
Abstract
Body mass index (BMI) is a widely accepted method for categorizing weight according to height and is typically used in association with health outcomes. Its value has been established, because when BMI scores increase, so do risks for many chronic diseases. Thus, increased BMI has been associated with cardiovascular disease, certain cancers, type 2 diabetes, hypertension, arthritis, and early mortality [1–4].
Associations have also been drawn between BMI, mental health, and suicidal ideation, although there is conjecture regarding the nature of the relationship. Some have reported that increased BMI is associated with depression [5–8] and suicidal ideation [5], whereas others have found that it seems to provide some protection, particularly in male subjects [9–11].
Challenges in interpreting these disparate findings include the fact that they relate to different populations, and that different measures of mental health morbidity have been utilized. A further confounder has been the presence of physical illnesses, which, in their own right, may have influenced the presence of mental disorders. Indeed, a few studies have allowed for that, and it is of note that Jorm et al. reported that controlling for physical health accounted for the association of obesity with depression in women [12]. In contrast, others have reported that when controlling for physical health, an association has remained [7, 8, 13].
The present study was designed to elucidate the relationship between BMI and mental health further by comparing standardized mental health and BMI data, controlling for the presence of physical illnesses, from two large and independently derived data sets of the same community population. The interview techniques differed, as did the measures of depression and suicidality, thereby providing two perspectives on this important clinical and community debate.
Method
Participants
Participants were drawn from two separate South Australian databases: the South Australian Health Omnibus Survey (SAHOS) and the South Australian Monitoring and Surveillance System (SAMSS).
SAHOS participants were assessed in 2008 in the South Australian Health Omnibus Survey (SAHOS), a multi-stage, systematic, clustered area sample of households, conducted annually since 1991 [14]. They were randomly selected from Australian Bureau of Statistics collection districts within the Adelaide metropolitan area and South Australian country towns with a population of ≥1000 people. Data were collected through face-to-face interviews conducted in the home.
SAMSS participants were recruited to take part in a survey conducted each month between 2002 and 2007 to assess trends in the prevalence of chronic conditions, risk and protective factors, and other determinants of health [15]. All households in both rural and metropolitan South Australia with a listed telephone number were eligible for selection, and data were collected via a computer-assisted telephone interviewing (CATI) system.
All interviews were carried out by trained interviewers and each dataset was weighted to provide population estimates across 5 year age groups, sex, area (metropolitan and rural), and household size to match the most recent Australian Bureau of Statistics Census or Estimated Residential Population data for South Australia.
Measures
Body mass index
BMI was calculated using the standard equation of weight (in kilograms) divided by height (in metres) squared and categorization of different BMI was made in accordance with the World Health Organization [16] definition of underweight for scores <18.5, healthy weight for scores between 18.5 and 24.99, overweight for scores between 25 and 29.99, obese for scores between 30 and 39.99, and morbidly obese for scores of ≥40.
Major depression/psychological distress
SAHOS
Major depression was determined using seven items from the Primary Care Evaluation of Mental Disorders (PRIME-MD), an instrument with demonstrated validity and reliability for differentiating DSM-IV diagnoses in primary care settings [17].
SAMSS
Psychological distress was determined using the Kessler 10 [18]. Participants with low (0–15) or moderate scores (16–21) were deemed not to be suffering psychological distress, while those with high (22–29) or very high scores (>29) were categorized as having psychological distress.
Suicidal ideation
SAHOS
Suicidal ideation was determined using responses to the PRIME-MD item ‘In the last 2 weeks have you had thoughts that you would be better off dead or of hurting yourself in some way?’
SAMSS
Suicidal ideation was determined using four items drawn from the severe depression subscale of the 28-item General Health Questionnaire (GHQ-28). These were: ‘Have you recently felt that life is not worth living?’; ‘Have you recently found yourself wishing you were dead and away from it all?’; ‘Have you recently had thoughts of the possibility that you might do away with yourself?’; and ‘Have you recently found that the idea of taking your own life kept coming into your mind?’. This has been described in detail elsewhere [19, 20].
