
Abstract
A central pillar of the recommended multi-modal treatment approach for attention-deficit–hyperactivity disorder (ADHD) is psychostimulant medication [1]. Around 75% of children who receive an ADHD diagnosis will also receive psychostimulants [2–5]. The effectiveness of psychostimulants in the treatment of ADHD has been demonstrated because they can dramatically reduce ratings of symptom severity [6–9]. The effectiveness of this treatment saw psychostimulant use for ADHD increase significantly in Western nations over the last two decades [10]. (The authors note the controversy around psychostimulant treatment for ADHD. There is continued debate about the possible misdiagnosis or overdiagnosis of ADHD and whether psychostimulant treatment is warranted in the case of every young person diagnosed with ADHD. The data used for the present study provided no information on diagnosis, only that medication had been prescribed (a process that legally requires diagnosis in this jurisdiction). Thus, the matter of appropriateness of psychostimulant treatment is beyond the scope of this paper. For more detailed discussion of the issue of diagnostic practices, we note the first author's book [11].)
Due to the prominence of ADHD in the USA, this nation provides a useful context against which to compare recent Australasian trends. Between 1990 and 1997, the production of methylphenidate in the USA rose from 1788 kg to 13 824 kg, with the majority of extra production being used for ADHD treatment [12]. Estimates of the number of US children using psychostimulants between 1987 to 1995 rose from 750 000 to 2 million [13, 14]. Other estimates claim a doubling in the number of children between 1990 and 1995, and a further doubling by 2000 [15],[16]. Recent estimates vary between a survey of parents that reported 4.3% and a study that found that 7.8% of children received psychostimulant medication [17, 18]. Specific details on the prevalence of psychostimulant use are difficult to ascertain because there is a high variation in national, regional and local data [19–21]. Some US estimates have been as low as 0.4% in one county in New York, [22] while other estimates have been as high as 23% [23]. These figures need to be viewed cautiously because a number of factors may influence the variability in psychostimulant rates [24], such as the problems of data collected over different periods, with different populations, across different locales, and with disparate methods.
In the Australian context, between 1984 and 2000, there was a 26% increase per year in the total rate of consumption of dexamphetamine and methylphenidate per year, while from 1994 to 2000 the rate of total psychostimulant consumption increased 8.46-fold (compared with the period 1984–1993) [25]. Australia's total consumption of dexamphetamine during the period 1984–2000 for all States showed an average increase of 31% per year and a 30% per year increase for methylphenidate [25]. A recent study in Western Australia found that the rate of stimulant prescription was 2.3–5.3-fold greater in major cities compared with remote and very remote parts of that State [26]. In the present study the association between socioeconomic disadvantage and the rate of stimulant prescription was highly variable in different jurisdictions [27–29].
Other areas that lack clear data include which Australian children are treated with psychostimulants and for what duration. Although past studies suggest that most students start psychostimulant use around 7 years of age [30, 31] and that usage peaks at 9–10 years [32], there is still limited information about the age at which children start treatment and the duration of that treatment. Reports based on US regional data estimate that duration of psychostimulant treatment ranges between 8 years for high school students and 5 years for middle school students [33], with an average of 4 years for all students [2]. The duration of psychostimulant treatment for most children, however, essentially remains unknown.
Socioeconomic status (SES) has been identified as a risk factor for ADHD diagnosis [34] (due to a link with environmental or psychosocial stressors [35] and the tendency of teachers to rate hyperactivity higher in students of lower SES) [36, 37], although there are conflicting international accounts of the links between income and psychostimulant use [10, 38, 39]. In the Australian context there are lower levels of psychostimulant use among indigenous [40] and Asian populations [41], while in New Zealand the prevalence among the Maori population reflects that of the broader population [42]. This also raises the role of ethnicity in the acceptance of psychostimulant treatment.
Throughout the 1990s Australia and New Zealand closely paralleled the American increase in psychostimulant use [10, 38, 42]. In New Zealand, between 1992 and 2003 Ritalin prescriptions rose from just under 3000 to almost 70 000 prescriptions, while dexamphetamine prescriptions grew from <1000 to around 5000 in the same period [42]. Currently, levels of psychostimulant use in Australia and New Zealand approximate those of the USA [11, 27, 28, 43]. In summary, there is an urgent need for studies that provide more stable estimates of how many children (with which demographic characteristics) are taking psychostimulants for ADHD and for what duration. This information has important clinical implications in the integration and effective functioning of pharmacological and other interventions.
