
Abstract
The development of a code of ethics is one of the hallmarks of a profession, but defining what the ethics of any group should be is fraught with difficulty. Opinions vary, there is disagreement as to the extent to which values are personal or communal, and all attempts to codify ethics struggle to cope with different contexts. Health professionals and bioethicists have responded to these difficulties by seeking moral and political validity for codes of ethics in empirical data.
Much has been made of the so-called ‘empirical turn’ in bioethics discourse [1]. It has been argued that sociological methods have an important contribution to make to bioethics discourse [2]. Sugarman describes these methods as ‘the application of research methods in the social sciences (such as anthropology, epidemiology, psychology, and sociology) to the direct examination of issues in bioethics’ [3]. Empirical methods aim at a descriptive, rather than normative account of ethics – they define ‘what is’ rather than what ought to be. Empirical research can shed light on many aspects of ethics. It can inform the different phases of ethical reasoning-the description of the moral question, the assessment of the moral question and the evaluation of decision-making around the question [4]. Empirical research can also describe how ‘social actors’ interact within a moral framework and better define the nature of a phenomenon, such as a value system or the nature of an ethical dilemma [5]. Empirical approaches to ethics are a relatively new process in psychiatric research [6].
Importantly, empirical research can also inform the study of ‘values’ (axiology). Values conceptually develop before ethics in that values help determine what is regarded as ‘the Good’. To behave ethically is to behave in regards to such a conception of the Good. When looking at the values of groups, such as psychiatric professionals, the sociological perspective of values comes into play. The most important thinker in this area was John Dewey, who saw the definition of the Good as the outcome of a process of ‘valuation’. Such valuation is an iterative process of balancing of personal and cultural sets of values [7].
Various methods of empirical axiological study have emerged from sociology, the best known being the Hartman value profile, which tests through questionnaires what people regard as valuable [8]. We had previously conducted qualitative research to identify the values of a group of psychiatrists in Argentina [9, 10], work that established that qualitative methods could be used to empirically evaluate the values of a group. In the present study we describe the values held by Australian psychiatrists, in order to appraise the existing Royal Australian and New Zealand College of Psychiatrists (RANZCP) Code of Ethics [11]. Using empirical methods, such as those used in the present study, to validate and evaluate codes of ethics in psychiatry is unique because this is usually done by special committees rather than through analysis of data [12].
Methods
To assist the reader we have provided a glossary of terms (Table 1).
Glossary of terms
Ethnomethodology
Ethnomethodology is a form of qualitative enquiry, which examines how social order is achieved by the interaction of social actors. Garfinkel's original work in ethnomethodology described the documentary method, in which social actors selectively abstract certain facts from a given social situation, observe patterns among the facts and then attempt to comprehend these patterns [13, 14]. The social actors comprehend an observed phenomenon by contextualizing or ‘indexing’ it to particular circumstances. Other ethnographic methods have been described since the seminal work of Garfinkel, in particular the ‘talk-in-interaction’ and ‘study of work’ method described by Psathas [15]. In the present study the aim of the ethnomethodological approach was to construct a local theory of values relating to this group of Australian psychiatrists. Because ethnomethodology does not have a rigid methodological approach to acquiring and analysing data, various techniques from established qualitative methodologies can be applied to the process.
Sample and recruitment
The study sample was obtained using a theoretical approach [16, 17] to purposive (i.e. non-probabilistic) sampling [18]. Rather than making a priori judgments about the characteristics of the sample, each subject was deliberately selected after examining results of the ongoing analysis of the data. In other words, the type of participant was determined iteratively by the responses of previous participants. The Human Research Ethics Committee (HREC) at the University of Sydney approved the study.
Interview
Semi-structured interviews were conducted with each participant and digital dictaphone recorded these. The recordings were then transcribed and coded. Based upon an iterative process, emergent codes or areas of interest influenced subsequent interviews, either as new questions or through the choice of interview subjects. Defining the point of ‘thematic saturation’ was difficult, given the lack of consensus or evidence-based guidance in the qualitative research literature [19]. The work of Guest et al. suggests theoretical saturation occurs ‘when all of the main variations of the phenomenon under study have been identified and incorporated into the emerging theory’ [20]. In other words, ‘saturation’ is operationalized as the point in data collection and analysis when new data produce little or no change to the codebook. In defining theoretical saturation, another researcher coded sections of transcripts independently, and coding strategies were compared. No new coding categories emerged after the 11th interview, but the sample was extended to address apparent biases in the data set, based on the demographic factors of age, gender and work setting.
