 1).
Interictal epileptiform discharge (large spike) present in one channel of intracranial electroencephalography (ECoG) of a person with epilepsy.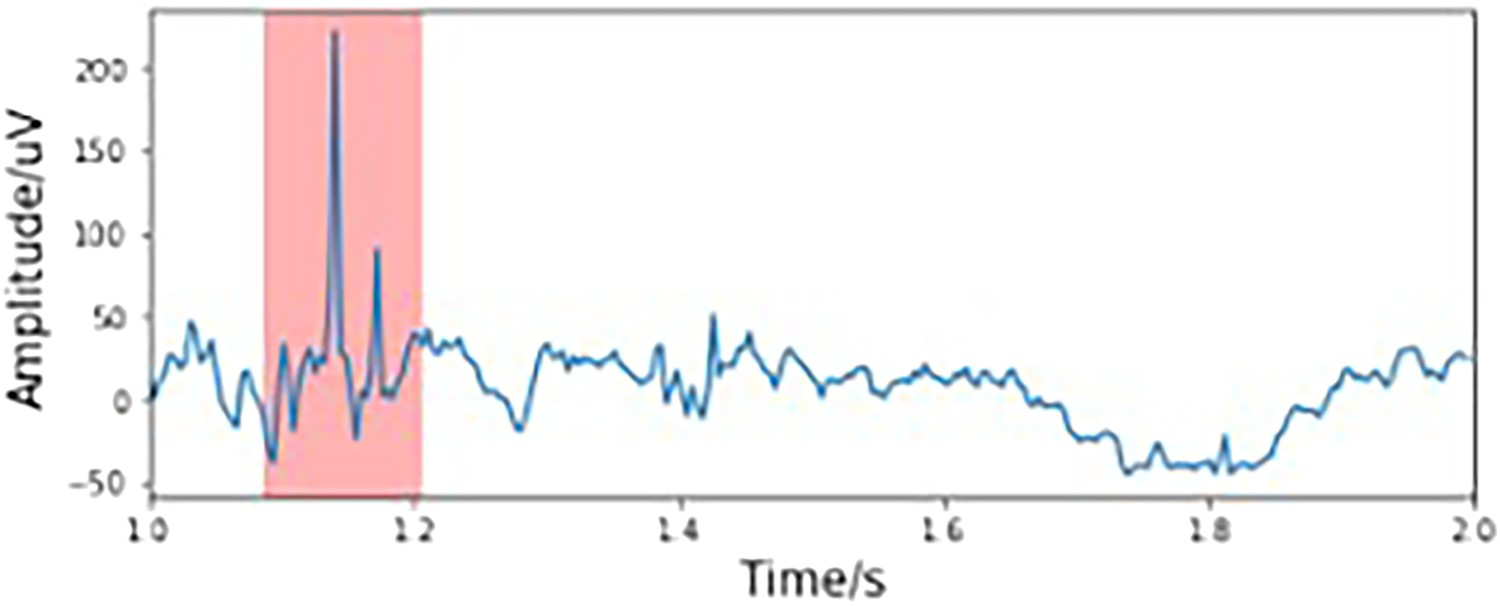
In the experiments discussed below, automatic detection of IEDs was performed using a pattern-matching algorithm that was trained on a human-expert annotated database of thousands of IEDs (Quon et al. 2021a). Once the algorithm was trained, performance on the detection of new IEDs with new patients was determined to be close to that of manual human annotation. Thus, the automatic detector was used to determine which among a range of auditory stimuli were effective at reducing IEDs, both during and after stimulus presentation, and how large of an effect was produced.
Experiments using auditory neurostimulation
The experiments described here and in the following sections were conducted by members of the Epilepsy and Cognition Lab at Dartmouth-Hitchcock Medical Center and the Brain, Emotions, and Affective Sound (BEAtS) Lab at Dartmouth College. The team members comprised undergraduate students, graduate students, post-doctoral researchers, technical staff, and faculty in clinical neurology, music theory and composition, computer science, and physics. The research was managed by weekly meetings, with overlapping participation between groups.