In a previous paper we reported analysis of psychostimulant use in the state of South Australia for the period 1990–2000 [29]. This paper found that the rate of prescriptions grew dramatically until 1995, but then rates of psychostimulant use aligned with the average for Australia as a whole [43]. We found that demographic characteristics mirrored those of the USA, with more boys medicated and the majority of cases in the 5–9-year-old age range. In the study, the median duration of psychostimulant use was approximately 2.5 years and there was pronounced geographic variability in prescription rates (which significantly correlated with SES). Surprisingly, there was also pronounced variability in the yearly rate of new prescriptions as we documented a rapid increase in the number of new prescriptions for psychostimulants, along with a sharp decline after 1995.
In the present paper we revisit the South Australian content to provide new data on psychostimulant use covering the years 2001–2006. This allows comparisons between 1990–2000 (the period in which the majority of psychostimulant treatment began), and 2001–2006 (the period in which psychostimulant treatment had become well established). We report data on yearly prescription rates, demographic information, duration of psychostimulant use and geographic variation (including SES). We hypothesized that (i) the demographic characteristics of children in relation to starting age and male:female ratio within this sample would not differ across the two periods; (ii) the rate of new cases in this sample would stabilize; and (iii) the correlation between low SES and psychostimulant use would remain significant for the period 2001–2006.
Methods
Data used for the present study were archival records of children who received prescriptions for psychostimulants provided by the South Australian Health Commission (SAHC). Psychostimulants are classified as ‘drugs of dependence’ and in South Australia medical practitioners are required to obtain an authorization from the SAHC to treat a patient for periods >2 months. This data set consisted of all children (birth–18 years) who had been authorized to receive psychostimulants in the city of Adelaide. Metropolitan Adelaide has a population of >1 million people and comprises >70% of the total population of South Australia. Data for 7849 cases are presented spanning the periods 1990–2000 (5189 cases) and 2001–2006 (2660 cases).
Data provided by the SAHC include gender, date of birth, date of psychostimulant authorization, date of last contact (which indicates when authorization ceased), postcode and status. Status was defined by the SAHC as either ‘active’ (i.e. the child was authorized to receive psychostimulants) or ‘ceased’ (i.e. the child was no longer authorized to receive psychostimulants). From these data we calculated the start age (date psychostimulants authorized minus birthdate), duration (date ceased minus date psychostimulant authorized), and the number of children beginning psychostimulants per year. Postcode was used as a geographic marker because it covers a small and homogeneous population grouping. There are 125 postcodes in the Adelaide metropolitan area. Eight postcodes that cut across the metropolitan Adelaide boundary (and covered a very small population) were excluded. The mean population of the postcodes was 8607 (SD = 1960).
Population and socioeconomic figures on postcodes were obtained from the Australian Bureau of Statistics (ABS). For the period 1990–2000 we used census data from 1996; for the period 2001–2006 we used census data from 2001. Standardized medication ratios (SMRs) for each postcode were computed using indirect standardization. The ratio of observed counts to expected counts for each postcode were derived by calculating age–sex stratum-specific proportions (using the entire Adelaide population as the reference) and multiplying these proportions with the stratum-specific populations and summing the product. The SMR for each postcode was calculated by dividing the observed number of children with prescriptions by the expected number (SMR > 1 indicates more cases were observed than expected). To assess the relation between SES and psychostimulant rates for postcodes, we used the ABS Index of Relative Socioeconomic Disadvantage (IRSD) [44]. The IRSD considers factors such as educational levels, income, and unemployment. A high score suggests that a postcode has higher income families, more educated people and lower unemployment.
Influencing the data was a shift in the status category used by the SAHC to indicate whether a child was authorized to receive psychostimulants midway through the 1990s. Until 1994, practitioners were required to re-authorize treatments yearly. Due to an increase in the number of authorizations that occurred throughout the 1990s, the SAHC was unable to handle the volume of requests on a yearly basis. This demand resulted in a change in policy. After 1994 physicians were no longer required to request yearly re-authorizations, instead the initial authorization was valid until the child reached the age of 18. Physicians were asked to report voluntarily when a child ceased psychostimulants, but it is highly unlikely that physicians reported all patients who had ceased. The introduction of an improved data system by the SAHC in 2005 identified many inactive cases and deleted them. For this reason we report duration data for only those who were reported to have ceased.