Reflexivity
‘Reflexivity’ in qualitative research refers to an awareness of the researcher's contribution to how the data are collected and analysed. In order to achieve an appropriate degree of reflexivity, the researchers regularly discussed coding frameworks, which is argued as a valid strategy in reflexivity [21], particularly when points of variance in coding of extracts serves as the focus of discussion [22].
Analysis
The data analysis was based on the method described by Richards [23], using the NVIVO7 software package (QSR International, Melbourne, Victoria, Australia). The interviews were transcribed and then read closely with a view to identifying various categories of speech acts. These were coded into the nodes function on NVIVO7 and memos written. The journal function of NVIVO7 provided linkages between the various memos and conceptualizations of the data as they were developing.
The analysis of the interview data by the first author, a psychiatrist, was considered to have been influenced in a top-down way. The second phase of analysis involved the re-reading of nodes and memos, and the condensation of nodes into the tree nodes function of NVIVO7. This generated the initial thematic map. The coded extracts (and linked memos) were then examined for overlap in the different nodes. Extracts that displayed significant overlap were then reformulated with reference to the various nodes in which they were initially coded. In this way themes were developed and various subthemes were integrated into the larger themes. The nodes that were negligibly represented in the coded extracts were either subsumed into larger themes or rejected. After the initial process of coding, subsequent analysis of the data was based upon a thematic analysis approach, as described by Braun and Clarke [24]. Some aspects of the analysis drew upon the grounded theory method developed by Strauss and Corbin [25] and Charmaz [17].
Results
The sample characteristics are shown in Table 2. The open coding of the data is shown in Table 3. The main themes to emerge from the data are shown in Figure 1. In refining the coding of the data set into a set of values constructed by psychiatrists, four core themes emerged: ‘valuing patients’, ‘advocacy’, ‘reflection’ and ‘sophisticated understanding’.
Core values of the Australian psychiatric profession based upon the data set.
Sample characteristics
Data coding pattern
Valuing patients
In the data analysis a number of subthemes emerged, which appear to provide a richer description of what psychiatrists valued in their patients. The first was the notion of valuing of the patient's identity and their individual experience manifest as the patient's unique narrative:
I think that a narrative is, I think that an interview, a narrative, an understanding of the person, an individual perspective is fundamental to my interactions with a patient, to everything, to my ability to make a diagnosis, to my ability to formulate a management plan, have to be on that individual basis. I don't know that the person's interested in those things, I think they're interested in their narrative, I don't think they care how I get to what I think I need to. (Psychiatrist 14)
All of the participants viewed the diagnostic act as an integral part of their work in that it:
labels the patient and it can set a course of action in terms of treatment or in terms of the person's or other people's opinions of that patient or whatever … I use the fact that it is a label, I use it as a focus for describing what's going on. (Psychiatrist 1) (O)nce people are adults and talking about their experiences of child abuse, I think that we tend to deal with our discomfort by stigmatizing the victim, and no matter what we label them, whether it's the good old fashioned hysteric, or it's your contemporary borderline, what we are doing is dealing with them from a very defensive position that culture is unhappy with confronting. (Psychiatrist 3)