Summarizing (Quon et al. 2021b), eight persons with refractory (drug-resistant) epilepsy participated in a preliminary experiment at Dartmouth-Hitchcock Medical Center during 2018 to determine if there were positive effects of auditory neurostimulation on IED rates. Participants were patients undergoing intracranial electroencephalography (ECoG) monitoring and they had been surgically implanted with electrodes matching their treatment needs before being transferred to the monitoring facility. During monitoring, participants were asked if they would like to participate in a listening experiment. Those who agreed heard many 15-second sound clips, each followed by 15 s of silence. The clips were presented using a portable powered speaker that was placed in front of the patient on an over-bed hospital table and adjusted to a comfortable listening level before the start of the experiment.
The test stimuli for the first analysis consisted of 15 s samples of a 40-Hz tone and a 440-Hz tone. Two other test stimuli were also presented in the same listening sessions: Mozart's piano sonata in D Major for two pianos, which was motivated by prior work in using music for the treatment of epilepsy further discussed below, and the same Mozart recording altered by amplitude modulation with a 40-Hz sinusoid using signal processing software written in Matlab. While the effective frequency response of the speaker was within the desired range for three out of four of the test stimuli, the 40-Hz sinusoid stimulus was not expected to be reproduced by the speaker at sufficient volume due to the large difference in the diameter of the speaker cone (12 cm) and the wavelength of sound in air at 40-Hz (857.5 cm). Hence, the 40-Hz stimulus was presented at a greater amplitude than the other stimuli which produced distortion in the speaker and introduced harmonics of the 40-Hz pure tone. Thus, the presented stimuli was a complex tone with a 40-Hz fundamental frequency and harmonics, see Figure 2.
log-frequency spectrogram of 1 min of the 40-Hz stimulus as recorded through the Roland Cm-30 portable powered speaker used in the gamma auditory neurostimulation experiment. Note the presence of harmonics which serve to reinforce the 40-Hz fundamental.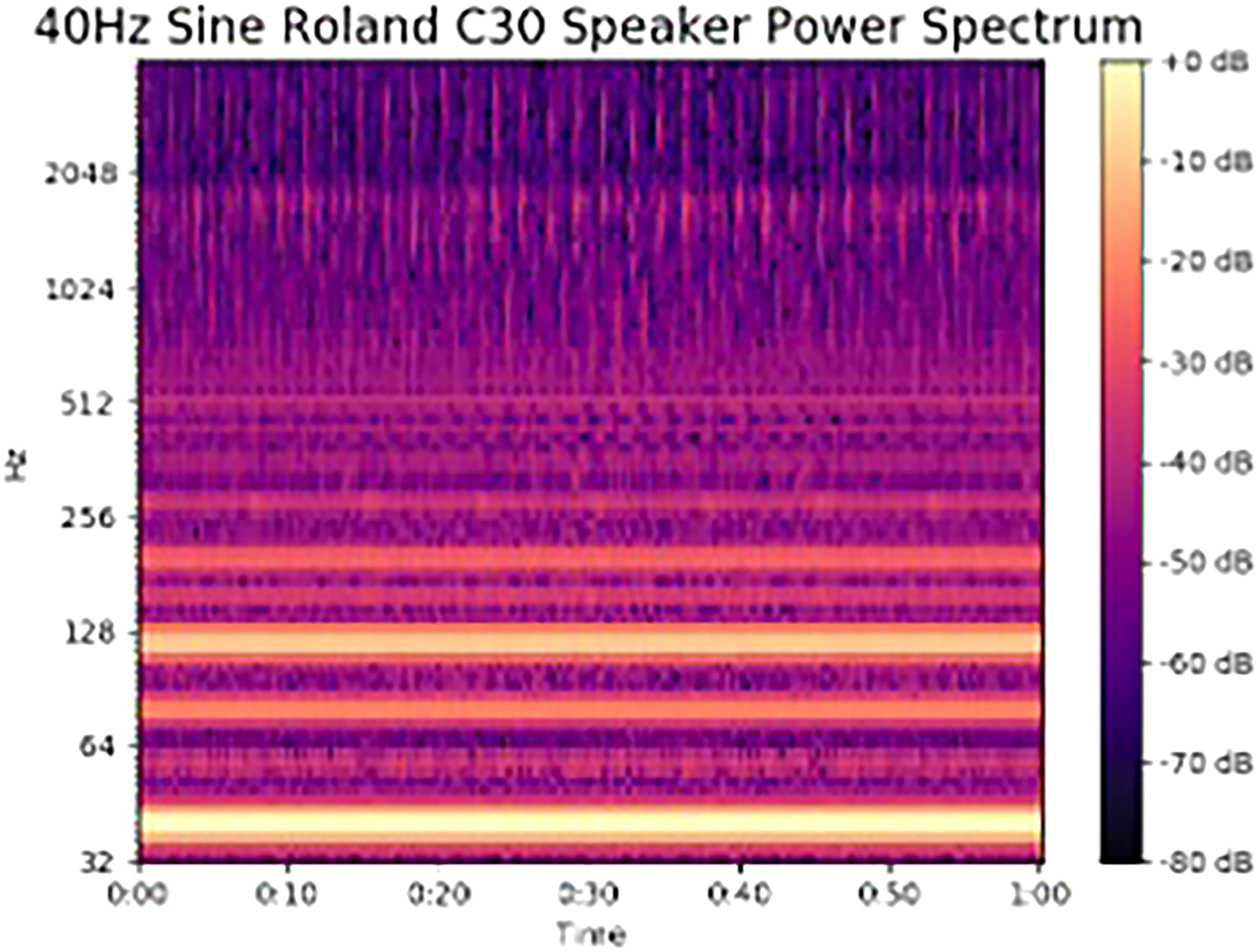