Results
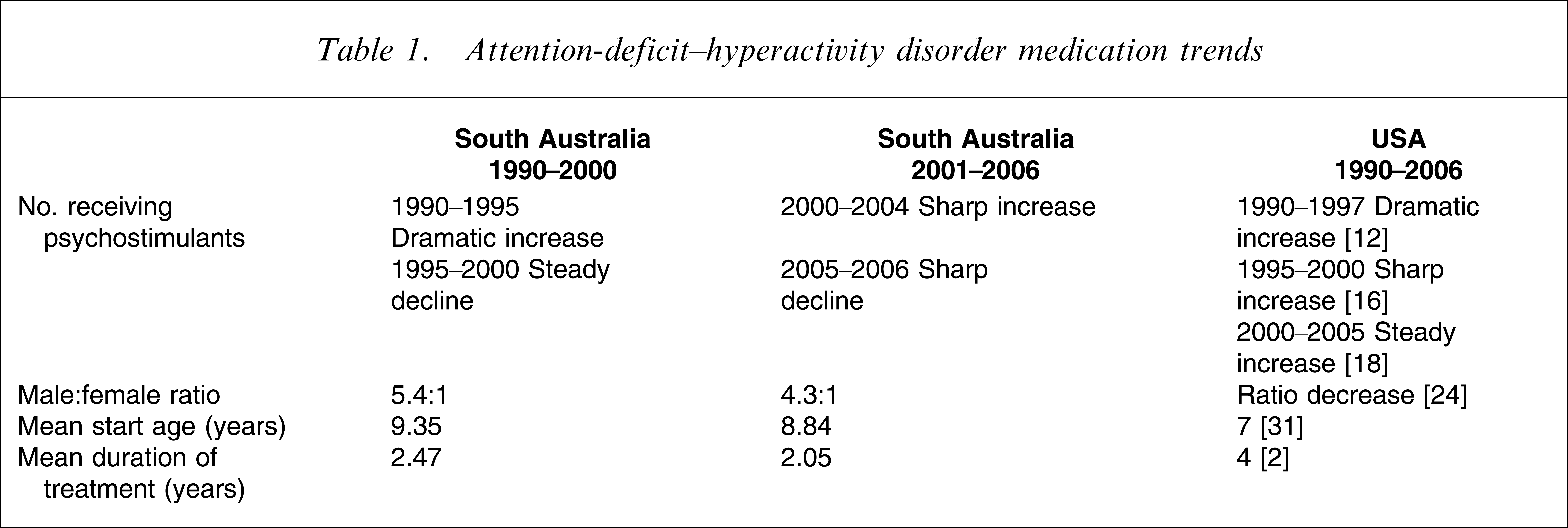
Table 1 provides a comparative overview of the results for the periods 1990–2000 and 2001–2006.
Attention-deficit–hyperactivity disorder medication trends
Prescriptions by age group
Figure 1 shows the number of children per thousand of the population beginning psychostimulants from 1990 to 2006 (according to age group). The number of children receiving psychostimulants increased markedly from 1990 to 1995, after which it began to decline noticeably. Interestingly, in 2000 the number of new authorizations approximated the numbers of 1992. In 2000 the numbers again began to increase, a trend that continued until 2004. Numbers decreased sharply, however, in both 2005 and 2006. As expected, 5–9-year-olds received the majority of the new prescriptions, followed closely by 10–14-year-olds. These increases (and decreases) in prescriptions by age were due to changes in the number of boys receiving prescriptions, while rates for girls showed a slower increase.
