
Abstract
Sleepwalking is a parasomnia characterized by automatism related to arousal during non-rapid eye movement (NREM) sleep. It may present variably from aimless walking or wandering behaviours to a series of more elaborate and complex activities such as driving or sleep-related violent behaviours. The episodes commonly occur in the first one-third of the night and the subjects usually have complete or partial amnesia afterwards. The evolvement of the understanding of the pathophysiology and aetiologies of sleepwalking ran parallel with the advance of sleep medicine and psychiatry. The apparent dramatic scenes of sleepwalking were earlier hypothesized as a type of dissociative disorder during which the subjects might act out their unconscious traumatic experiences during sleep [1]. This dissociative hypothesis of sleepwalking, however, was not supported by modern clinical evidence [2]. Nowadays sleepwalking is regarded as an independent disorder with complex aetiologies, consisting of interactions among genetic predisposition [3, 4], facilitating factors such as sleep deprivation, and triggering factors that increase sleep fragmentation [5].
Sleepwalking has a typical onset in childhood. It usually disappears when the child grows up and hence it is mostly regarded as a self-limiting illness related to central nervous system immaturity [6]. In adults, sleepwalking is less common, having a population prevalence rate of 2.0–3.5% [4, 7]. As based on the Finnish population-based twin study, the majority (>80%) of adult sleepwalkers had childhood-onset sleepwalking; and adult-onset sleepwalking was relatively rare [4].
There was a suggestion that adult sleepwalking was more likely to be associated with psychopathology and psychotropic medication. Epidemiological study in the general population found that a higher percentage of subjects with adult sleepwalking suffered from psychiatric illnesses, especially affective spectrum disorder [7]. Active adult sleepwalkers were suggested to be more likely to have personality disorder [8]. Nonetheless, there were arguments against the association of psychopathology and adult sleepwalking. A study on adult patients with sleep-related injury reported that the majority of subjects with sleepwalking did not have a lifetime psychiatric diagnosis. In addition, the treatment of underlying psychiatric illnesses did not lead to remission of the parasomnia [9]. Hence, other factors might also contribute to adult sleepwalking. In particular, there were accumulating case reports on psychotropic-related sleepwalking, but there was a lack of large case series or systematic study in psychiatric populations [10–22].
Given these potential risk factors, adult psychiatric patients, who suffer from active psychiatric illnesses and who are taking psychotropics, were hypothesized to be more susceptible to develop sleepwalking. Thus, we carried out a clinical epidemiological study in psychiatric outpatients. The estimated lifetime and 1 year prevalence of sleepwalking were found to be 8.5% and 2.9%, respectively, which were higher than that of general population [23]. Similar to the other studies on adult sleepwalking, this clinical epidemiological study was limited to only active adult sleepwalkers, and there was no delineation of the age of onset and the clinical characteristics. Because there is limited knowledge on the clinical similarities and disparities between adult-onset and childhood-onset sleepwalkers in the psychiatric population, the aim of the present study was to investigate these sleepwalkers with reference to age of onset and clinical profiles.
Method
A cross-sectional study was conducted in a regional university-affiliated psychiatric outpatient clinic, the details of which have been described elsewhere [23]. In brief, adult subjects aged 18–65 years attending the clinic within a consecutive 4 week period were recruited into the study. A self-report questionnaire including demographics and sleep problems was followed by a second-phase clinical interview for confirmation of the sleep diagnosis. The questionnaire has been demonstrated to have good validity and reliability [23]. The age of onset, duration of illnesses and frequency of attacks of sleepwalking were also investigated. Computerized clinical data and case notes were reviewed for psychiatric, medical and psychotropic prescription histories. The principal psychiatric disorders were diagnosed clinically according to ICD-10 [24]. The medication records included the list of psychotropics that the subjects had been given since the beginning of psychiatric service (lifetime psychotropic history) and the latest prescriptions for the last 1 year (current psychotropics).
This study was approved by the institutional ethics committee and written consent was obtained from the subjects. Univariate analysis of continuous and non-parametric data was performed using Student's t-test and χ2 test, respectively. Fisher's exact test was used for n < 5 in the non-parametric data. Predictive variables were determined by logistic regression. Backward stepwise model of logistic regression was used and the result was checked with the forward model. The cut-off for the selected variable for logistic regression was fixed at p < 0.10. SPSS version 14.0 (SPSS, Chicago, IL, USA) was used for data analysis.
