
Abstract
Keywords
In recent years the notions of secondary and vicarious traumatization have been theoretically developed, and these constructs have captured the interest of many professionals working in the field of trauma support. Many simply assume that such traumatization inevitably exists, but there has been some difficulty in building a body of quality empirical support. Considering that ‘compassion fatigue workshops’ and ‘vicarious trauma treatments’ are being offered to therapists who work with trauma populations (www.vicarioustrauma.com), an empirical base for these assumptions is becoming more desperately needed. Combining these workshops with debriefing training (www.cisfma.org.au) raises even more concerns regarding the need for an evidentiary basis.
It makes intuitive sense that engaging with another person in an empathic relationship characterized by the identification with and understanding of their emotional experience, similarly impacts upon the emotional experience of the therapist, both at a conscious and subconscious level. Borne through anecdotal report, the notion that prolonged occupational exposure to demanding interpersonal situations with inadequate support can lead to psychological strain in some people has been around since the early 1970s. While burnout has remained a well-researched construct among a range of professions, including mental health, more recently secondary trauma-related constructs such as compassion fatigue, secondary traumatic stress (STS), and vicarious trauma (VT) have been developed and used to describe the impact on mental health professionals of working therapeutically with traumatized people. These constructs have greatly influenced thought and research around therapists’ emotional well-being for the past 10 years, despite the original and broader construct of burnout possessing more sophisticated and robust empirical validation.
Burnout is currently conceptualized as a ‘psychological syndrome in response to chronic interpersonal stressors on the job’ [1]. The three dimensions of the syndrome identified through the Maslach et al. early factor analytic research have been retained over the years: ‘overwhelming exhaustion’ or feeling depleted of one's emotional and physical resources (which is the central ‘stress’ quality of burnout); feelings of cynicism and detachment from the job; and a sense of ineffectiveness and lack of accomplishment [1]. Work overload, limited support, role conflict and role ambiguity have been consistently associated with burnout [1] and are considered its primary antecedents. Research has also found that burnout tends to be more prevalent in younger ‘helping professionals’ [1–3] than in those aged 30–40 years and over – a finding that is confounded by work experience and survival bias. Perceived social support has also been found to be a significant predictor of burnout [4, 5]. For therapists, caseload satisfaction [6], job stress and support of supervisors and colleagues [7] have been associated with burnout.
Another body of research and theory that has developed in parallel to that of burnout is VT. While also addressing the deleterious effects experienced by therapists as a result of chronic interpersonal stressors, VT is theorized to be the ‘cumulative transformative effect upon the trauma therapist of working with survivors of traumatic life events’ [8]. According to Pearlman and Saakvitne VT has its theoretical basis in constructivist self-development theory (CSDT). Critical of symptom and event-focused approaches to trauma therapy as conveying ‘little awareness of the whole person’ (p.56), CSDT attempts to understand an individual's adaptation to trauma as an interaction between personality, personal history, the traumatic event and its social and cultural context [8]. The underlying assumption of CSDT is that ‘the meaning of the traumatic event is in the survivor's experience of it’ (p.57), and that construction of meaning occurs and recurs as new information and experiences are incorporated into an individual's beliefs and systems of meaning. This premise is believed to be fundamental to therapeutic change. The authors propose that given this understanding of how trauma impacts on the individual, it is theoretically inevitable that, chronically exposed (vicariously) to patient's trauma and their struggle with it, therapists undergo a similar transformation over time.
Although the construct of VT has a theoretical framework, there is little empirical validity testing of either the construct or the sole measure used to assess it (Trauma Stress Institute–Belief Scale; TSI-BS) [9]. The primary empirical studies of VT have found that higher levels of exposure to traumatized patients is a significant predictor of VT [10, 11], although other studies have contradicted this, finding no difference between trauma and non-trauma therapists on VT [12, 13]. Some studies have found that a personal history of trauma predisposes therapists to VT [10, 14], yet others found it had no impact [11]. It has been claimed that evidence to support VT is ‘meagre and inconsistent’ [15] despite its theoretical basis. The common factors that Pearlman and Saakvitne proposed to contribute to the aetiology of VT in therapists include: exposure to trauma patients; the chronicity of trauma work; the individual's capacity for emotional empathy; and a history of personal trauma [8].
According to its proponents, STS is the term used to describe the ‘rather natural consequence of caring between two people, one of whom has been initially traumatized and the other whom is affected by the first's traumatic experiences’ [16]. Figley further defined STS as a syndrome of symptoms ‘nearly identical to those of PTSD’, including symptoms of intrusion, avoidance and arousal, and that it can develop following just one incident [17]. STS was a phenomenon posited in the mid-late 1990s, following a revision to the DSM in 1994 [18], which altered the diagnostic criteria for post-traumatic stress disorder (PTSD). Rather than developing anecdotally or through theory, it appears that the strongest influence for the development of STS was a shift in the diagnostic criteria for PTSD, when definition of criterion A of ‘traumatic event’ was broadened to include witnessing or hearing about threatened death or serious injury occurring to another individual [18].