Each participant completed 80 randomly ordered trials consisting of two listening sessions of 10 trials for each of four different stimuli. Therefore, each stimulus was presented 20 times in two testing sessions, for a total stimulus duration of 10 min each with a total interleaved resting duration of 10 min for each of the stimuli. ECoG data were recorded, via each participant's implanted electrodes, synchronously with all the stimulus presentations for subsequent analysis of the IED rates during exposure to each of the stimuli. The data collected during the experiments were later analyzed, using the automated IED detection method described above, to test the following hypotheses: (H1) exposure to the 40-Hz auditory stimuli induces participant-level reductions in IED rates compared to the control periods; and (H2) localized brain regions would be significantly associated with IED rate alterations observed during exposure to the auditory stimuli.
Results of 40-Hz auditory neurostimulation
For analysis purposes, participants’ baseline IED rates were calculated, and subsequently, they were divided into two groups corresponding to high-baseline (4 participants) and low-baseline (4 participants) IED rates, determined by a cut-off threshold. The threshold was defined by the participants’ mean baseline IED rate, which was approximately 1.23 IEDs per minute. This pre-analysis clustering was performed to minimize the effect of spurious events in low count data, which would otherwise disproportionately affect the statistics.
The 40-Hz auditory tone yielded a significant positive response with the high baseline IED rate group during exposure. The four participants in this group experienced an average of 35.25% reduction in the probability of IEDs during stimulus presentation. There was no significant effect with the 440-Hz tone. This difference in effect, between the two frequencies, indicates that low-frequency stimulation (in the gamma band) yields an effect whereas higher-frequency components did not yield benefits, at least with short-duration stimuli (15 s). Across participants, significant IED reductions were generally localized to lateral and medial temporal brain regions, with partial overlap with the participants’ seizure onset zones.
Discussion
This work was the first to specifically examine the influence of 40-Hz auditory stimulation on IED rates in epilepsy, and the findings corroborate the results of past studies using gamma audio and visual stimulation with other conditions such as bipolar disorder, schizophrenia, stroke, and, most commonly, Alzheimer's disease (Oda et al. 2012; Roach et al. 2013; Adaikkan et al. 2019; Martorell et al. 2019; Zheng et al. 2020).