Physical illness
SAHOS
Overall levels of physical functioning was assessed with the Physical Component Summary (PCS) of the SF-12 [21] using Australian norms.
SAMSS
Participants were asked to indicate whether a doctor had ever told them that they had diabetes, asthma, other respiratory problems (such as bronchitis, emphysema, or chronic lung disease), coronary artery disease (heart attack or angina), arthritis, or osteoporosis.
Analyses
Controlling for demographic variables and measures of physical health, associations between each of the BMI categories (dummy coded with ‘healthy weight’ as the reference category), major depression/psychological distress, and suicidal ideation were examined on weighted data using hierarchical logistic regression, in SPSS for Windows version 15.0 (SPSS, Chicago, IL, USA).
Results
In the SAHOS there were 3034 participants aged ≥15 years, representing a response rate of 62.8%. The mean age was 45.8 years (SD = 18.9), and 1479 (48.7%) were male. In the SAMSS there were 30214 participants aged ≥16 years, with a response rate of 69.3%. Their mean age was 46.0 years (SD = 18.7), and 14811 (49.0%) were male.
Descriptive statistics
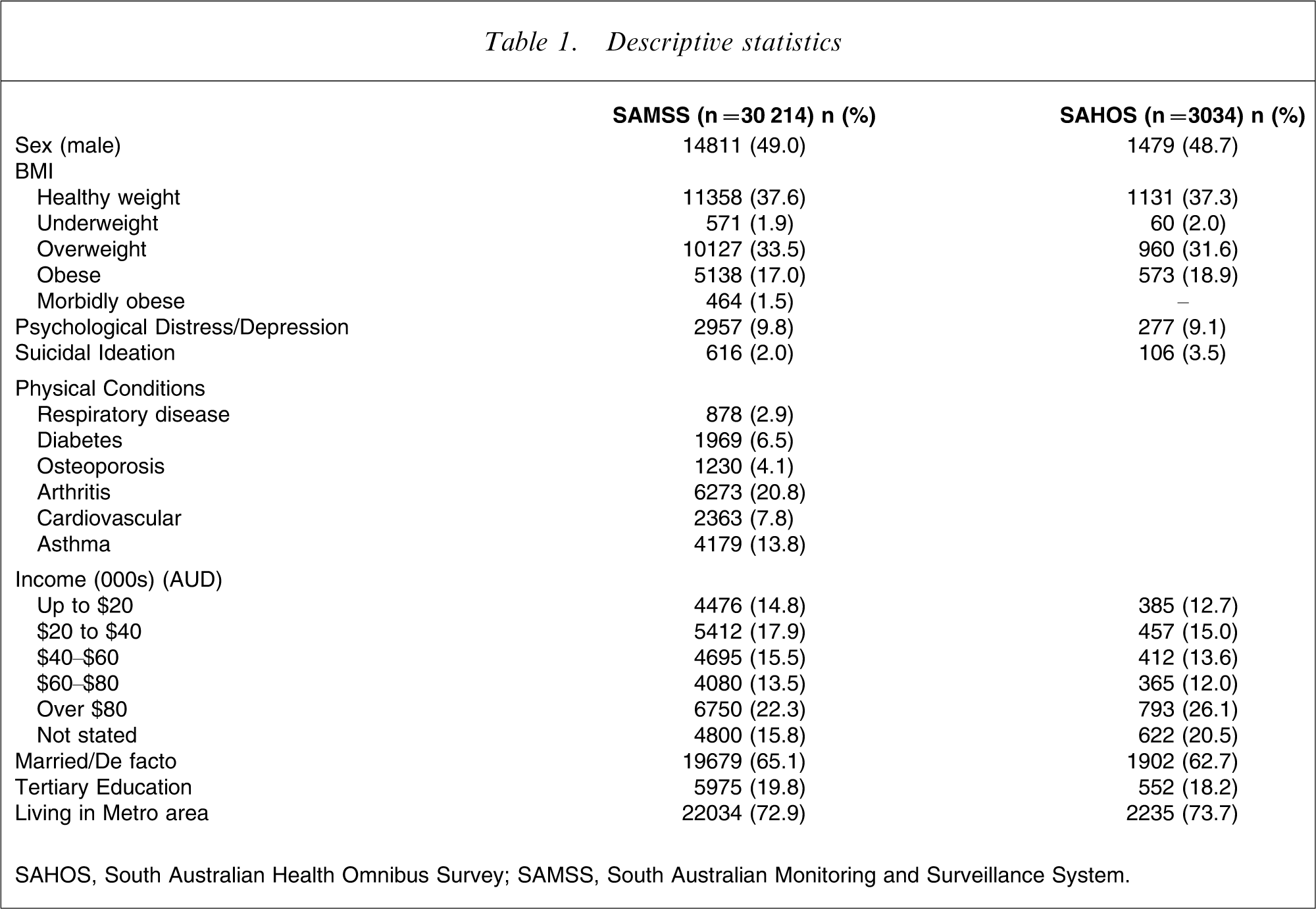
SAHOS, South Australian Health Omnibus Survey; SAMSS, South Australian Monitoring and Surveillance System.
Mental Illness vs BMI
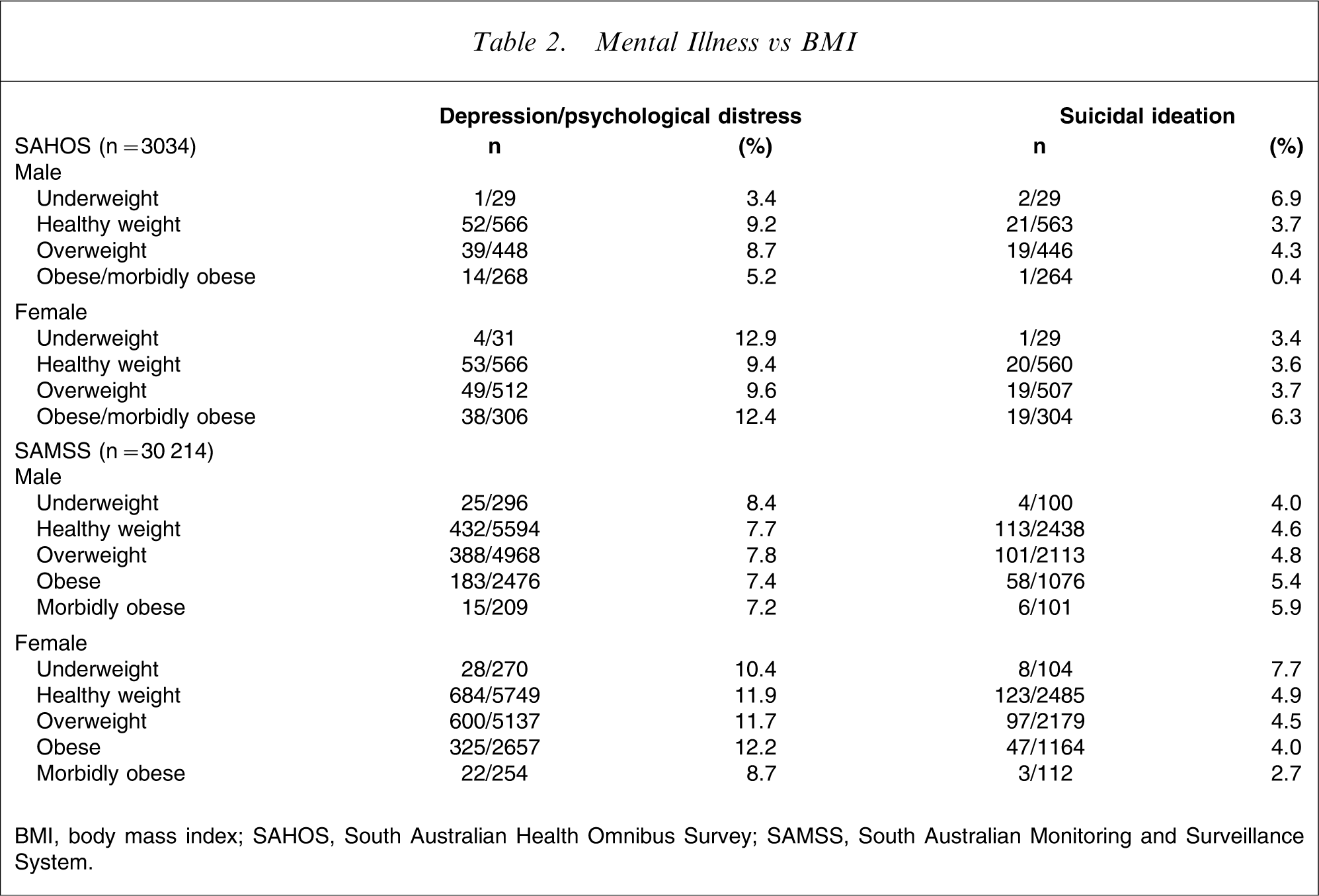
BMI, body mass index; SAHOS, South Australian Health Omnibus Survey; SAMSS, South Australian Monitoring and Surveillance System.
SAHOS: multivariate associations between BMI and mental health†
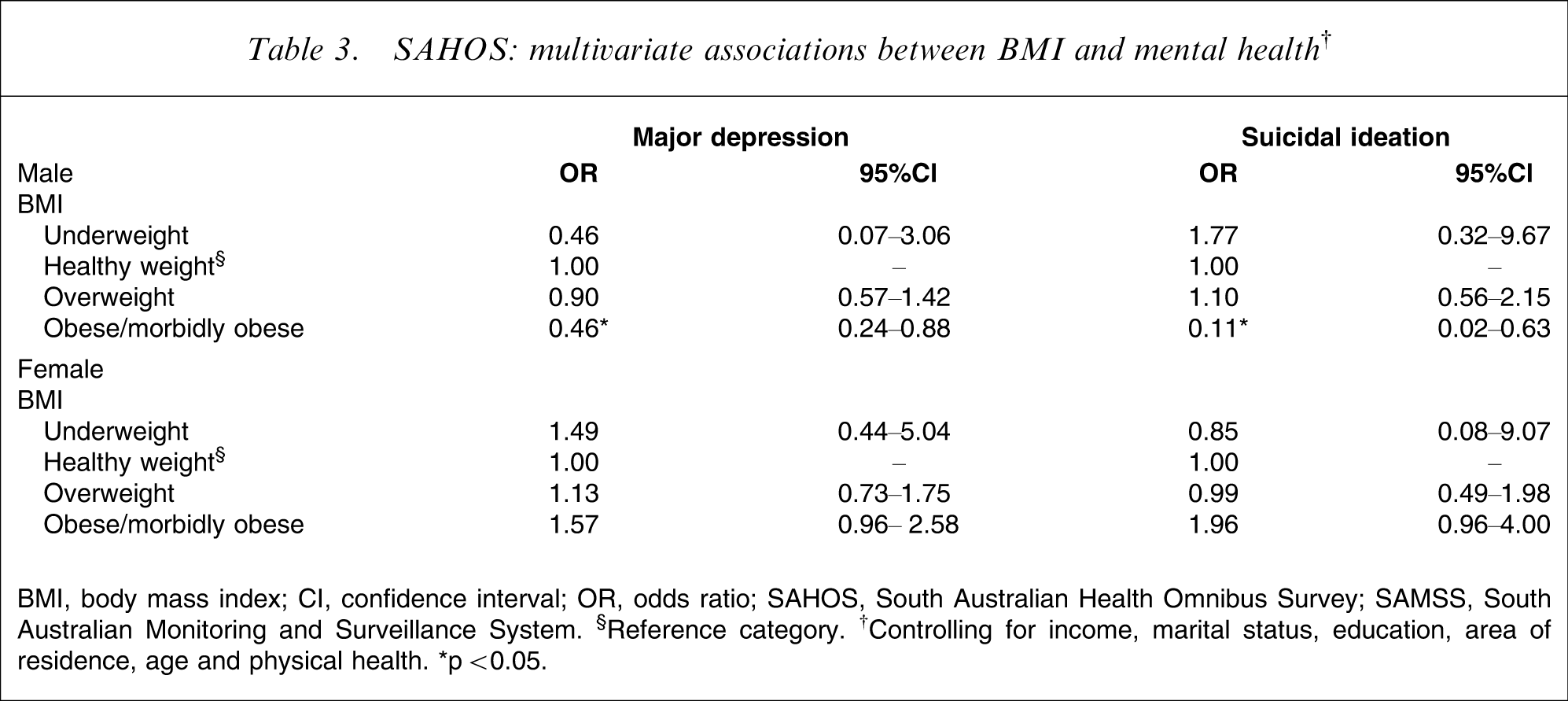
BMI, body mass index; CI, confidence interval; OR, odds ratio; SAHOS, South Australian Health Omnibus Survey; SAMSS, South Australian Monitoring and Surveillance System. §Reference category. †Controlling for income, marital status, education, area of residence, age and physical health. ∗p < 0.05.
SAMSS: multivariate associations between BMI and mental health†