In the past STS was known as ‘compassion fatigue’, but in 1999 Figley renamed it as STS, and one of his most recent positions is that ‘compassion fatigue is a more user friendly term for secondary traumatic stress disorder’ (STSD) [17], which is nearly identical to PTSD, except it affects those emotionally affected by the trauma of another (usually a patient or a family member) (www.giftfromwithin.org). While the distinction between STS and compassion fatigue has not been clearly delineated, and the two terms are frequently used interchangeably, compassion fatigue has been described in the literature as ‘a form of caregiver burnout’ [19], which consists of three distinct factors. It incorporates the symptoms of intrusion, avoidance and hyperarousal typical of STS, but re-labels this factor ‘compassion stress’; while also including a ‘burnout’ factor and the protective factor of ‘compassion satisfaction’, or satisfaction derived from therapeutic work. According to Figley these factors are predictive of an individual's susceptibility to developing compassion fatigue, although there is no clear theory underlying how the factors interrelate, or to describe the aetiology of the condition. In 2003 Salston and Figley recommended eliminating the burnout component, which had been arbitrarily attached to the original theoretical focus of STS, because it acted to diffuse the construct and was not well correlated with the MBI, a well-validated measure of burnout. As such, the initial conceptualization of STS will be used in this study, defined as ‘a syndrome of symptoms parallel to post-traumatic stress disorder’ [20]. STS will not be used interchangeably with the term ‘compassion fatigue’ because the constructs are clearly distinct.
There is a paucity of literature for STS, with only a small number of independently peer reviewed studies published. The independent research to date suggests that symptoms of post-traumatic stress among those who are secondarily traumatized are not at a severe level [21–23], although Figley reported much greater prevalence of STS [19]. In a study of 100 psychotherapists in outpatient mental health agencies, Kassam-Adams used the Impact of Events Scale to measure symptoms of STS [24, 25]. Associations have been found between STS and high levels of exposure to traumatized patients, a personal history of trauma, and gender.
Research into the impact of trauma work on therapists has typically been limited by a lack of clarity around the concepts used, compromised designs and the use of measures the validity of which are yet to be sufficiently tested. This aside, there is some evidence to suggest that the negative effects of secondary exposure to trauma are overestimated, and that symptoms of STS and VT may not be dependent upon trauma exposure. There has been only one study published that used a control group to compare the constructs of STS and VT among trauma and non-trauma therapists. Van Minnen and Keijsers found that for their sample of 20 trauma therapists and 19 non-trauma therapists, that there was no significant difference between the groups on measures of STS, measured using subjective reports of PTSD symptoms and general distress (Symptom Checklist-90-R total score), nor was there a difference on VT scores [26, 27].
There is confusion regarding the terminology used in the area of secondary traumatization. For the purpose of this study, the following definitions were used: ‘burnout’: ‘emotional exhaustion; feelings of cynicism and detachment from the job; and a sense of ineffectiveness and lack of accomplishment’ [1]; ‘vicarious trauma’ (VT): the ‘cumulative transformative effect upon the trauma therapist of working with survivors of traumatic life events’, which specifically impact on ‘the identity, world view, psychological needs, beliefs and memory system of the therapist’ [18]; and ‘secondary traumatic stress’ (STS): a syndrome of symptoms ‘nearly identical to those of PTSD’ [17] including symptoms of intrusion, avoidance and arousal, which is ‘the natural consequence of caring between two people, one of whom has been initially traumatized, and the other whom is affected by the first's traumatic experiences’ [16].
The present study differs from previous studies conducted in the area in that it examined the three constructs of STS, VT and burnout together rather than assuming that they are distinct. It also used mental health professionals who predominantly treat trauma patients as well as a control group of non-trauma therapists, foregoing the assumption that it is trauma work per se that leads to STS and VT as it is currently theorized and measured. The aims of the current study were (i) to determine the discriminant and construct validity of the measures for STS, VT and burnout; (ii) to determine whether the constructs of STS, VT and burnout are actually measuring different things; (iii) to determine what impact, if any, trauma work has on therapist distress; (iv) to determine whether the trauma-related constructs contribute significantly to the prediction of ‘affective distress’, beyond that attributed by burnout; and (v) to determine what VT contributes to the prediction of affective distress, beyond burnout. Based on the research discussed here, it was hypothesized: (i) that STS and VT scores are more convergent with each other and affective distress than is acceptable for construct validity; (ii) that STS and VT are not sufficiently discriminated from burnout; (iii) that when the predictors for burnout and VT are used in a regression model for STS, the model will fit the data as well or better than when the theoretical predictors of STS are used; (iv) that when the predictors for burnout and STS are used in a regression model for VT, the model will fit the data as well or better than when the theoretical predictors of VT alone are used; (v) that when work factors such as ‘hours worked each week’ and ‘work stress’ are held constant, there is no significant difference between therapists with high and low exposure to trauma patients on measures of STS or VT; (vi) that burnout and VT will both contribute significantly to the prediction of affective distress, because they are measuring similar phenomena, but that burnout will contribute the most; and (vii) that all of the domains of cognitive schema encompassed by VT will predict affective distress among this sample of therapists equally well.