Rate of new psychostimulant medication prescriptions per year by age group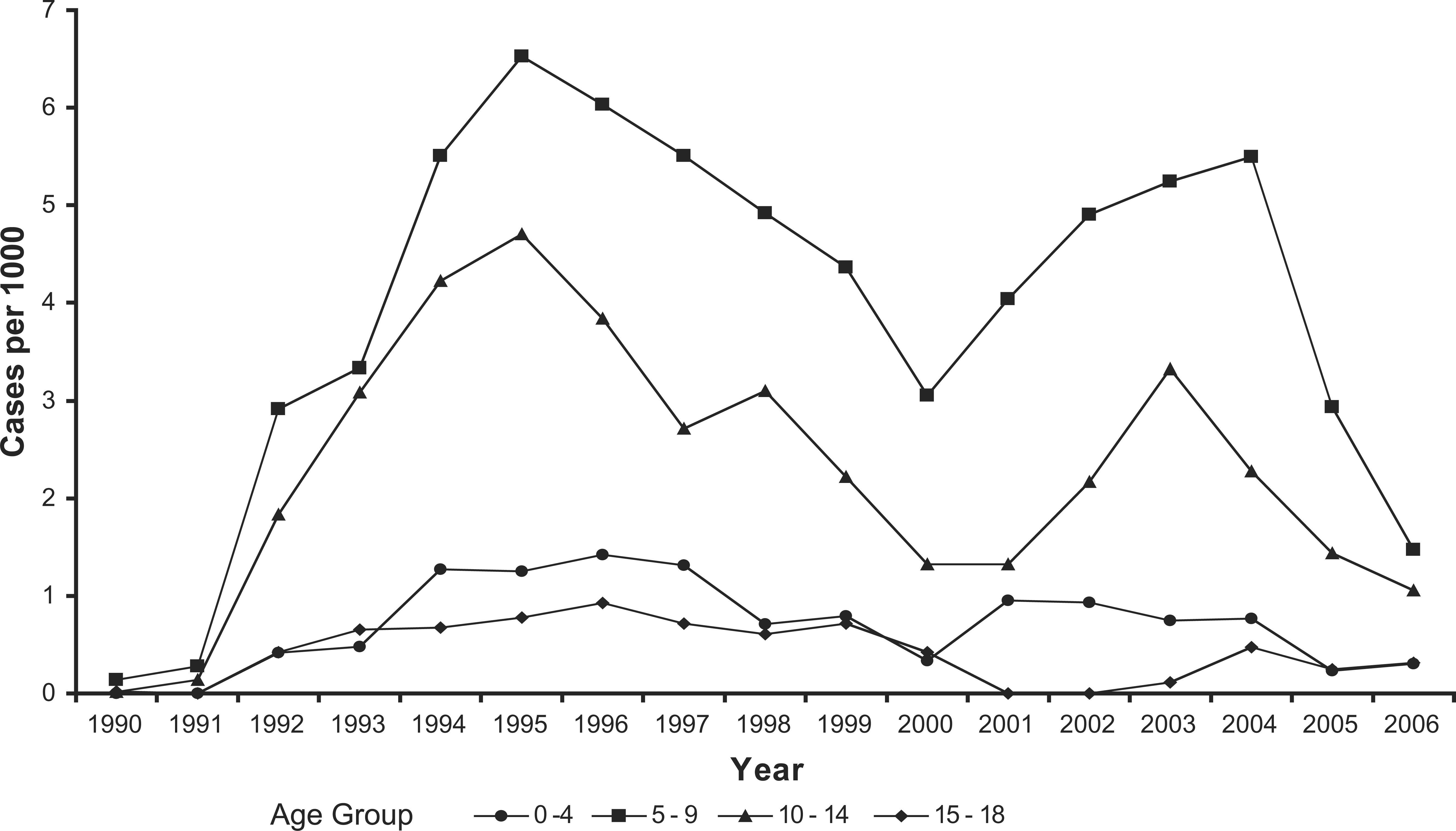
Prescription by gender
From 1990 to 2000 the overall male:female ratio was 5.4:1, while from 2001–2006 the overall male:female ratio changed to 4.3:1. The difference in male:female ratios across the two periods was significant (χ2=7.8, p = 0.005, df = 1). Thus, there was an overall decline in male:female ratio during the period 1990–2006. There was also considerable variability within each period. From 1992 to 2000 the male:female ratio exhibited a high of 7.7:1 (in 1993) and a low of 4.3:1 (in 1998), but the changes within this period were statistically significant (χ2=22.63, p = 0.003, df = 8; note: 1990 and 1991 were excluded due to low numbers). From 2001–2006 the male:female ratio exhibited a high of 5.97:1 (in 2002) and a low of 3.46:1 (in 2006). Again the changes within the 2001–2006 period were significant (χ2=11.27, p = 0.046, df = 5).