Results
Sixty-six subjects had a confirmed lifetime diagnosis of sleepwalking. Approximately 56% (n = 37) had onset of sleepwalking in childhood or when they were teenagers (group A, age of onset <18 years), while the remaining 29 subjects (43.9%) had adult-onset sleepwalking (group B, age of onset >18 years). Among the childhood-onset sleepwalkers, 60% (22 out of 37) had no further episodes in their adulthood and 15 subjects (40%, 15/37) had sleepwalking in both childhood and adulthood. There were no significant differences in gender, age and family history of sleepwalking between the childhood- and adult-onset groups (Table 1). The adult-onset sleepwalkers (group B), however, had a higher body mass index (BMI) and a higher percentage of sleep-related eating (SRE) behaviours during sleepwalking (group A, 5.4%; group B, 65.5%, p < 0.001), which were characterized by eating and sometimes cooking behaviours during the automatism attacks. Consumption of high-calorie food such as instant noodles and chocolates was commonly reported by the subjects. The adult-onset sleepwalkers also had more frequent attacks of sleepwalking (peak attacks, monthly: group A, 13.5%; group B, 37.9%, p = 0.0022). The prevalence of sleep-related injuries as a consequence of sleepwalking was, however, comparable between the groups (group A, 32.5%; group B, 34.5%).
Subject characteristics vs age of sleepwalking onset
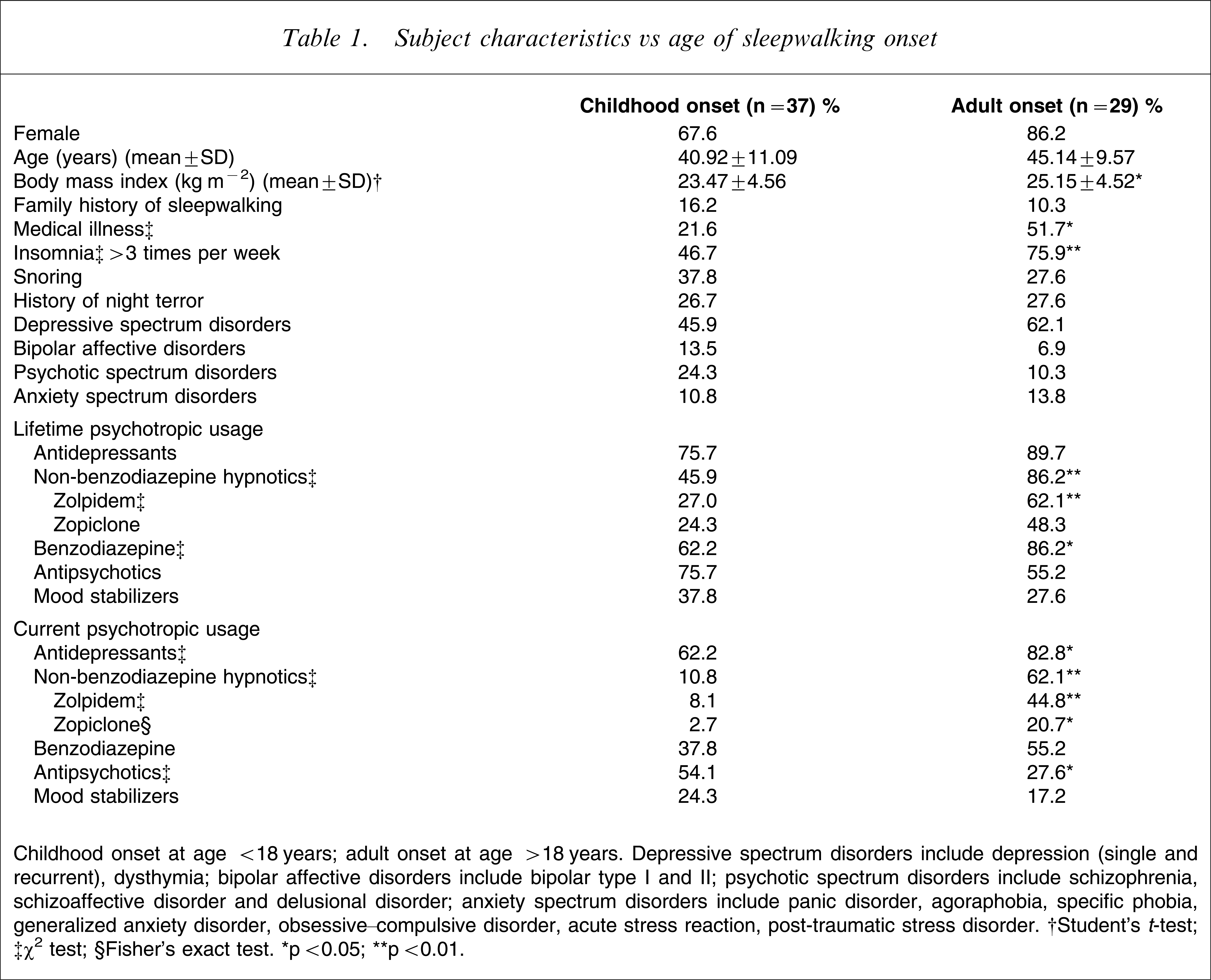
Childhood onset at age <18 years; adult onset at age >18 years. Depressive spectrum disorders include depression (single and recurrent), dysthymia; bipolar affective disorders include bipolar type I and II; psychotic spectrum disorders include schizophrenia, schizoaffective disorder and delusional disorder; anxiety spectrum disorders include panic disorder, agoraphobia, specific phobia, generalized anxiety disorder, obsessive–compulsive disorder, acute stress reaction, post-traumatic stress disorder. †Student's t-test; ‡χ2 test; §Fisher's exact test. ∗p < 0.05; ∗∗p < 0.01.
In comparison with the childhood-onset sleepwalkers, the adult-onset sleepwalkers had increased prevalence of medical illnesses including hypertension, diabetes mellitus and ischaemic heart diseases (Table 1). They also had more insomnia symptoms. They had a higher prevalence of usage of non-benzodiazepine hypnotics, especially zolpidem, in both lifetime and active usage. For those taking the non-benzodiazepine hypnotics, all of them were taking the therapeutic dosage and the majority (14/18, 77.8%) were using them regularly and nightly.