Method
Participants
Participants were 152 volunteers (45 men, 107 women) aged >18 years. All participants were mental health professionals working in Victoria, Australia, including psychologists (n = 125), psychotherapists (n = 15), clinical social workers (n = 6), a psychiatrist (n = 1), a nurse (n = 1) and other (n = 4). Currently, in Victoria there are 1457 male (24%) and 4555 female psychologists (76%) with general registration (Psychologists Registration Board of Victoria, February 2008). The present sample consisted of 29% men and 71% women and thus was representative of the gender distribution of the Victorian psychologists (p = 0.11).
An a priori power analysis using Clintools [28] indicated that a total sample size of approximately n = 126 would be required to provide sufficient power (0.8) for the primary analyses. This was calculated assuming at least a medium effect size (d = 0.5) and an alpha level of 0.05 for a two-tailed test. Other studies in this field using direct mail-out recruitment procedures recorded response rates of 32% [10] and 37% [24], so a minimum response rate of approximately 32% was expected. We also expected 5% of the responses (at the most) to be incomplete due to the substantial size of the questionnaire. A sample size of at least n = 126 was needed, so it was determined that 480 potential participants would need to be approached.
Participants were recruited using a number of approaches. One-third of the total potential participants were directly approached by email or post using contact details obtained from publicly available databases (the Australian Association of Cognitive Behavioural Therapists member database and the telephone book listings for psychologists, counsellors, psychotherapists and social workers in Victoria, Australia). A random number generator [28] was used to randomly select 160 names from a possible 2385. The remaining two-thirds of the total potential sample (n = 320) was randomly selected from a database of 900 therapists who have experience working with victims of crime, through the Victims Support Agency in Victoria, Australia. Other participants were recruited by placing a brief advertisement for the study in an online newsletter for psychology and psychiatry alumni of the University of Melbourne. All potential participants were sent a letter outlining the details of the study and what was required of them, the weblink to the online questionnaire battery and the contact details to request a postal paper copy of the questionnaire battery, should they prefer this method of data procurement. All potential participants were asked to participate only if they were engaged in clinical therapeutic work. The total response rate for the study was unable to be estimated considering the use of electronic advertising. The response rate for the direct mail-out, however, where respondents did not opt to confidentially submit online, was 32% – remarkably consistent with that in the Pearlman and MacIan study [10].
All participants who completed the postal version of the questionnaire signed and returned a consent form. All of those who completed the online questionnaire read an online consent form and checked a box indicating that they provided informed consent.
Measures
Demographics and work-related variables
General demographics were obtained, including questions related to age, gender, marital status, the number of children the participant had both under and over 10 years of age, education level, employment status, average time spent with each patient, primary therapeutic orientation, profession, average hours worked per week as a mental health professional, duration of career as a mental health professional, average number of patients seen per week, average number of days taken off (vacation and sickness) over a 3 month period, patient groups worked with, any therapeutic specialization, whether they work for themselves or an organization, whether they work in a team (and the size of the team), whether they received workplace orientation/induction, and the average number of hours of supervision accessed per month.
The variable ‘work stress’ is an index of four categorical scales (5 point Likert-type scales), which measure the participant's perception of whether the workplace is supportive, whether their workload is reasonable, whether demands placed on them at work are conflicting and whether they have a clear idea of what is expected of them at work. These scales are frequently used in research to provide a quantitative measure of an individual's perception of workplace stressors, and research has indicated that they consistently correlate with burnout [1]. Participants were also asked to rate their satisfaction with work as a mental health professional.