Prescription by start age
Figure 2 shows a box plot of the median age at which children began psychostimulants between 1992 and 2006 (1990 and 1991 were excluded due to low numbers). For the period 1990–2000, the average age at which children started was 9.35 years (SD = 3.25). The average start age for boys and girls was 9.41 years (SD = 3.21) and 9.02 years (SD = 3.39), respectively, while the difference between the two was significant (F(1,5188) = 10.32, p = 0.001). For the period 2001–2006 the average age at which children started was 8.84 years (SD = 2.88). The average start age for boys and girls, respectively, was 8.74 years (SD = 2.81) and 9.28 years (SD = 3.15), and again the difference was significant (F(1,2658) = 14.48, p < 0.001). Median start age varied between a low of 7.80 years (in 2001) and a high of 9.87 years (in 1993). Results of a 2 (time period)×2 (gender) ANOVA showed that there was a significant difference in start age across time periods (F(1,7845) = 4.40, p = 0.036), and that there was a significant period×gender interaction (F(1,7845) = 23.11, p < 0.001). Thus, the average age of starting psychostimulants declined slightly over the period 1990–2006, but there was no significant main effect for gender.
Median age of starting psychostimulants (years) for 1992–2006.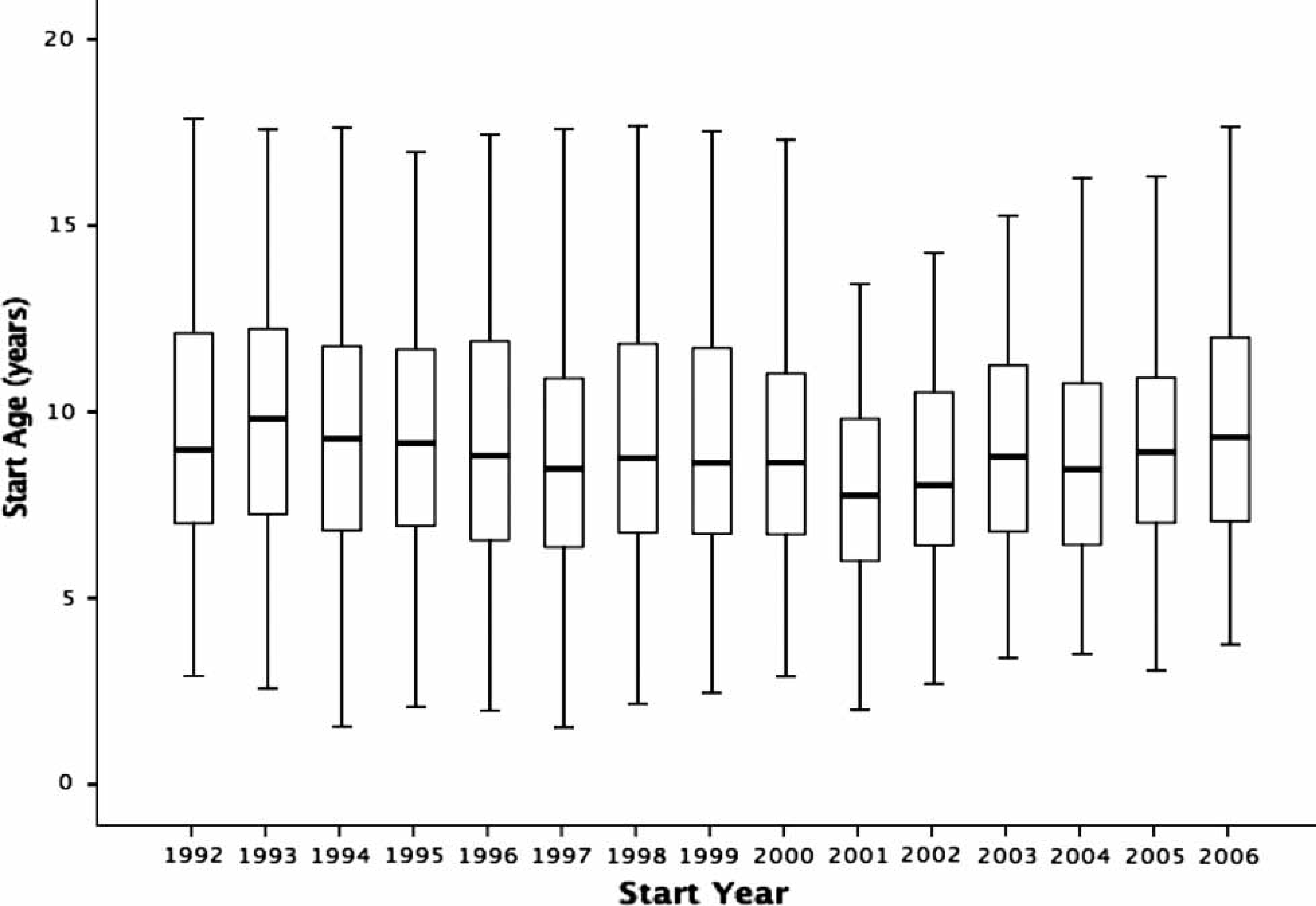
Duration of psychostimulant treatment
From 1990 to 2000, 1688 children (1410 boys, 278 girls) were reported as having ceased psychostimulant use. Of these cases, 945 (56%) were from the period 1990–1994 and 743 (44%) were from 1995–2000 (which is after the reporting procedure changed). For those reported as ceased, the mean length of treatment for boys and girls was 2.87 years (SD = 1.94) and 2.85 years (SD = 1.75), respectively, and there was no significant difference between boys and girls in treatment duration. Mean treatment length was 2.47 years. For the years 2001–2006, 302 children (219 boys, 83 girls) were reported as ceased. The mean length of treatment for boys and girls, respectively, was 1.98 years (SD = 1.64) and 2.27 years (SD = 1.48) and the mean treatment length was 2.05 years. Although the duration of treatment declined during the period 1990–2006, there was no significant difference in treatment duration between boys and girls.
Prescription by geographic variation
For the period 1990–2000, the SMRs of observed versus expected rates by postcode ranged from 0.49 (indicating that only half as many children as expected had received prescriptions) to 3.42 (indicating that more than threefold as many as would be expected). Seventeen postcodes had significantly lower rates (p < 0.05) than would be expected and 16 had significantly higher rates than expected (p < 0.05). The Pearson correlation between SMR and IRSD was significant (r = − 0.46, p < 0.01). For 