
Abstract
It has been shown that effective treatment in patients with first-episode psychosis (FEP) improves treatment response and functional outcomes [1]. Antipsychotic medications remain the mainstay of treatment in these patients. Although patients with FEP have a better response to antipsychotics than patients with chronic illness [2], they are also more sensitive to the side-effects of these medications [3]. In recent times, the side-effects of weight gain and abnormalities in glucose and lipid metabolism that have been associated with antipsychotic treatment, especially the second-generation antipsychotics (SGAs) have been an area of concern for psychiatrists. In patients with FEP, this side-effect carries the serious health risks of metabolic syndrome in very young individuals who may potentially need long-term treatment. In addition, the dual stigma of not only having mental illness but also being overweight is likely to result in low self-esteem and further lead to social discrimination and isolation in these young people. Weight gain has also been shown to increase the risk of medication non-compliance [4].
Hence there is an urgent need to examine not only the incidence of metabolic abnormalities during treatment with antipsychotic medication in patients with FEP, but also understand the risk factors associated with these side-effects. Zipursky et al. [5] examined the extent, time course and predictors of weight gain from data collected as part of a multicentre, randomized, double-blind clinical trial comparing olanzapine and haloperidol in FEP patients. Intention-to-treat analysis showed that mean weight gain was 10.2 kg with olanzapine and 4.0 kg with haloperidol. Individuals in both treatment groups gained weight rapidly in the first 12 weeks of treatment. The pace of weight gain tapered gradually thereafter and stabilized after 1 year. A 12 week open-labelled, randomized clinical trial that evaluated metabolic changes in drug-naive, FEP patients treated with haloperidol, olanzapine, or risperidone concluded that drug-naive patients experienced weight gain on both first-generation antipsychotic (FGA) and SGA medications after the first 12 weeks of treatment. Significant increases in total cholesterol and low-density lipoprotein (LDL) cholesterol levels were associated with the aforementioned three treatments [6]. In a randomized, double-blind, and controlled prospective study in 99 patients with FEP treated with either haloperidol, olanzapine or risperidone for 6 weeks, it was concluded that 77% of olanzapine-treated patients, 63% of risperidone-treated patients and 22% of haloperidol-treated patients had clinically significant weight gain (≥7%) [7]. The investigators also found that diagnosis of undifferentiated schizophrenia, treatment with olanzapine and lower body mass index (BMI) at baseline were significant predictors for the weight gain.
Prospective, naturalistic studies offer the advantage of examining the treatment outcomes in real-world practice. In FEP, there are often changes to the initial antipsychotic medication and patients are treated with concomitant antidepressants and benzodiazepines for comorbid conditions. In one study that looked at weight gain in 118 FEP patients in a naturalistic way, the investigators found that these individuals gained an average of 11.9% of their original bodyweight and the maximum increase was in the first 6 months [8]. Strassnig et al. followed up 98 FEP patients and 30 controls over a period of 1 year and found that a greater number of co-medications per patient, and co-prescription of antidepressants significantly and independently increased antipsychotic-associated weight gain [9]. None of these studies, however, investigated metabolic parameters such as lipid profile and glucose metabolism.
The aim of the present study was to investigate the effects of antipsychotics on weight changes, serum lipid, glucose and insulin levels, in patients with FEP who were started on antipsychotic medication. The hypothesis was that there would be a high incidence of weight gain, dyslipidemia and serum glucose dysfunction in patients after initiation of treatment.
Methods
All consecutive patients admitted to the Singapore Early Psychosis Intervention Programme (EPIP) between September 2001 and September 2004 who completed the assessments at baseline and later at 6 months were included in the study. EPIP is a nationwide programme launched in 2001 at the Institute of Mental Health and Woodbridge Hospital, the only State psychiatric hospital in Singapore. Fifty-six patients fulfilled the following criteria: (i) age between 18 and 40 years; (ii) presence of a first-episode psychotic disorder; (iii) no prior or minimal treatment (i.e. <72 h of antipsychotic medications); (iv) psychosis was not secondary to substance abuse or medical problems; (v) not on concurrent medications, such as sodium valproate, oral contraceptives, steroids and so on, that could affect weight and glucose or lipid metabolism; and (vi) able to give informed consent. The study was approved by the Institutional Review Board.
The patients were assessed at baseline (i.e. within 72 h of starting antipsychotics), and 6 months later. Patient diagnoses were assessed using the Structured Clinical Interview for DSM-IV, patient version (SCID-P) [10], and the severity of psychopathology was assessed using the Positive and Negative Scale for Schizophrenia (PANSS) [11]. Sociodemographic data was obtained using a semi-structured questionnaire. In addition, weight (kg) and height (m) were measured and BMI was calculated (BMI = weight (kg)/height2 (m)). Blood samples were taken from all subjects in the morning after a 12 h overnight fast. Blood was withdrawn into vacutainer tubes for measurement of blood glucose and lipid analysis. Total cholesterol, high-density lipoprotein, LDL cholesterol and glucose were determined enzymatically using Synchron Lx System(s) (Beckman Coulter, Inc., Brea, California, USA), UniCel DxC 600/800 System(s) (Beckman Coulter, Inc., Brea, California, USA) and Synchron Systems Lipid Calibrator (Beckman Coulter, Inc., Brea, California, USA).