With respect to trauma work, participants were asked to indicate the proportion of their caseload that is dedicated to working with trauma patients, whereby the effects of the trauma are directly addressed (the DSM-IV definition of a traumatic experience was included to reduce individual variability regarding what constitutes a trauma). Responses on this question were used to classify participants into quartiles, whereby the lower quartile are considered to have low exposure to trauma cases and those in the upper quartile are considered to have greater exposure to trauma cases. If the participant indicated engaging in trauma work, they were also asked to indicate the duration of their career spent working with trauma patients, hours per week spent working with trauma patients in which trauma-related issues are addressed, and the primary treatment approach used with trauma patients. They were also asked to rate how they perceive that working with trauma patients has impacted upon them personally.
Victimization history
This self-report measure assesses whether the respondent has experienced a traumatic event in the past (directly experienced or observed), when and the number of times it was experienced, and the level of distress experienced at the time, as well as the level of distress currently caused by the event. Respondents indicated their distress using a 5 point Likert-type scale ranging from 1 = no distress to 5 = extreme distress. Only those experiences that were rated as ≥3 at the time were included in the analyses. This was to avoid including experiences that the participant endorsed as stressful, but which was could not be described as traumatic. This inventory is an adaptation of the trauma screen that forms part of the Post-traumatic Stress Scale [29], and was developed for the purpose of this study.
Affective distress
The Depression, Anxiety and Stress Scales (DASS-21) is a 21-item self-report instrument designed to measure the three related negative emotional states of depression, anxiety and tension/stress [30]. The DASS-21 is the short form of the 42-item DASS [30], and each of the three DASS scales contains seven items, with each item representing a negative emotional state. Subjects are asked to use 4 point combined severity/frequency Likert-type scales to rate the extent to which they have experienced each negative emotional state over the past week, ranging from 0 = did not apply to me at all to 3 = applied to me very much or most of the time. Acceptable levels of reliability and validity have been reported, for this commonly used measure [31].
Burnout
The Copenhagen Burnout Inventory (CBI) is a 19-item self-report inventory measuring three types of burnout: personal, work and patient burnout [32]. According to Borritz and Kristensen, personal burnout is defined as ‘a state of prolonged physical and psychological exhaustion’ [33]. Work burnout is ‘a state of prolonged physical and psychological exhaustion, which is perceived as related to the person's work’. Patient burnout is ‘a state of prolonged physical and psychological exhaustion, which is perceived as related to the person's work with clients’. The questions are answered on a 5 point Likert-type scale, and separate scores are obtained for each of the three scales. Borritz and Kristensen reported the CBI to have high internal consistency for the personal, work and patient burnout scales, respectively (0.86, 0.87 and 0.85) [33].
Secondary traumatic stress
The Secondary Traumatic Stress Scale (STSS) consists of 17 5 point Likert-type scale items, designed to measure the frequency of intrusion, avoidance, and arousal symptoms associated with indirect exposure to traumatic events via one's professional relationships with traumatized patients, over the past 7 days [34]. The STSS measures the symptoms outlined in the DSM-IV criteria B (intrusion), C (avoidance) and D (arousal) for PTSD [18]. The STSS, unlike other measures of traumatic stress symptoms, refers specifically to ‘work with clients’ as the traumatic stressor. This self-report measure has shown good reliability, with Cronbach's alpha of 0.93 for the total score [34].
Vicarious trauma
The TSI Belief Scale–Revision L (TSI-BSL) measures the disruptions in beliefs about self and others that arise from psychological trauma or from vicarious exposure to trauma material through psychotherapy or other helping relationships [9, 35]. The full version of the TSI-BSL consists of 80 items, and yields an overall score and 10 scale scores. The five scales that were used in the present study, due to design constraints, included Self-Safety (the need to feel that one is reasonably invulnerable to harm inflicted by self or others), Other Safety (the need to feel that valued others are reasonably protected from harm inflicted by oneself or others), Other Esteem (the belief that others are valuable and worthy of respect), Other Trust (the belief that one can rely upon others) and Other Intimacy (the belief that time spent with others is enjoyable). The selected scales were chosen based on their perceived relative significance to clinicians working with traumatized people. The selected scales have been suggested to be more sensitive to the cognitive effects of therapeutic work with traumatized people on the therapist than the other scales [26, 36]. Schauben and Frazier found that reliability coefficients for the five subscales selected for use in this study were within the range r = 0.68–0.84 [11].
Empathy
The Interpersonal Reactivity Index (IRI) is a 28-item self-report measure of general empathy [37]. Responses are made on a 5 point Likert-type scale, with higher scores indicating greater empathy. The measure has four subscales, and according to Davis the Perspective Taking scale measures the ‘tendency to spontaneously adopt the psychological point of view of others’, the Fantasy scale measures respondents ‘tendencies to transpose themselves imaginatively into the feelings and actions of others’, the Empathic Concern scale measures ‘other-oriented feelings of sympathy and concern for unfortunate others’, and the Personal Distress scale measures ‘self-oriented feelings of personal anxiety and unease in tense interpersonal settings’ [37]. Internal consistencies of the four scales of empathy have been found to be satisfactory, within the range 0.71–0.77 [37], with test–re-test reliabilities ranging from 0.62 to 0.71.