2001–2006 the SMRs ranged from 0.15 (i.e. fewer than one-sixth of expected children had received prescriptions) to 3.23 (i.e. more than threefold as many as expected). The discrepancy between observed and expected rates was significant for 25 of the postcodes: of these, 12 had significantly lower rates (p < 0.05) than expected and 13 had significantly higher rates than expected (p < 0.05). The Pearson correlation between SMR and IRSD was significant (r = − 0.36, p < 0.01). Thus, postcodes with lower SES were associated with increased likelihood of receiving psychostimulants in both the 1990–2000 and 2001–2006 periods.
Discussion
The present results show that the demographics of children in South Australia receiving psychostimulants are similar to those of children in the USA. The average age at which treatment began was consistent with previous research, as was the increase with age, peaking at age 9 or 10 years. The ratio of boys to girls was also consistent with other studies. The male:female ratio exhibited considerable variability across and within time periods, ranging from approximately 3:1 to 6:1. The overall trend, however, was toward a lower male:female ratio. The age at which psychostimulant use started appears to be trending downward as the mean start age decreased by approximately 6 months between the 1990–2000 period and the 2001–2006 period. There were differences across gender in start age. Although there was little change in the mean start age for girls across the two periods (9.02 vs 9.20), the male mean start age decreased from 9.41 to 8.74 years. Thus, the trend toward starting psychostimulants earlier was primarily the result of increased numbers of boys receiving at an earlier age. Increases in the rate of young children receiving psychostimulants have been noted previously [45], but the change in mean start age was small (around 8 months).
One of the most surprising aspects of the data was the variability in the rate of new cases per year. The data included a large population and we expected much more stability. The rapid increase in the period from 1990 to 1995 can be explained when one considers that the rate of psychostimulant authorization for the decade prior to 1990 was essentially nil (and rates were in effect catching up with the 3–5% rate at which ADHD is thought to occur). After these children had been accounted for, however, we expected that the rate would then decrease slightly and stabilize because the treatment population had been identified and treated [26]. Instead, there was a marked decrease across the two major age groups (5–9- and 10–14-year-olds) between 1995 and 2000. This was followed by another increase (in 2004) to reach near 1995 levels, which in turn was followed (in 2005) by an abrupt drop in numbers to those approximating 1992 levels.