One of the main theories for the neural basis of the 40-Hz effect is that the frequency corresponds to the rate at which excitatory and inhibitory regulation of cortical pyramidal cells is synchronized by GABA interneurons (Buzsáki and Wang 2012; Vierling-Claassen et al. 2008). Disorders in the firing of these interneurons are associated with the dysregulation of epileptic networks (Yizhar et al. 2011). While other frequencies have been used in prior experiments, 40-Hz appears most effective at improving dysfunctional timing in the regulation of cortical structures (Liu et al. 2019).
The Mozart effect
For more than two decades, neurology research has demonstrated that listening to specific pieces of music, mostly by Mozart, yields benefits to patients with epilepsy. These studies repeated an effect, originally discovered by Hughes et al. (1998), that was observed in patients listening to Mozart piano sonatas K448 and K545, which were found to reduce markers of epileptic activity in their brainwaves during and after listening (Lin et al. 2012). Several repeat studies have since demonstrated a therapeutic reduction in seizures and related abnormal brain activity due to K448 and K545 stimulation. Further reinforcing these discoveries, a meta-analysis demonstrated that approximately 84% of participants in the reviewed studies exhibited significant reductions in epileptic brain activity while listening to Mozart's K448 (Sesso and Sicca 2020) (Figure 3).
Score of the opening of Mozart's Sonata for Two Pianos in D Major (K448) showing the introduction and beginning of the primary theme as performed on two pianos.
The so-called Mozart effect was first introduced by Rauscher, Shaw, and Ky (1993) in an article describing enhancement on a spatial task during exposure to K448. Subsequently, there was much interest in using Mozart, especially for children's education. However, Steele et al. (1999) highlighted failures to repeat the Mozart effect on the same tasks that Racuher et al. had reported, citing methodological and interpretative errors, and they concluded that there was no measurable benefit, prompting the authors to conclude that ‘a requiem is likely in order’. Enthusiasm for Mozart's music as a pedagogical panacea subsequently waned. However, in an act of resurrection, Hughes et al. (1998) and Jenkins (2001) demonstrated the Mozart effect again, but this time in patients with epilepsy using electroencephalography to demonstrate observable changes in brain function. Interest in the Mozart effect resurged, and numerous publications repeated the findings that exposure to a few works by Mozart produced measurable benefits in populations of neurology patients. At this time, established hypotheses for the K448 effect include activation of brain regions implicated in reward and emotion (Blood and Zatorre 2001; Huron 2006) and specific arrangements of acoustic features, such as the ratio of lower to higher harmonic frequency components and the presence of interference between low-frequency harmonics, as candidates for the mechanisms behind the effects (Štillová et al. 2021; Lin et al. 2010).
Despite all of these studies, only one previous study examined the ‘Mozart effect’ in an adult population using higher-quality, less noise susceptible intracranial recordings (Tao et al. 2007). To test the effect of Mozart's piano sonatas, the above experiment included Mozart's K448 as one of the stimuli. This was included to see if the prior reported effects could be replicated using surgically implanted intracranial EEG (ECoG) versus scalp EEG as in the previous studies. A further hypothesis to be tested was that 40-Hz modulation would increase the effect. So the modified version of the K448 stimulus was also used in the experiment, amplitude modulated with a 40-Hz sinusoid as described above.
Results of Mozart auditory stimulation
The unmodified K448 stimulus yielded significant reductions during exposure to two of the four participants with high baseline IEDs, yielding an average 40.50% reduction in IED rates. IED rate alterations were not significant when using stimuli altered with amplitude modulation. The negative result for K448 modulated with 40-Hz indicates that the distortions introduced by embedding the modulation served to reduce the effectiveness of both 40-Hz and K448 alone for short-duration stimuli. The modulated stimulus method introduced distortions to all frequency components in the original K448 recording, including inharmonic distortions, which may have distracted participants from listening to the music.