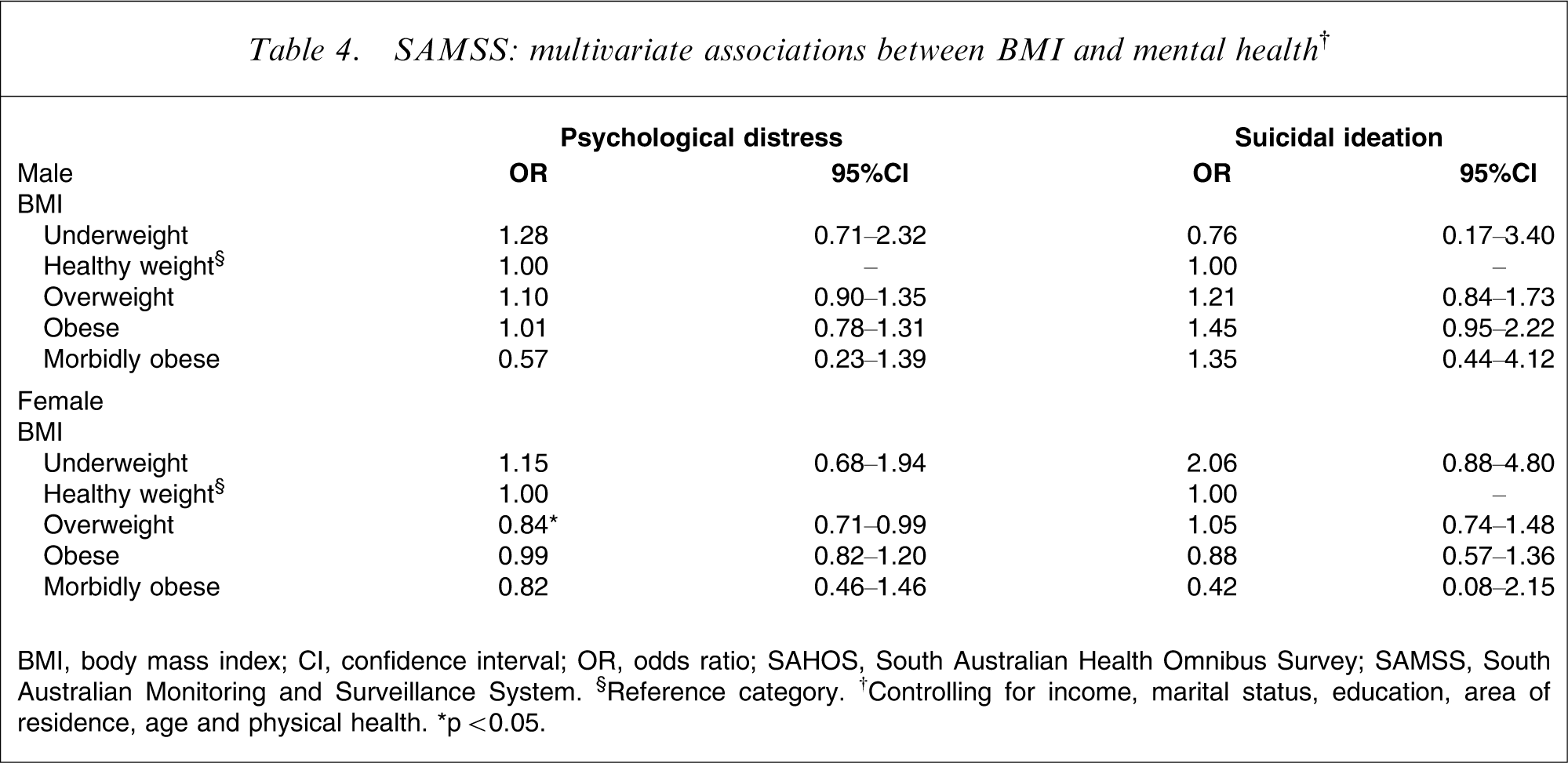
BMI, body mass index; CI, confidence interval; OR, odds ratio; SAHOS, South Australian Health Omnibus Survey; SAMSS, South Australian Monitoring and Surveillance System. §Reference category. †Controlling for income, marital status, education, area of residence, age and physical health. ∗p < 0.05.
For the SAHOS data (Table 3), obese men were significantly less likely to have major depression or suicidal ideation than those within healthy weight, but there was no such associations for women.
For the larger SAMSS data (Table 4), the only significant result was for overweight women to report less psychological distress than their healthy weight counterparts.
Similar results were obtained using BMI as a continuous variable, when demographic data and physical health were controlled for. In the SAMSS data, continuous BMI was not significantly associated with psychological distress or suicidal