The other subtheme was the value of defining the patient's experience in terms of their resilience rather than deficit or impairment. One of the psychiatrists interviewed gave an emotional account of this value:
I see people who have unbelievable pain, and unbelievably awful experiences, and they soldier on, and you just look at them and you think, my God, humans are just something special. (Psychiatrist 12)
Advocacy
The core value of advocacy included the beneficent and non-maleficent diagnostic act, appropriate levels of political activism, and advocating for individual patients and patient groups. For one psychiatrist it was simply a case of ‘making sure they (patients) don't get lost or screwed around’. Approximately half of the participants viewed an advocacy role as having a broader social imperative:
I personally felt like I didn't, well I did have an option, but I felt required to act beyond the individual advocacy. (Psychiatrist 7)
There was no consensus as to what the limits of such advocacy ought to be for psychiatrists. One of the participants offered an ‘onion skin’ model of advocacy, which provided a means of defining the level of psychiatric advocacy relating to psychiatry's place in social and political discourse. The onion sort of skin model of justice, if that exists, I think to be just in our clinical practice to the best of our abilities is a starting point, to treat patients fairly and with respect, to improve their access to treatment, to provide them with the best treatment, I think has to do with justice. Then with the additional layers, I suspect the further you progress through the layers, the less influence or role the psychiatrist has. (Psychiatrist 11)
Sophisticated understanding
The value of ‘sophisticated understanding’ integrates the value placed upon seeking a comprehensive and elaborate understanding of the patient and their environment as well as the systems in which psychiatrists and their patients find themselves. The sophisticated understanding of the patient is the integration of different components of a particular patient's situation: context, symptoms, psychodynamics, existential aspects, broader sociocultural factors, and how their experience is communicated in different cultural settings. This was referred to as the need for ‘integrative models’ or to be ‘holistic’. For one psychiatrist, ‘the marrying of those is the heart of how you come up with a management plan in what you're doing’. Moreover, the value of sophisticated understanding also extends to evolving a sophisticated political understanding. This reformulation of politics is evident in the way psychiatrists manage institutions, relationships with third parties, the manner of their participation at various levels of social discourse, and the way in which the RANZCP informs and influences public policy. As one participant said, ‘there's the politics within the professional organization as well as the politics at the bigger level’ (Psychiatrist 13).
Reflection
The value of reflection, evident throughout the data, included reflection upon the tension between personal and professional value systems and how these might be imposed upon the patient:
One can't help but impose one's own assumptions and values on the process, but one would aim to try not to do this as much as possible. (Psychiatrist 6) But on a personal level, it's … it's a very difficult thing to do, to balance the personal and the professional and not be aligned to any particular political interest. (Psychiatrist 1)