Logistic regression suggested that frequent insomnia (odds ratio (OR) = 5.39, 95% confidence interval (CI) = 1.58–18.40, p = 0.007) and lifetime usage of zolpidem (OR = 5.58, 95%CI = 1.65–18.84, p < 0.006) were associated with a higher risk of adult-onset sleepwalking after adjustment for age, gender and peak frequency of sleepwalking.
Discussion
In contrast to the uncommon occurrence of adult-onset sleepwalking in the general population (fewer than one-sixth of all sleepwalkers) [4], a much higher proportion of adult-onset sleepwalkers was found in the pyschiatric population (44%). The increased prevalence of adult-onset sleepwalking in the psychiatric population was probably not incidental but aetiologically related, as suggested by their unique clinical features and the associated risk factors.
Adult sleepwalking was suggested to differ from childhood sleepwalking in terms of increased frequency of attacks and lower association of family history [8, 25]. The present findings extend the previous results in psychiatric populations. Although the prevalence of sleep-related injuries and family history was comparable between the two groups, the adult-onset sleepwalkers had more frequent attacks, and had more diverse and complex clinical features, especially the high comorbidity of SRE features, which was rarely seen in childhood sleepwalking.
The exact nosological status and aetiological factors of SRE syndrome are not certain, but SRE is commonly regarded as a variant of sleepwalking [26, 27]. It is characterized by involuntary eating, drinking or cooking behaviour under impaired level of consciousness. Two case series of five and 19 subjects, respectively, and a clinical epidemiological study in a psychiatric sample consistently demonstrated the association of zolpidem usage and SRE [23, 28, 29]. This compelling evidence of zolpidem and SRE has been replicated in the present study. The adult-onset sleepwalkers had a significantly higher lifetime chance of taking zolpidem, mostly at regular and therapeutic dosage. Zolpidem, a non-benzodiazepine hypnotic, could contribute to sleepwalking by its amnesic effect and possible modulation of slow wave sleep [30]. In contrast to other non-benzodiazepine hypnotics such as zopiclone, zolpidem seemed to be specifically associated with eating behaviour during the automatism attacks. The exact mechanism remained enigmatic but the possible effect of zolpidem-related hyperphagia was postulated [23]. In this regard, further pharmacological investigation into the relationship between eating behaviour and zolpidem, especially on the subtypes of γ-aminobutyric acid receptors, is needed. In addition, the present case series failed to demonstrate the previously reported association of adult-onset sleep walking with other psychotropics such as antipsychotics and mood stabilizers [10, 18, 20].