Perceived social supports
The 12-item Interpersonal Support Evaluation List (ISEL-12) measures the perceived availability of potential social resources [38]. It has three scales that can be summed to produce a total score: tangible, appraisal, and belonging support. Responses to a list of statements are made on a 4 point scale, ranging from 1 = definitely false to 4 = definitely true. Higher scores indicate greater perceived social support, and internal reliability for the scales has been found to be within the range 0.88–0.90 [38].
Procedure
Those participants who were contacted directly were sent the plain language statement, which outlined the purpose of the study, requirements of participants and details regarding confidentiality and grievance procedures. It was specified that ‘the purpose of this project is to explore how therapeutic work might have emotional repercussions on the therapist, using a sample of Australian mental health professionals’. The plain language statement referred participants to the website where the questionnaire battery was posted, and offered contact details to request a paper version of the questionnaire battery, if preferred.
All participants were given the standardized questionnaire battery, and either completed and submitted it online (n = 53), or completed a paper version that was then returned in the post to the researchers (n = 99).
Results
We utilized the following software: SPSS (SPSS, Chicago, IL, USA), Statistica, version 6.1 (StatSoft, Tulsa, OK, USA) and ClinTools version 4.1 [28].
Data cleaning and randomization
Where cases were missing a significant number of values on any one scale (>3), the case was deleted. In this way, four cases were deleted. The following transformations were applied to variables prior to analyses in order to meet the assumptions of normality (ungrouped data): square root transformations: TSI-BSL total score, each of the five TSI-BS subscale scores, Burnout total score, ISEL-12 total score, trauma patient caseload, caseload (average), duration of career as a mental health professional, duration of career treating trauma patients, hours worked per week with trauma patients; log10 transformation: DASS-21 total score (affective distress), history of personal trauma (number of experiences); and inverse transformation: STSS total score. For the remaining variables analytical assumptions were met, and the data were parametrically distributed with approximate homogeneity of variance.
To determine whether any differences within the sample had an impact on the measures of interest, between-subjects multivariate analyses of variance were conducted. The dependent variables STS, VT, burnout and affective distress were not found to be significantly influenced by (i) professional affiliation: psychologists (n = 124) versus Other (n = 26; F(4,145) = 0.75, NS; (ii) theoretical orientation (F(4,102) = 0.58, NS); or (iii) the patient group with which the therapist predominantly worked (F(4,144) = 1.95, NS). Nor were any of the dependent variables found to be significantly different between any of the groups. Subsequently it was considered valid to use a sample with mixed disciplines, theoretical orientations and patient groups.
Participants were asked to respond to a number of demographic items, the results of which are presented in Table 1.
Subject characteristics (n = 152)
MHP, mental health professional.
The internal reliability of each of the measures used in the study, using the present sample, was calculated using Cronbach's alpha. The coefficients were found to be as follows: DASS-21, Cronbach's α = 0.91; STSS, Cronbach's α = 0.90; CBI, Cronbach's α = 0.93; TSI-BSL, Cronbach's α = 0.92; ISEL-12, Cronbach's α = 0.86; and IRI, Cronbach's α = 0.71.
Are STS and VT are more convergent with each other and affective distress than is acceptable for discriminant validity?
To test hypothesis 1 Pearson correlation analyses using the entire data sample (n = 150) assessed the degree to which STS, VT and affective distress were associated with one another. STS and VT were found to correlate moderately highly (r = 0.49, p < 0.01), indicating strong convergence between the constructs. STS was found to be associated with affective distress, correlating very highly (r = 0.61, p < 0.01) and indicating very strong convergence between the constructs. Similarly, VT was found to correlate highly (r = 0.51, p < 0.01) with affective distress, indicating strong convergence between the constructs.
Are STS and VT sufficiently discriminated from burnout?
In order to test hypothesis 2 Pearson correlation analyses (n = 150) were applied to assess the degree to which STS and VT were associated with burnout. STS was found to correlate very highly (r = 0.62, p < 0.01), which is unexpected considering the theoretical differences between the two constructs. Furthermore, the correlation between STS and trauma patient caseload was small (r = 0.19, p < 0.05). VT was also found to correlate highly with burnout (r = 0.51, p < 0.01), which is unexpected considering the theoretical differences between the two constructs. The correlation between VT and trauma patient caseload was small (r = 0.24, p < 0.01). Both STS and VT correlate more strongly with burnout than they do with each other, indicating that the constructs tap into more than trauma-related psychopathology.