ideation in either gender. In the SAHOS, continuous BMI was not associated with major depression for either gender, but there was a significant inverse association for men but not for women, with suicidal ideation (odds ratio (OR) = 0.926, 95% confidence interval (CI) = 0.86–0.99, p = 0.03). BMI was also included as a quadratic term, but this was not significant in any analyses, indicating no evidence of a u-shaped relationship between BMI and depression/suicidal ideation.
Discussion
At the outset it is important to note that these findings are consistent with the variable results obtained from other research. Although the random and representative samples within this study were drawn from the same general population, the differences in the results are not unexpected because different methods were used. This variation between methods is both a weakness and strength. The replication of results is the cornerstone of the scientific method, but replication is even more robust if it can be done with different methods, and, in this regard, the consistent findings across these two databases appear to outweigh the differences, and the differences in themselves are consistent with the questioning of hitherto accepted assumptions.
Before discussing these results further, it is pertinent to reflect on potential shortcomings of this research. It could be argued that different results might emerge if BMI was used as a continuous variable. This was addressed, and no statistically significant association emerged between BMI and psychological distress and suicidal ideation in the SAMSS data, and the SAHOS data showed no association with major depression, although there was a statistically significant, albeit small, decrease in suicidal ideation in men with increasing BMI, consistent with the initial analyses. Furthermore, the lack of significance when BMI was used in a quadratic form precluded the presence of any u-shaped relationship.