Experiment with longer stimulus duration
The difference between music and 40-Hz effects in the above experiment may be explained by the use of short 15-second clips, as there was likely insufficient exposure within each clip for the music to activate entrainment or engagement. Previous studies using scalp EEG had used much longer stimulus durations averaging eight minutes (Lin et al. 2014; Sesso and Sicca 2020; Bodner et al. 2001). This motivated a follow-up ECoG study using music clips with 90 s duration in which we tested the following hypotheses: (H1) the ‘Mozart effect’ would be dependent on a longer stimulus duration; (H2) the effect would extend to regions outside of the primary auditory pathways, owing to past observations of music and its involvement with higher-order systems, such as emotion circuits and mirror neurons (Molnar-Szakacs and Overy 2006); and (H3) musical form is a factor in suppressing IEDs via processes of emotional engagement recruit the brain's anticipation and reward systems which are known to be active in listening to music (Cheung et al. 2019).
In the analysis phase, the 16 participants were stratified into two groups based on whether they received 15 s or 90 s of Mozart's K.448. For clarification, we combined data from experiment 1 (8 patients) and experiment 2 (8 patients) performing the same group-level statistical analysis for each group independently. The results of longer duration exposure showed a 66.5% average global IED reduction with the K448 stimulus with exposures from 30-seconds to 90-seconds, a greater effect than observed with the 15 s clips. Moreover, the IED reductions began after at least 30-seconds of exposure and were maximal during the last 30 s, showing that the effect changed over time.
Musical phrase boundary effects
The music-theoretic concept of musical structure describes listeners’ segmentation of auditory information into nested hierarchical units of various sizes (Lerdahl and Jackendoff 1983). In principle, this organization is similar to human language, where speech is nested recursively into units such as phonemes and words, which are, in turn, nested into phrases and sentences. Correspondingly, music consists of notes, chords, themes, and higher-level functional units such as phrases and sections (Collins and Schmuckler 1997) which occur at quasi-periodic intervals and are marked by significant changes in melodic theme, harmony, rhythm, and key (Chiappe and Schmuckler 1997). These higher-level compositional elements underlie emotional engagement with music and are experienced as anticipation of upcoming events, which is rewarded by dopamine release when expectations are violated in pleasurable ways. Prior studies have reported that violation of expectations can induce strong emotions (Steinbeis, Koelsch, and Sloboda 2006). Furthermore, as pointed out by Huron (2006), an unexpected but seemingly innocuous event may result in anticipatory failure but generate positive emotions, known as the reaction and appraisal responses. Thus, phrase-level structural components are primary functional units in the cognitive processing of music.
These processes of expectation and expectation-violation are maximal at phrase boundaries, where abrupt changes in harmony, melody, dynamics, timbre, note density, and texture mark the transitions to new material. The neural correlates of predictive engagement with music have previously been observed to reside in the prefrontal cortex, and the emotional responses they elicit reside in the limbic system. Evidence for the relationship between music and frontal emotion networks is provided by Tillmann, Janata, and Bharucha (2003) fMRI study, which showed enhanced activation of the bilateral inferior frontal regions for unexpected targets. More specifically, the structural syntactic relations between musical events led to increased bilateral frontal activation, where greater activation was correlated with processing incoherent, unexpected events (Tillmann, Janata, and Bharucha 2003). Arjmand et al. (2017) augmented these findings by showing that unexpected changes in musical features, such as intensity and tempo, activated frontal brain regions linked with positive emotional responses. This suggests that the generation of neural predictions about musical features may depend on both the duration of exposure and transitions from prolonged segments within the musical stimulus–as this may be driving enhanced activation of emotion networks regulated by frontal cortices. The following analysis of the ECoG data from the long-duration experiment sought to understand interactions between music structure and the activation of emotional brain networks.