When the predictors for burnout and VT are used in a regression model for STS, will the model fit the data as well or better as when the theoretical predictors of STS alone are used?
To test hypothesis 3 a multiple regression analysis was conducted (n = 144). The independent variables or predictors included in the analyses were those predictors for burnout, and the theoretical predictor of VT, which is not also a theoretical predictor of STS. Specific predictors included the following: burnout: ‘work stress’ (lack of support, role conflict, unreasonable workload, and unclear employer expectations), ‘satisfaction with work as a mental health professional’, ‘duration of career as a mental health professional’, ‘number of clients seen each week’, ‘hours worked each week as a mental health professional’, ‘perceived interpersonal support’; and VT: ‘time spent working therapeutically with traumatized people’. The predictors were entered using the ‘enter’ method. The ratio of cases to independent variables was considered to be sufficient, using n ≥ 104 + 9 (predictors) [39]. This model predicted 19% of the variance observed in STS scores, with an adjusted R2 of 0.19 (r = 0.48, F(6,138) = 6.76, p < 0.001), indicating that this model of STS is a better fit for the data than the theoretical model proposed by Figley [17], which predicted only 1.7% of variance. The strongest individual predictors of STS were ‘perceived interpersonal support’ (β = − 0.23, p < 0.01), ‘caseload’ (β = 0.24, p < 0.01), and ‘satisfaction with work as a mental health professional’ (β = − 0.24, p < 0.05); all predictors of burnout. See Table 2 for correlations between the variables, and Table 3 for the unstandardized regression coefficients and intercept, the standardized regression coefficients, and the semi-partial correlations for the independent variables.
Multiple regression analysis for variables (predictors of VT and burnout) predicting STS among therapists (n = 144)
DV, dependent variable; MHP, mental health professional; STS, secondary traumatic stress; VT, vicarious trauma.
For variables that were transformed using inverse to meet the assumption of normality, the direction of the correlation coefficient has been corrected.
Means and standard deviations presented are for transformed variables.
∗p < 0.05, two tailed; ∗∗p < 0.01, two-tailed.
Multiple regression analysis for variables (predictors of STS and burnout) predicting VT among therapists (n = 144)
DV, dependent variable; MHP, mental health professional; STS, secondary traumatic stress; VT, vicarious trauma.
For variables that were transformed using inverse to meet the assumption of normality, the direction of the correlation coefficient has been corrected.
Means and standard deviations presented are for transformed variables.
∗p < 0.05, two tailed; ∗∗p < 0.01, two-tailed.
When the predictors for burnout and STS are used in a regression model for VT, will the model fit the data as well or better as when the theoretical predictors of VT alone are used?
First, it should be noted that the predictors of STS include all of those that predict VT, so only burnout predictors will be used in this model.
In order to test hypothesis 4 a multiple regression analysis was conducted (n = 144), and the independent variables or predictors included in the analyses were those predictors for burnout: ‘work stress’ (lack of support, role conflict, unreasonable workload, and unclear employer expectations), ‘satisfaction with work as a mental health professional’, ‘duration of career as a mental health professional’, the ‘number of clients seen each week’, ‘hours worked each week as a mental health professional’, and ‘perceived interpersonal support’. The predictors were entered using the ‘enter’ method.
This model predicted 39% of the variance observed in VT scores, with an adjusted R2 of 0.39 (r = 0.64, F(5,139) = 19.02, p < 0.001), indicating that this model of VT is a much better fit for the data than the theoretical model, which predicted only 4.9% of variance. The strongest individual predictors of VT were ‘perceived interpersonal support’ (β = − 0.43, p < 0.001) and ‘work stress’ (β = 0.25, p < 0.01). Unexpectedly, the model for burnout predicts VT better than it does for burnout in this sample (Table 3).
Does STS and VT differ based upon therapist exposure to trauma patients?
To test hypothesis 5 a one-way between-subjects multivariate analysis of covariance was conducted, with STSS total score and TSI total score as dependent variables; and the upper and lower quartiles of trauma patient caseload as the independent variable. These two groups represent participants with low (n = 34, mean = 5.8% of caseload) and high (n = 44, mean = 89.6% of caseload) exposure to trauma cases. Total sample size (n = 79) was reduced to 78 due to a missing score on one of the covariates. The covariates in this analysis were ‘hours worked each week’ and ‘work stress’, to determine whether removing the variance attributed to these variables would influence the results. ‘History of personal trauma’ was also used as a covariate due to there being a significant difference between the two groups on this measure. Removing the variance attributed to this variable enabled a clearer comparison of the two groups on STS and VT.