It may be pertinent that the data were not all gathered during exactly the same time period, and it is possible, although unlikely given the limited variability of time, that this would have influenced results. Perhaps the biggest shortcoming is that the BMI was calculated on the basis of respondent information, rather than direct measures, and, although some researchers have found that self-reported height and weight have provided an accurate representation of BMI [22], it is generally believed that there is a tendency for self-report to overestimate height and underestimate weight [23]. Nevertheless, the majority of studies have used self-report measures, and therefore comparison with them appears to be valid. It is also acknowledged that information about physical health was not verified with clinical records or doctor reports.
It is also fair to note that the use of the SF-12 PCS scoring could be questioned, and the alternative RAND-12 scoring method has been advocated [24]. Most studies, however, have used the factor scoring method, and this has been used to facilitate comparison with previous work.
Notwithstanding these caveats, we consider that these two random and representative community samples of the same broad population, rather than clinical samples, represent a unique opportunity to examine the association of BMI with measures of mental health and suicidal ideation using differing methods. Indeed, to the best of our knowledge there have not been previous reports of such analyses of the one population.
The most striking feature of these results is that being overweight was not significantly associated with increased depression or psychological distress or suicidal ideation in either of the two datasets. In fact, obese men in the SAHOS analysis were significantly less likely to have major depression or report suicidal ideation, and overweight women in the larger SAMSS dataset were less likely to experience psychological distress. Indeed, there was no statistically significant finding in either the SAHOS or SAMSS dataset to associate obesity or morbid obesity with major depression, psychological distress, or suicidal ideation. This lack of significant association was consistent across both sets of analyses, despite methodological differences. This is of particular note in terms of the physical illness confounders, for which SAHOS analysis was restricted to the Physical Component Summary of the SF-12, whereas the SAMSS analysis had the benefit of controlling for specifically acknowledged illnesses. It is of interest that when physical confounders were not controlled for, the previously noted protective factors remained significant in both the SAHOS and SAMSS, but in the SAHOS the obese and morbidly obese women had a statistically significant increase in suicidal ideation (OR = 1.98, 95%CI = 1.02–3.85, p = 0.04).
The present results are consistent with the only other similar Australian data controlling for physical ill-health, those of Jorm et al. [12], and did not replicate the reports of Dong et al. or Onyike et al. from the USA, who found that extreme obesity (BMI ≥40), controlling for physical illness, was associated with depression [7, 13]. They are also not consistent with the recent US work of Zhao et al., but it may be pertinent that they controlled only for selected obesity related comorbidities [8]. Furthermore, the absence of an association between suicidal ideation and BMI, including morbid (extreme) obesity, was not consistent with Dong et al. [25], who reported an association between extreme obesity and attempted suicide. Indeed, the protective effect in men was consistent with the observation of Mukamal et al. that suicide risk in men is ‘strongly inversely related to BMI’ [9].
Bearing in mind the weak, albeit statistically significant findings from this and other studies and the variability of results, it would be premature to speculate why there could be any protective effect from increasing BMI. At the very least we would agree with Mukamal et al. [9] that ‘obesity can not be recommended’ on the basis of such findings. Furthermore, it is pertinent to reflect that BMI may be too blunt an instrument to examine these relationships. In this regard it is of note that a recent report suggested that depressive symptoms may be associated with abdominal obesity, rather than overall obesity [26], although previous research assessing waist circumference in relation to depressive disorders provided negative results [27]. It may also be relevant that weight perception may be a more important risk factor for psychological distress than actual weight status (BMI) per se [28]. Indeed, future studies could well include measures of abdominal obesity and weight perception.
Conclusion
The present results, coupled with those of other studies, confirm that the relationship between BMI, mental health, and suicidal ideation is complex. There are now data that indicate that being overweight may actually be protective for some people, and, at the very least, it is no longer tenable to state without qualification that increasing BMI is necessarily associated with adverse mental health.