To determine if the changes in brain activity over time could be related to changes in the music, i.e. the musical form, an analysis of K448 was performed in which the temporal locations of phrase boundaries were annotated manually, by a member of the music faculty in the group, and also using an automatic audio music structure extraction algorithm by McFee and Ellis (2014). The two annotations were compared and their substantial agreement was verified. Although the music was an instance of the classical sonata form, the duration of the clip covered only the ‘exposition’, omitting the canonical repeat of the exposition, the development section, and the recapitulation. Within the exposition, nine phrase boundaries were determined, including the introduction, main theme, variations on the main theme, a prolonged transition section, the second theme, return to the main theme (in the dominant key), and, finally, the coda. As such, the sections were of substantially different durations ranging from 4 s to 30 s (Figure 4).
log-frequency spectrogram of the first 90 s of Mozart's Sonata for Two Pianos in D Major (K448) showing structural annotations provided by expert analysis.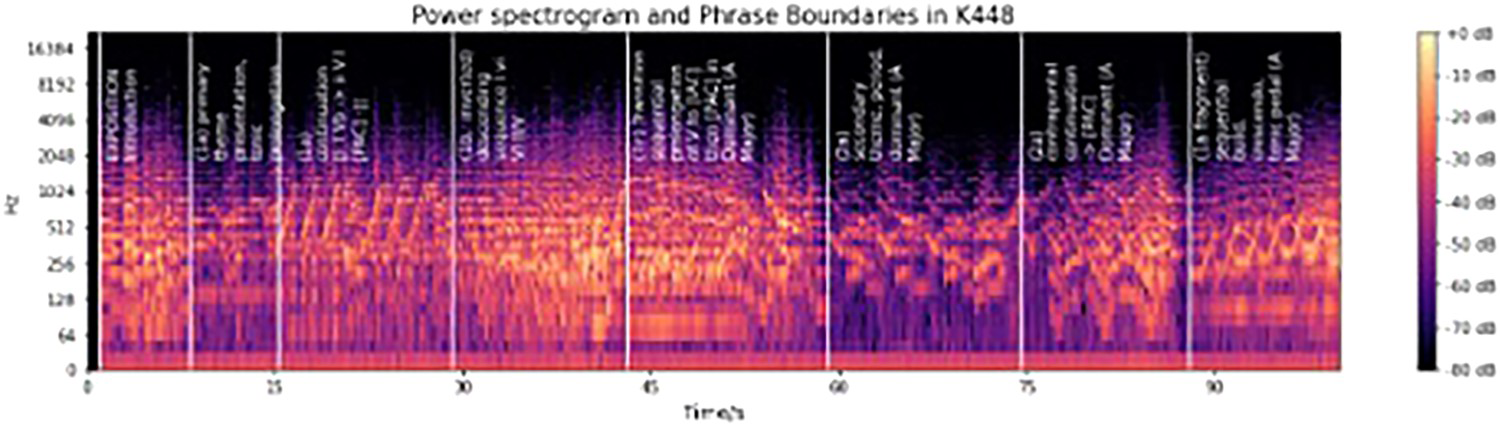
The spectral power of the neural ECoG response to auditory stimulation was calculated in canonical frequency bands: delta (2–4 Hz), theta (4–7 Hz), alpha (8–12 Hz), beta (12–30 Hz), gamma (25–40 Hz), and high gamma (40–100 Hz). As such, this was the first analysis in the literature to systematically evaluate the relationship between musical segment boundaries and spectral power changes related to music listening effects in persons with epilepsy.
Analysis of IED rates during the different phrases within the musical form showed that the effects were localized frontally with an average of 62% IED reduction in bilateral frontal cortices. Correspondingly, transitions after long K448 phrases increased theta activity (4–7 Hz) in frontal brain regions also. Bilateral frontal areas have previously been associated with the cognition of higher-order structure in music, so the increased activity after longer phrase boundaries is likely to be associated with expectation violations of harmony and melody, as those are the locations within the musical form where the music changes the most, hence prediction-errors would be maximal. The frontal powerband increase was not observed during transitions from shorter musical segment boundaries and during all transitions within the filtered version of K448.
This agrees with past observations that listening to music was associated with increased activation of prefrontal cortices, such as Mansouri et al. (2017) observation that high-tempo music activated prefrontal cortical areas, while transcranial direct current stimulation (tDCS) over prefrontal regions negated the influence that music had on executive functions. These current findings also agree with Rauscher, Shaw, and Ky (1993) original observation that K448 enhanced spatial–temporal working memory, a process directly linked with dorsal frontal activation.