Hotellings’ trace was used to determine the significance of the main effect of group. A series of independent samples t-tests found that the two groups (high and low exposure to trauma cases through therapeutic work) differed significantly on the number of directly experienced traumatic events endorsed, with participants high in exposure to trauma cases reporting a greater ‘history of personal trauma’ (t(77)= − 3.12, p < 0.01). The groups also differed significantly on ‘work stress’ with participants low in exposure to trauma cases reporting more ‘work stress’ (t(77)= − 2.31, p < 0.05). Due to there being a significant difference between the groups on these measures, they were selected as covariates and used as outlined in an earlier section. Correlations between these variables and the outcome variables of STS and VT were examined for both the total sample and each group separately, to determine whether by using the covariates the main effect would be removed from the analysis. A history of primary trauma did not relate to outcome (correlations low), and ‘work stress’ correlated inconsistently with STS (high in group 1 and low in group 2). Considering that ‘work stress’ is theoretically distinct from both STS and VT, and it had an influence on outcome, it was retained as a covariate.
With the use of Hotellings trace, the combined dependent variables were found to not be significantly influenced by exposure to trauma cases (F(2,72) = 2.26, NS) when the variance attributed to the variables of ‘hours worked each week as a mental health professional’, ‘work stress’ and ‘history of personal exposure to trauma’ were covaried from the analysis. Neither VT (F(1,73) = 3.41, NS), nor STS (F(1,73) = 2.21, NS) were identified as being significantly different between the two groups. Considering the very high correlations between STS and VT with work stress (Table 4), despite being theoretically distinct, it appears that STS and VT tap into this non-trauma-related phenomena. An ANOVA using work stress as the dependent variable (n = 78) found that the groups differed significantly (F(1,78) = 5.28, p = 0.02), with work stress greater among therapists with fewer trauma patients on their caseload (mean = 15.22, SD = 3.25) than those with a higher number of trauma patients (mean = 13.55, SD = 3.09). This represented a moderate effect size (Hedges’ g = 0.52). The two groups did not differ significantly when burnout was used as the dependent variable (F(1,78) = 0.74, NS).
Intercorrelations between main variables (n = 150)
STS, secondary traumatic stress; VT, vicarious trauma.
For variables that were inversely transformed to meet the assumption of normality, the direction of the correlation coefficient has been corrected.
∗p < 0.01, two-tailed.
Respective contribution of VT and burnout to affective distress
To test hypothesis 6 two hierarchical regression analyses were conducted (n = 150). The independent variables included in the analysis were burnout and VT. STS was not used in the analysis due to the very high correlation between the STS and burnout (r = 0.61) and the similarity in questions between the STS and the DASS-21 (the measure used for affective distress). In the first analysis burnout was entered in the first step and VT in the second; and vice versa in the second analysis. The predictors were entered using the ‘enter’ method. In addition to the screening of data as discussed, the ratio of cases to independent variables was considered to be sufficient, using n ≥ 104 + 2 predictors [39].
The two independent variables predicted 37% of the variance observed in affective distress scores, with an adjusted R2 of 0.37 (r = 0.62, F(1,147) = 45.56, p < 0.001). Both predictors were found to contribute significantly to affective distress irrespective of which was entered into the model first, which is unsurprising considering the high degree of shared variance between them. Burnout, however, contributed an R2=0.31 when entered first, and an R2 change = 0.12 when entered second; whereas VT contributed an R2=0.26 when entered first and an R2=0.07 when entered second (Table 5).