A second aspect of reflection was an awareness, not only of the historical failings of the psychiatric profession, but also of the persistence of the preconditions for such events. The example cited by at least three of the participants was that of the abuses perpetrated by a psychiatrist at Chelmsford Hospital in the 1980s. The abuse of power that led to the Chelmsford tragedy was considered to be still possible, prompting one psychiatrist to assert ‘I think we have other Chelmsfords that we need to think about’ (Psychiatrist 3).
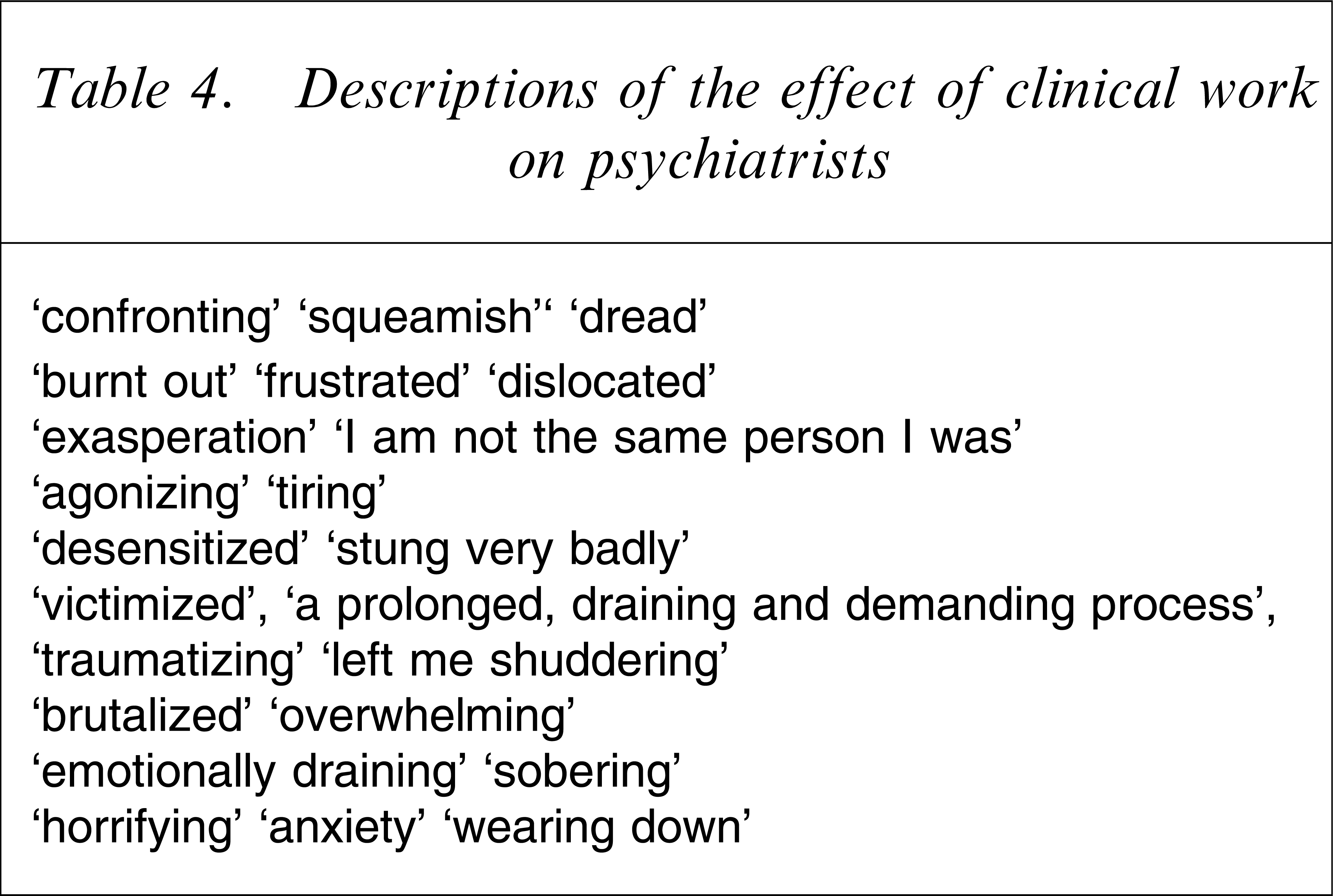
Akin to this point of reflection, was the potential for the misuse of psychiatrists’ knowledge by third parties, such as government agencies or insurers, not only in directly maleficent ways, but also in ways that diminished the patient. The value of reflection also referred to judicious intervention based upon the patient's needs, rather than blanket application of evidence-based treatments. Moreover, there was a need for circumspection, or perhaps a wariness of claims of certainty in the craft of psychiatry. The final aspect of this value was reflection upon protection of the psychiatrist and his or her family in the face of the potential adversity associated with working with severely disturbed or distressed patients. The terms used to describe the effects of such work on the psychiatrists are shown in Table 4.
Descriptions of the effect of clinical work on psychiatrists
Discussion
By our estimation, this is the first empirical study of psychiatric ethics in the Australian setting. This study seems to confirm that empirical methods can be applied to generate models of values for professional groups such as psychiatrists.
Of the four values identified in the study, two require closer consideration because they represent newer perspectives on the values of psychiatrists. First, the value of the individual patient was reflected in the psychiatrists valuing the individual narratives of their patients. While most systems of ethics start with assumptions about human welfare and moral status, patient autonomy has been a central concept in Western bioethics [27–29]. This did not seem to fully explain what the psychiatrists in the present study valued in their patients. The capacity to construct a patient's story through history gathering and observation of mental state is, therefore, regarded as a fundamental skill of psychiatrists. This becomes a joint construction of the patient's narrative. Given the influence of context on the way a narrative is constructed [30], psychiatrists perform ‘editorial roles’ in the course of evaluation and diagnosis. In imposing the structure of diagnosis upon a patient's experience, they risk assuming a ghostwriting role [31]. The necessary skill of ‘narrative competence’ is the capacity to absorb the plight of others in such a process [32].
The value of a patient's narrative form is not a new concept in medicine or medical ethics. As has been said of the craft of medicine:
Patients have always emerged from an encounter with a physician bearing a new story about the nature and significance of their illnesses. Sensitive physicians have generally seen to it that the new story bears the stamp of a particular patient's unique individuality. (p.139) [33]
The importance of jointly constructed narratives as a therapeutic process has also been outlined by Brody [34], in that ‘symbolic healing’ represents the creating of a narrative that has the function of an explanatory system, facilitates care and compassion, and represents mastery and control by the patient over his or her suffering. The joint construction of this narrative requires the full involvement of the patient, and such a narrative must be salient to the patient. In Brody's view, the redrafted narrative must, ultimately, facilitate the patient's progress beyond suffering.