Finally, the results are also concordant with past music research, which demonstrated that pleasant music was associated with increased frontal theta power (Sammler et al. 2007; Bekkedal, Rossi, and Panksepp 2011; Knyazev 2007; Chabin et al. 2020). Some of these previous studies further proposed that frontal theta oscillations may be associated with activation of the limbic system in response to emotionally arousing musical stimuli.
That the musical structure of K448 may be contributing to a therapeutic effect implies that the sonata form itself may elicit positive emotional responses important for anti-epileptic effects. This is further supported by past observations of another composition with verified anti-epileptic properties, Mozart's Piano Sonata in C Major, K545 (Lin et al. 2014). However, in addition to musical structure, we also revealed the importance of other musical features, such as the stimulus's frequency components. This was supported by our finding that the filtered version of K448 failed to elicit a therapeutic response. Despite similar broad structural components, the filtered version of K448 may have decreased emotional salience (i.e. frequency distortions made it less acoustically pleasurable), resulting in a reduced likelihood to develop internal musical predictions and engage emotionally with the piece.
A follow-up analysis, using event-related potentials (ERPs), demonstrated that note onsets and phrase boundaries elicited distinct neural responses, with three temporal clusters at −150, 200, and 450 ms relative to the stimulus markers showing significant differences in the majority of sessions. The correlation between musical expectations and emotion (Huron 2006) supports our observations of such differences in the neural signals. The two post-stimulus components could be potentially explained by a violation of melodic expectations. The −150 component unique to the processing of higher-level structures suggests a potential prediction response (Huron 2006) which describes the effect of positive emotions resulting from anticipatory success and has been commonly overlooked in earlier studies of phrase boundaries. During the exposure to music, listeners gradually learn the information dynamics of the music and are able to predict forthcoming phrase boundaries, due to changes in note density, melodic themes, key, tempo, and rhythm. The neural representations leading to correct predictions are strengthened and reused. These pleasurable responses to phrase boundaries are also related to reward and increased activity in the frontal lobe.
Beyond Mozart
Why Mozart? And why only piano sonatas K448 and K545? Have other musical works been found that are effective in the treatment of epilepsy? One explanation for the Mozart effect could be selection bias. As noted above, many physicians are musicians. This is reflected in high rates of musical training in admitted medical school applicants. A majority of these students’ prior musical education was in classical Western traditions, with a predominance of singers, pianists, and violinists. Would music selections for medical interventions be different if, instead or in addition to classical music, those students had studied jazz, R&B, country, folk, and pop?
Further studies attempted to elicit the effect with musical works by other classical composers and in other musical styles, but to this date, K448 and K545 have remained the only anti-epileptic music selections that have been verified by repeated experiments (Sesso and Sicca 2020). Several studies tested music by Glass, Bach, Beethoven, Chopin, and Liszt. A non-classical exception was Yanni, but even in this latter selection the use of synthesized strings and piano is reminiscent of the sounds of classical music. These studies generally failed to demonstrate an effect for the alternative music choices, and none of the works purported to have produced an effect have been successfully verified by repeated experiments. Why are there so few, or possibly no other works that have been discovered to be effective? What are the characteristics of music stimuli that are effective?
We used alternative music selections in the experiment with longer stimulus durations described above. In addition to the original Mozart K448 and K448 modified with 40-Hz amplitude modulation, we created a search algorithm to match songs in a database that were thought to be convergent with the acoustic characteristics of K448, but in different genres: Ambient Music, Classic Country, Heavy Metal, Non-Western, and Rock-N-Roll. Participants were asked to select a ‘preferred’ genre that would be included in their playlist, along with Mozart K448 and its amplitude modulated version. Each genre consisted of two songs truncated to two-minutes duration. The first song was convergent with specific acoustic properties of Mozart K448 and the second was maximally divergent.