There is no obvious explanation for the changes observed in the present study. One possible explanation is that in each Australian State a relatively small number of physicians can account for a disproportionate number of new prescriptions. For example in Western Australia, five of 59 registered paediatricians account for 26% of prescriptions statewide [46]. Changes in this group (e.g. relocations, retirement etc.) could result in significant changes in the rate of new psychostimulant prescriptions. Further, in small and discrete urban communities such as Adelaide, unique factors such as media reports, public events or changes in policy [10, 39] can have significant implications. Such factors are worthy of future research in their own right.
In relation to duration of psychostimulant use, results are consistent with recent reports that found median duration to be approximately 2.5 years [45] and that 36% of children discontinued within 1 year [47]. The present data showed that half the children in the subset reported receiving psychostimulant treatment for <3 years. This finding has significant treatment ramifications. Because children were most likely to start medication before age 9, many will have ceased psychostimulants before the end of primary/elementary school. Studies in Australia also found that current inclusive education policies struggle to provide non-pharmacological resources for students with ADHD behaviours [48–50]. Further, in Australia only a small percentage of parents are able to access school-based or mental health services for their children, with costs of services and long waiting lists frequently cited as barriers [51]. This suggests that many students may receive no treatment for ADHD for the majority of their time in school. We would caution that the results from the 2001–2006 period should be interpreted very judiciously due to the fact that relatively few children were reported as ceased compared to the previous period.
In relation to regional and socioeconomic variation, previous studies have reported distinct differences in the rate of psychostimulant use between different countries [25] and across the USA [31, 52]. There are also regional differences in Australia as is demonstrated by a 2003 rate of psychostimulant use in Western Australia that is double that of next highest State and almost fourfold the national average. [25–28] The present results show that there can also be considerable variation even within a limited geographic area, such as the Adelaide metropolitan area. There was a 20-fold difference between the highest and lowest SMR in the present study, with the correlation between SES and SMR significant for both periods. The highest SMRs tended to be in areas that are predominantly lower SES with high unemployment. This result is consistent with that of the Calver et al. study, which found that boys from socioeconomically disadvantaged regions had higher rates of psychostimulant use. [26]
Limitations
The present data must be interpreted cautiously. First, because of the changes in authorization procedures there was no way to determine the number of children who ceased psychostimulants after 1995. The data show that the number of children reported as ceased decreased markedly after 1994, but whether this indicates an increased duration of psychostimulant use or simply that physicians were not reporting children who ceased treatment cannot be determined. Thus, it is not possible to generalize the data from the subset of children who were reported as having ceased psychostimulants to the entire sample. Second, these data do not include children who ceased within 1 month of starting medication and were not required to be reported to the SAHC. Third, children who ceased psychostimulants may have been switched to other medications (e.g. antidepressants), which would not be reflected in theses data. Finally, because of the small numbers of student reported as ceased in the 2001–2006 period it is uncertain if the results would generalize to the entire sample.
Finally, the present data addressed the relationship between psychostimulant use, income, unemployment and SES at the level of statistical region (which approximately related to postcode). The data did not address diagnosis, treatment and SES on the individual level. Thus, it should be noted that there can be significant variations in SES within statistical regions, and although the present study suggests a correlation between lower SES regions and higher rates of medication use, it should not be assumed to be a causal link between low-income families and psychostimulant treatment.
Clinical implications
The data on duration of medication suggest that significant numbers of children receive psychostimulant treatment for ADHD for a relatively short period, and many children may be untreated during much of childhood and adolescence. Unless there are other supports in place (e.g. educational accommodation, behaviour modification, counselling) there could be increased risk for adverse outcomes. Further, if medication is to be the mainstay of a treatment programme, children must be maintained on an appropriate (and properly monitored) course of psychostimulants.
In sum, the present results suggest that the demographics of children receiving psychostimulants in Australia are similar to those in the USA. Although the magnitude of psychostimulant use is smaller, the overall patterns of use across age and gender were extremely consistent. The yearly rate of new cases, however, is extremely variable and should receive continued attention. Until now, duration of treatment has received relatively little research, and the present study indicates that it is an important aspect of future treatment planning. Further, an understanding of why children cease psychostimulants and how transitions are supported, as well as the success of treatment should be the focus of future research. Finally, the complex relationship between SES and psychostimulant use remains largely unexplored and could provide important insights for more effective and equitable treatment practices in the future.
Footnotes
Acknowledgements
The authors thank Geoff Andersen, Senior Pharmacist, Environmental Health Services, South Australian Health Commission, SA Department of Health.