Psychiatric disorders, in particular those arising from the experience of psychological trauma, have a profound effect upon narrative. In the context of psychiatric care, Rorty asked that if all the patients’ grand narratives are questioned in the therapeutic process, where does that leave the individual? [35] The psychiatrists interviewed emphasized the need to acknowledge and integrate contextual, cultural, existential and subjective aspects of the patient's experience in a manner that allowed a diagnosis to be made in a way that did not impose an impersonal and rigid structure on the patient's narrative and, therefore, their personhood or identity. The psychiatrist shares this, but also draws upon this to formulate an understanding of the patient's experience. The uniqueness of the patient's narrative is challenged by the imposition of diagnostic categories as a means of structuring the patient's experience.
Psychiatrists also value the intrinsic resilience of their patients. Resilience has been defined as ‘a self-righting force within everyone that drives him/her to pursue self actualization, altruism, wisdom, and harmony with a spiritual source of strength’ [36]. Resilience represents a distinct trajectory in the face of adversity [37] and derives from the person's identification of developmental assets (such as temperament, cognitive style and intelligence) and their available protective factors, which are integrated and promote individual growth [38]. The practical value of resilience is its psychological protective function [39]. Psychiatrists in the present study valued resilience in their work, and felt compelled to avoid casting their patients, primarily through diagnostic practices, into a victim role, thus diminishing their resilience.
The value of sophisticated understanding resonated throughout the data. All of the participants alluded to the importance to go beyond simplistic approaches to their patient's individual situations to the broader context in which these occurred. Such an understanding escaped the constraints of Engel's bio-psycho-social model [40], which is argued to be eclectic and therefore not intellectually rigorous [41].
Based upon the identified set of values, we now consider how these values are reflected in the relevant principles of the RANZCP Code of Ethics, and propose revisions, as necessary.
Principle 1
Psychiatrists shall respect the essential humanity and dignity of every patient
This principle emphasizes respect for patient culture, ethnicity, language and religion. It proscribes discrimination on grounds of ‘age, gender, race, ethnicity, sexual orientation, disability, language, creed, religion or political affiliation’. It also emphasizes that psychiatrists ought not impose their own values upon patients. In the context of involuntary treatment, it demands that psychiatrists are ‘especially mindful of respect for autonomy’. In caring for a patient whose autonomy is impaired, psychiatrists should respect their ‘essential humanity and dignity.’ The principle emphasizes that the purpose of involuntary treatment is ‘to enhance the patient's welfare and ultimate autonomy’. There is also a requirement that psychiatrists shall obtain informed consent from the patient and show respect for their dignity and privacy in teaching. This principle clearly articulates the value of the patient. The annotations of the principle address the fundamental issue of patient autonomy, which is appropriate given the complexities of autonomy in mental illness and its treatment. The value of ‘the patient’ emergent from the data set incorporates autonomy as one of the constitutive components of this value. It does not, however, of itself, provide a comprehensive account of the concept of the patient's intrinsic value. In order to have a comprehensive ontological grasp of the patient, there appears to be a need for psychiatrists to integrate the value of the patient's identity, being particularly mindful of the vulnerability of identity in the face of diagnostic labels, and psychotropic and psychological treatment. As we have argued, the concepts of identity, self-experience and personhood are based in the patient's narrative, which is also vulnerable to the imposition of structure in the course of psychiatric intervention. The other critical value related to the patient is the need to see the patient and their experience through the prism of their resilience. These considerations may be articulated as an annotation, which might read as follows. Psychiatrists ought recognize that patients’ identities are evident in their unique narrative and their resilience. These capabilities are vulnerable in the context of mental illness and its treatment. As such, psychiatrists have an obligation to consider the impact of their interventions on these domains.