Hence, our study combined three approaches for determining whether music is beneficial for persons with refractory epilepsy. Our first approach was to use an audio-similarity search algorithm, matching songs from a range of genres to a specific acoustic property of Mozart's K448. This approach was based on our observations, and previous reports, of the benefits of Mozart's K448 piece for persons with epilepsy. If validated, then we would be able to use this algorithm to create personalized music playlists for each patient in a newly defined ‘anti-epileptic’ genre. Our next approach was to modify any piece of music by boosting lower frequency harmonics, with this boost centred at 40-Hz. This approach was based on previous findings that gamma entrainment (40-Hz) was beneficial for a variety of neurological disorders, including epilepsy, and as shown in our previous music study which also provided support for this beneficial property by showing a reduction in IEDs. If validated, we could then use this approach to make any piece of music ‘beneficial’ for persons with epilepsy by embedding gamma amplitude modulation. Finally, we sought to evaluate if a participant's emotional connection to a specific piece of music was driving these beneficial responses by asking participants to select their most preferred song from a list of options.
For the search algorithm, the acoustic property that we selected for comparison was the amplitude modulation spectrum (Shamma et al. 1993). This feature was motivated by both the neurophysiology of hearing, in which the modulation spectrum is tracked by neurons in the thalamus with maximum selectivity for modulations in the gamma band, and the theory that the Mozart effect for epilepsy is due to interactions between low-frequency harmonic components–which would result in amplitude modulation, or beating, between harmonics. Convergence with K448 was determined by calculating the average modulation spectrum for each song in the database and performing a Mann–Whitney U-test between the song and Mozart K448. The maximally convergent song in each genre, according to this statistical divergence measure, was selected for testing, as well as the maximally divergent song to be used as a control. All song selections were also matched to the average tempo for their genre so that there was minimal difference in tempo between the convergent and divergent selections in each genre.
Despite selecting songs from a range of genres with acoustic features that were matched to Mozart K448, and matching genres to participants’ preferred genre as well as offering a boosted version of each song selection with 40-Hz embedded amplitude modulation, none of the preferred or boosted stimuli were effective at reducing IEDs. Only Mozart's K448 and the 40-Hz tone were found to have a positive effect during the stimulus presentations. This was a somewhat perplexing result because the music selections had spectral acoustic features in common with Mozart.
What might the reasons be for the highly specific nature of the re-verified Mozart effect for epilepsy? Among the differences between the classical genre and the other genres is the sole use of the piano. However, the classical genre had a control that was also solely a piano piece: Liszt's Piano Sonata in B-minor, which was also found not to be effective at reducing IEDs. There remain other possible reasons that could explain why Mozart was effective and the other pieces of music were not. One is that the Mozart sonata K448 has quite a fast tempo, 137 bpm in the recording that we used, and it consists of runs of sixteenth notes often performed in parallel on the two pianos which yields an elevated note density for most of its duration compared to the other works in our selection. Further work is needed to match not only the low-frequency modulation spectrum, but also the tempo, onset density, timbral qualities, and possibly other factors such as key and musical form, to ascertain which among these properties might be the primary cause of the effect.
Our preliminary findings were the first to demonstrate a link between specific low-level acoustic features (40-Hz) and higher-order structural phrase boundaries and reduction in IEDs for persons with epilepsy. Our overall research programme aims to address the lacunae in our understanding of the effects of music on brain networks to encourage progress in, and uptake of, music neurostimulation as a viable, safe, affordable treatment option. Building on our preliminary results, in future work we will seek to determine whether reductions in IEDs can be replicated with music stimuli beyond the two verified Mozart works. We propose to further test the effects of music stimuli that are acoustically matched to K448 and K545 using automated audio feature analysis and to measure their effect on IEDs so that we may finally expand the range of music medicine.
In conclusion, we are reminded of the French physician, otolaryngologist Alfred Tomatis, who wrote a book on his experiences using Mozart's music for the treatment of hearing loss and other conditions. His book was entitled, Pourquoi Mozart? For now, we are left with the same question.
Footnotes
Acknowledgements
Dartmouth students Armond Dorsey and Yijing Feng assisted with aspects of the research; Dr. Elaine Chew read the manuscript; and Prof. Theodore Levin contributed to the introduction.
Disclosure statement
No potential conflict of interest was reported by the author(s).