We also found that the adult-onset sleepwalkers had higher BMI and concurrent medical illnesses, particularly cardiovascular disease, hypertension and diabetes mellitus. Pressman reviewed the case reports of medication-related sleepwalking and observed that most of the patients had complex medical and/ or psychiatric histories [5]. The underlying pathophysiology, however, remained elusive, especially on whether these associated factors were aetiologically related or merely a consequence of increased bodyweight and subsequent metabolic and cardiovascular medical illness in the adult sleepwalkers (e.g. via SRE features).
Regarding the role of psychopathology in adult-onset sleepwalking, mental illnesses per se did not stand out in the present results. In contrast to the previous reported association of SRE and eating disorder populations [31, 32], the present study did not find any association between them. The lack of association was probably related to the low prevalence of eating disorders among the present psychiatric sample group [23]. Furthermore, the present study subjects were all recruited from a psychiatric clinic, hence the effect of psychopathology or mental stress between different groups of sleepwalkers (flooring effect) was less prominent when compared to that of the general population. In contrast, the association of adult-onset sleepwalking with insomnia suggests an intriguing relationship. As shown by previous studies, insomnia has a complex relationship with psychiatric morbidity and could be seen as a symptom, prodrome, risk factor of future psychiatric morbidity or an independent disorder [33]. Thus, the present study adds another important association: that frequent insomnia in the psychiatric population is closely associated with sleepwalking. The detailed pathophysiological mechanisms are unclear. It remains to be determined, in further prospective studies, whether those subjects having frequent insomnia, hence more sleep disruptions, might be directly predisposed to the development of sleepwalking [5], or whether the sleepwalking occurs as a result of the hypnotics being given to treat the insomnia [23, 28, 29], or whether the sleep disruptions and insomnia occur as a consequence of sleepwalking features, especially with complex SRE-dominant features in adult sleepwalkers [34].
Some limitations were noted in the present study. Inherent to most studies of parasomnia, the diagnosis of sleepwalking was subject to recall bias, although we attempted to collect collateral history from the family members or bed-partners. Psychiatric morbidity was measured clinically without any structured interview and the impact of real-time association with active psychopathology was not addressed. Although most subjects reported good drug compliance, the current study did not measure other objective indices of compliance. Also, we were looking into lifetime history of sleepwalking and hence the real-time association of psychotropics, medical illnesses and insomniac symptoms with active sleepwalking could not be determined. Polysomnographic sleep assessment was not a mandatory requirement for the diagnosis of sleepwalking (ICSD-II) [34], but the lack of polysomnographic information might limit the diagnosis of comorbid and hidden sleep disorders such as sleep-related breathing disorder [35].
In summary, the present study suggests that adult-onset sleepwalking in the psychiatric population has unique clinical characteristics and aetiological basis, and is distinct from that of childhood-onset sleepwalking. Adult-onset sleepwalking was characterized by atypical SRE features, use of non-benzodiazepine hypnotics especially zolpidem, and presence of frequent insomnia. These results suggest that the assessment of adult sleepwalkers should include thorough sleep, psychiatric, medical and medication assessment. Clinically, the presentation of adult-onset sleepwalking in the psychiatric population warrants investigation of atypical clinical features, review of psychotropic prescriptions and management of comorbid sleep disturbances.
Footnotes
Acknowledgements
Dr YK Wing is currently receiving research support from Sanofi Aventis. (A study “Efficacy and safety of 2mg/day of M100907 on sleep maintenance insomnia with a sub-study of the effect of M100907 on stable Type II diabetes mellitus: a one year, multi-center, randomized, double-blind, placebo-controlled study”).