Principle 2
Psychiatrists shall not misuse the inherent power differential in their relationships with patients, either sexually or in any other way
This principle posits that the relationship between a psychiatrist and a patient is inherently unequal (based upon a variety of demographic, cultural and political factors) and that this power differential ought not be exploited. There are a series of pronouncements, which reflects zero tolerance of any form of sexual contact between psychiatrists and patients, and a series of descriptors of sexual harassment. Related to the exploitation of patients by psychiatrists, this principle emphasizes that the use of the power differential shall influence patients only ‘in ways that are consistent with the aims of treatment’. The annotations relating to this principle emphasize the abhorrence of sexual exploitation of the patient and then assert that the evident power differential in the psychiatric therapeutic relationship can be exploited only in ways consistent with treatment aims. Although psychiatrists can act in good faith in gathering clinical information relating to a patient, this information can still be accessed under legislative powers and used against the patient. An example of this is the way in which sensitive information obtained using the interview skills of psychiatrists can be accessed from patient's records by third parties to defend an insurance claim.
In the light of this, we propose an additional annotation to this principle. Psychiatrists should reflect upon the potential misuse of the power differential in their relationships by third parties.
This annotation integrates the value of reflection with the stated concerns about misuse of power.
Principle 3
Psychiatrists shall provide the best possible psychiatric care for their patients
This principle adumbrates the development of a beneficent, collaborative and ultimately therapeutic relationship ‘treating patients under the best possible conditions’, including adequate provisions for continuity of care, thorough documentation and record keeping and the appropriate involvement of the patient's family. Such treatment ought to be holistic, involving consideration of the patient's ‘physical, social and spiritual well-being’, and be sensitive to a patient's cultural background. It endorses discretionary grounds to decline referral of a patient ‘where appropriate and justifiable’.
The Code argues for a degree of self-chastening in that it states that psychiatrists should practise only ‘within the limits of their expertise’ and seek appropriate advice from colleagues. There is a proviso for the use of involuntary treatment as a means of ensuring access to treatment in the case of a patient's impaired autonomy. There is no reference to ‘best practice’ other than the awareness of the ‘relative benefits and risks of psychiatric procedures and treatment’. The code also specifies that psychiatrists should ensure that, in the case of a problem with their own physical or mental health, they should not care for patients when their capacities have diminished.
The annotations for this principle appear quite comprehensive and reflect the four main values identified in the present study. One might propose an annotation calling for the judicious use of evidence-based medicine. This, however, would likely represent an overreach because it is, effectively, attempting to legislate practical wisdom.
Principle 6
Psychiatrists shall not misuse their professional knowledge and skills
This principle outlines that psychiatrists shall not misuse their professional knowledge and skills to advance purposes ‘other than their patients’ interests’. The principle calls for psychiatrists to disclose if an intervention, such as a medico-legal assessment, is not therapeutic. In what is clearly a reference to the abuses of psychiatric diagnosis seen in the former USSR, it deems that psychiatric diagnosis or treatment is not to be based upon a person's political, religious, ideological, moral or philosophical beliefs, race, ethnicity or sexual preference. It also explicitly proscribes the participation of psychiatrists in execution, torture or ‘forms of cruel, inhumane or degrading punishment’. In cases of war, it deems that psychiatrists ought to act within accepted ethical guidelines. The principle is quite explicit in that such behaviour is unethical ‘(w)hatever the legal circumstances’.
This principle raises the problem of relativism in the definition of ‘misuse’ of knowledge or skills. This principle puts psychiatrists potentially at odds with current or future social or political institutions, which may have legislative power over this area. There are already mandatory reporting requirements in many aspects of the psychiatrist's work, such as in relation to child protection and impaired colleagues. Arguably, these pertain to particular knowledge or insights possessed by psychiatrists regarding the patients or colleagues in question. In recent times the involvement of psychiatrists in the interrogation of ‘unlawful combatants’ in Guantanamo Bay has highlighted the tension between the obligations of citizenship and professional ethics [42]. Moreover, institutions such as the military have certain expectations of duty and obedience to power structures within the organization. Although Australian psychiatrists have not, hitherto, been confronted with Guantanamo Bay- or Abu Graib-type situations, Australian law relating to national security erodes civil liberties in similar ways, and individuals have been imprisoned in institutions where psychiatrists have a consultative role. Moreover, psychiatrists have been involved in treatment of detainees in the custody of the Commonwealth Department of Immigration and Multicultural Affairs, in particular advising about the management of behavioural problems within detainee populations. This dual-role problem is a rich theme in the forensic literature, but has not been comprehensively discussed in the mainstream literature of psychiatric ethics.