The choice of a particular antipsychotic for the patient was based on the clinical decision of the treating physician and was noted. The total cumulative CPZ equivalent of antipsychotic exposure for each patient during the 6 month period was calculated.
Finally, an outcome event of clinically significant weight gain was defined as ≥7% increase in weight (kg) from baseline at 6 months. This definition is consistent with the US Food and Drug Administration guidelines [12].
Statistical analysis was performed using SPSS version 16.0 (SPSS, Chicago, IL, USA). Parametric tests for data analysis were used when normality assumptions were satisfied, otherwise the equivalent non-parametric test were used for comparison between baseline versus 6 months and between the two outcome event groups of ≥7% weight gain versus <7% weight gain. As where appropriate, confounders were controlled using analysis of covariance or logistic regression. All p values were two-tailed and statistical significance was set at p < 0.05.
Results
Patient characteristics

DUP, duration of untreated psychosis; PANSS, Positive and Negative Scale for Schizophrenia.
Thirty-five patients (62.5%) received the same antipsychotic medication(s) throughout the duration of the study; the remainder of the patients had their antipsychotics changed during the 6 month period. Forty-one patients (73.2%) received antipsychotic monotherapy throughout the 6 months, while 15 (26.8%) were concurrently treated with two antipsychotics during the 6 months. Overall 34 patients (60.7%) received treatment with FGAs (sulpiride, haloperidol, stelazine and chlorpromazine) and 35 (62.5%) with SGAs (risperidone, olanzapine, quetiapine, amisulpride and clozapine). Seventeen (30.4%) received depot medication (I.M Flupenthixol, I.M Pipothiazine, I.M Fluphenazine, and I.M Zuclopenthixol). The mean cumulative CPZ equivalent of antipsychotic medications that was prescribed during the study period was 41 116.35±30 239.46 mg.
Forty-four patients (78.6%) were treated with concomitant medications at some point during the duration of the study, 22 (39.3%) were prescribed benzodiazepines, 34 (60.7%) anti-cholinergics, seven (12.5%) antidepressants and none received mood stabilizers.
Clinical variables vs time
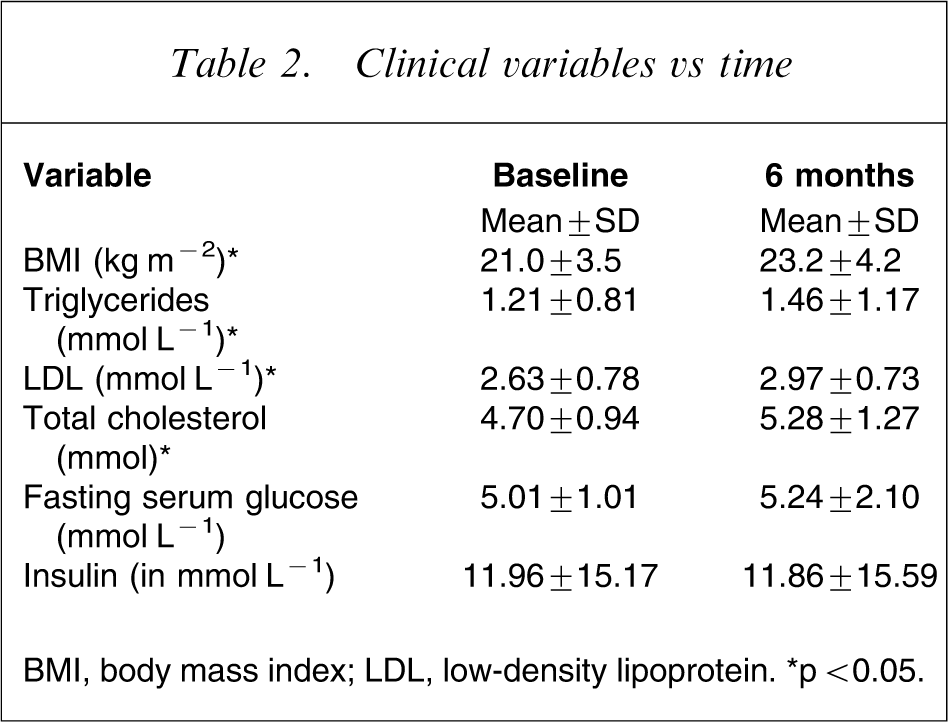
BMI, body mass index; LDL, low-density lipoprotein. ∗p < 0.05.
Factors predicting significant weight gain on logistic regression

BMI, body mass index; CI, confidence interval; CPZ, XXX; LDL, low-density lipoprotein; OR, odds ratio; PANSS, Positive and Negative Scale for Schizophrenia. ∗p < 0.05.