Any statement relating to the misuse of knowledge (or ‘power’, as in Principle 2) should acknowledge that psychiatrists have to balance their responsibilities to patients with those to society as evident in the social contract [43, 44]. Moreover, it is necessary to assert both that psychiatrists work in legislative frameworks and that their patients often suffer through failures of the social contract. Thus, we propose the following annotations. The first is as follows. Psychiatrists acknowledge that, as professionals, they are party to a form of social contract and practise their medical specialty in specific legislative frameworks. In circumstances in which their patients are disadvantaged by potential failures of the social contract, psychiatrists must balance conflicting obligations to this social contract and to their patients. And the second: Psychiatrists must be aware for the potential of their skills or knowledge to be misused by third parties.
Principle 11
Psychiatrists shall strive to improve the quality of, and access to, mental health services, promote the just allocation of health resources and contribute to community awareness of mental health and mental illness
This principle obliges psychiatrists to promote improvement of mental health services and the just allocation of health resources, including the advising of those responsible for the provision of psychiatric and related health services. It calls for collaboration with others in ‘ensuring that the best possible mental health care and welfare in the community is available to psychiatric patients’. One of the more contentious annotations of this principle argues that when services fall below ‘acceptable standards’, psychiatrists have ‘a duty to advocate for services and take appropriate action. Exceptionally, psychiatrists may have to dissociate themselves from such services, provided this does not put patients at risk.’
The principle acknowledges the need for psychiatrists to inform public discourse on scientific and professional opinion and requires Fellows to exercise restraint in speaking publicly, in particular avoiding gratuitous self-promotion and not traducing colleagues. It also requires psychiatrists to specify if their publicly aired views are against the psychiatric mainstream and whether they are speaking as a private citizen, rather than as a member of the psychiatric profession.
Like Principle 3, the annotations provide a comprehensive account of issues relating to distributive justice and advocacy. The annotations reflect the values evident in the data. The themes emergent from the data, however, may provide some points that make for a richer description of this principle. The first is that psychiatrists appear to value political sophistication, where politics refers to the realm of action in a variety of settings. Moreover, the onion skin model of justice provides a workable account of the limits of appropriate advocacy. The theory of values is at odds with the annotations of this principle, which presents a paradox. Recent experience indicates that psychiatrists not uncommonly encounter systems in which there are inadequate levels of care and where people suffering mental illness experience discrimination. The stipulated action, in response to this, is to disassociate from such settings, if this does not result in patients being disadvantaged. It is hard to imagine a circumstance in which psychiatrists abandoning inefficient health services would not be disadvantageous to patients. Most of the psychiatrists interviewed reflected upon the dilemma of whether to abandon a dysfunctional institutional setting or remain within it and attempt to effect change. The values of ‘sophisticated understanding’ and ‘advocacy’ would not seem to permit such acts. Rather, they would call for forms of advocacy within institutions, regardless of the capacity for systemic change within such institutions. There appears a need for assertive or even aggressive forms of advocacy in such institutions, which reflect the political sophistication valued by psychiatrists. This begs the question: is open conflict with government or bureaucracy an option in the face of moral affronts such as mandatory detention of children, forced removal of children on politically motivated grounds, or the deliberate or reckless running down of mental health services? The answer, according to this data set, appears to be ‘yes’.
In the light of this, we proposed the following annotation for this Principle. In the course of advocating for their patients, psychiatrists may find themselves in varying levels of conflict with institutional cultures or bureaucratic procedures, which fail to provide adequate care for their patients. In such instances, psychiatrists ought to consider carefully their obligations to use their influence in such settings to advocate for their patients’ best interests’.
Conclusion
Based upon the present study there are grounds to argue that empirical methods, particularly qualitative research, can provide a basis for the creation and evaluation of codes of ethics. Such methods allow codes of ethics to be more representative of the views of professional groups than is possible with specific ethics committees alone. Moreover, empirical methods could be used to assay the views of members of society or mental health services patients in regards to their conception of ‘ethical psychiatry’. Ultimately, this may be a way of realizing the true professional contract [44] between psychiatry and the society in which it practices.