Similarly, analysis of covariance for percentage change of LDL, total cholesterol and triglyceride levels at 6 months was performed controlling for age, gender, BMI at baseline, mean cumulative CPZ equivalent of antipsychotic exposure, and percentage change in BMI at 6 months, and none of the variables was found to be statistically significant.
Discussion
The weight gain and dyslipidemia seen in the present FEP patients after 6 months of treatment with antipsychotics were statistically and clinically significant. This was a naturalistic study and hence it was not possible to determine the extent by which a particular antipsychotic was responsible for the weight gain and make comparisons between different antipsychotics, but the fact that the majority of the patients (79.2%) gained weight and more than half (65%) had a clinically significant weight gain (i.e. ≥7% from baseline), indicates that irrespective of the type of antipsychotic, weight gain is a problem that needs to taken into consideration before starting patients on these medications. Even though the mean BMI and serum lipids at the end of 6 months were within normal limits, there is cause for concern because these increases emerged within a short span of 6 months in a young adult population who, in all likelihood, will need to take the antipsychotic medications on a long-term basis. Hence, the diagnoses and target symptoms need to be carefully defined, patients need to be educated about the metabolic side-effects and advised on healthy lifestyle, and regular monitoring for metabolic problems needs to be initiated.
We found that the patient-related factors (i.e. lower BMI at baseline, female gender, and younger age), rather than treatment and illness-related factors (cumulative CPZ-equivalent dose of antipsychotic exposure and improvement in PANSS scores) were associated with clinically significant weight gain. The significant effect of lower baseline BMI on weight gain has been found in patients with FEP [7] as well as chronic schizophrenia [13]. This finding reiterates that clinicians need to be careful in the choice of antipsychotic for patients who are not only overweight but also for those with normal or even lower baseline BMI. Previous studies have also found a significant association between weight gain and female gender [14, 15], as well as between weight gain and younger age [9, 16].
Results from studies that have investigated effects of dose of antipsychotics on weight gain [13, 17], as well as the correlation with treatment response [18–20] have been mixed and inconclusive. The relationship between therapeutic response, dose of antipsychotic and weight gain is complex and possibly related to other factors such as severity of illness, type of symptoms and adherence to treatment.
There have been previous studies that have reported that the increase in serum levels of lipids correlates with increase in weight [21], whereas others have found that it occurred independent of weight changes [22, 23]. In the present study we did not find a significant association between increase in serum lipids and weight gain. The lack of association between increases in serum lipids and weight gain at 6 months also serves as a reminder to clinicians that metabolic screening needs to be done regularly for all patients and not be restricted to only those who put on weight.
Although there have been many studies that have noted abnormal glucose metabolism in patients with chronic schizophrenia [24–26], studies in patients with FEP have produced mixed results [6, 27]. In the present study we did not find that there were any significant increases in serum levels of fasting glucose as well as insulin. This could possibly be due to the fact that these patients were relatively younger, as compared to patients with chronic schizophrenia, and had a relatively shorter duration of exposure to antipsychotics. Also, very few of the present patients (12.1%) received olanzapine and clozapine, the two antipsychotics that carry a higher risk of abnormal glucose metabolism [28]. A third possibility could be that it was a type 2 error, that is, the relatively small sample size of 56 patients may not have been adequate to detect changes in glucose metabolism.
This was a naturalistic study and hence the decision to start a patient on a particular antipsychotic was based on the clinical decision of the psychiatrist; this may have introduced a bias into the results because individuals with high BMI at baseline may have been more likely to receive a drug seen as having a lower propensity to cause weight gain. The naturalistic design also did not allow us to examine the effects of antipsychotic polypharmacy on weight, because even though 27% of the patients received two antipsychotics at some point during the 6 month period, the length of time that they received the two antipsychotics varied from a few days to a few weeks. The concurrent prescription of two antipsychotics was more likely to be part of a cross-taper rather than an augmentation strategy because none of the patients were on both antipsychotics throughout the duration of the study.
The present study did have some limitations: we did not control for the effects of differences in lifestyle, eating habits, and smoking. Twelve per cent of the patients were given antidepressants and some of the antidepressants are known to cause weight gain. Unfortunately the scope of the present study did not make it possible to separate out the weight gain due to antipsychotics and antidepressants in the patients. Although we did calculate the cumulative CPZ equivalent antipsychotic exposure, we did not measure compliance to the medications. Last, it is difficult to attribute changes in BMI, serum levels of triglycerides, LDL and total cholesterol to treatment alone. The lack of a control group in present study did not allow us to look at the natural changes in weight and metabolic profile in the healthy population. A treatment period of 6 months did not allow us to study the long-term metabolic effects of antipsychotic medication and it would be important for future studies to look at this. Nevertheless, the present findings are clinically relevant and emphasize the need to practise prevention and early intervention not only for treatment of FEP, but also for the metabolic side-effects that occur as a result of this treatment.
Footnotes
Acknowledgements
This project was funded by the National Healthcare Group (NHG), Singapore through their Small Innovative Grant.