Hierarchical regression analyses for burnout and VT predicting affective distress among therapists (n = 150)
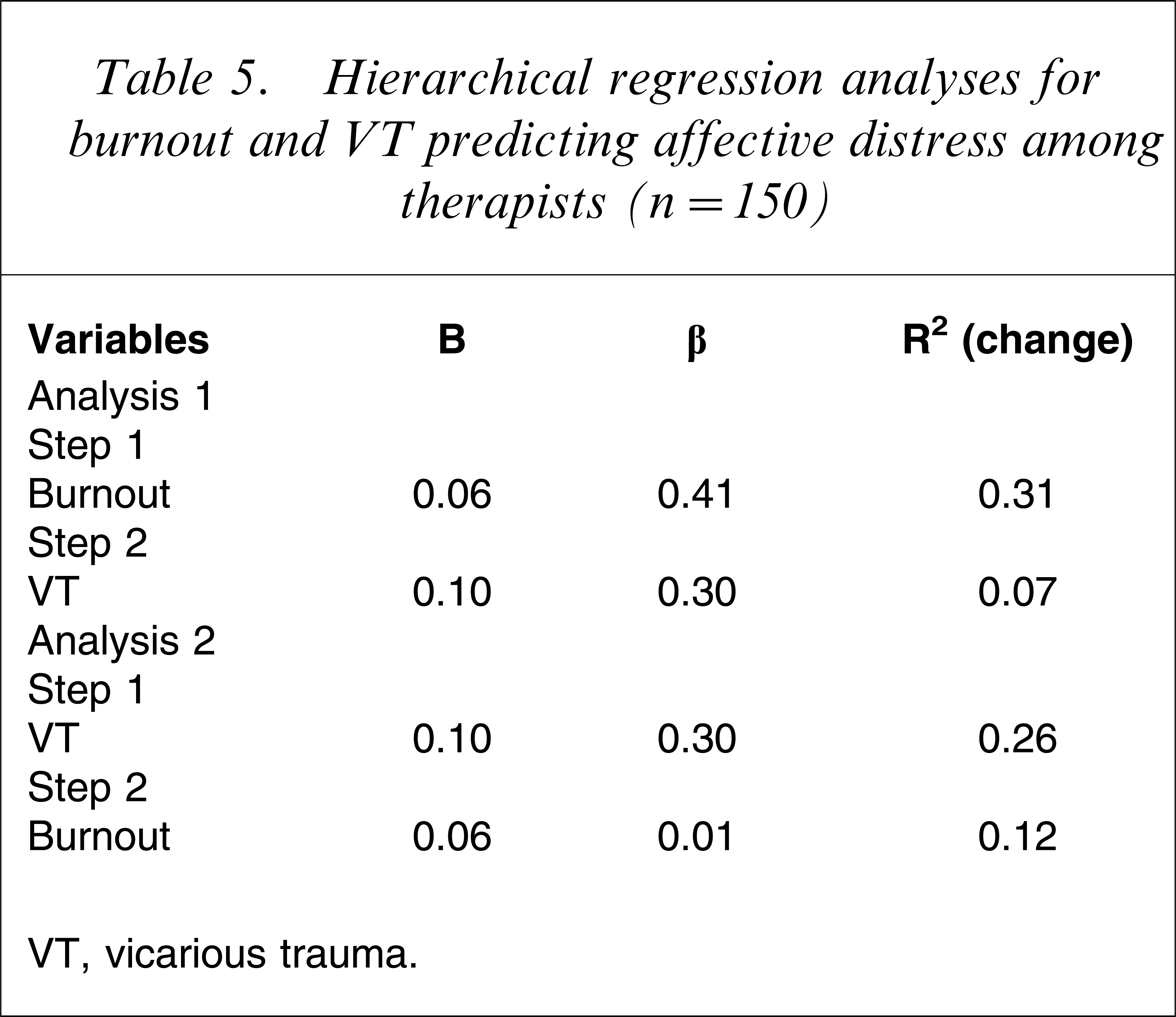
VT, vicarious trauma.
Domains of VT to predict affective distress
In order to test hypothesis 7 a multiple regression analysis was conducted with affective distress as the dependent variable. The independent variables included in the analyses were burnout, the individual subscales for VT, as well as the predictors for burnout: ‘work stress’ (lack of support, role conflict, unreasonable workload, and unclear employer expectations), ‘satisfaction with work as a mental health professional’, ‘duration of career as a mental health professional’, ‘number of clients seen each week’, ‘hours worked each week as a mental health professional’, ‘perceived interpersonal support’; and all trauma-related variables including: ‘trauma client caseload’, ‘duration of career as a trauma therapist’, ‘history of personal trauma’ and ‘hours of trauma work each week’. The predictors were entered using the ‘forward’ method, with F ≤ 0.05 to enter. In addition to the screening of data as discussed, the ratio of cases to independent variables was considered to be sufficient, using N ≥ 104 + 9 [39].
The significant predictors for affective distress were burnout (β = 0.36, p < 0.001), ‘duration of career as a mental health professional’ (β = − 0.25, p < 0.001), ‘beliefs about self-safety’ (VT; β = 0.24, p < 0.01), and ‘beliefs about other-intimacy’ (VT; β = 0.18, p < 0.05). This model predicted 44% of the variance observed in affective distress, with an adjusted R2 of 0.44 (r = 0.68, F(4,133) = 28.32, p < 0.001).
A regression analysis for affective distress was run using the most significant predictors of burnout: duration of career as a mental health professional, and beliefs about self-safety. The predictors were entered using the ‘enter’ method (n = 146). This model also predicted 44% of the variance observed in affective distress scores, with an adjusted R2 of 0.44 (r = 0.67, F(3, 143) = 39.64, p < 0.001). The results suggest that this model of affective distress is a better fit than the model using burnout (total score) and VT (total score), which predicted 37%. It also suggests that there is one subscale of VT, beliefs about self-safety, which contributes more to affective distress than all of the subscales combined.
Discussion
The aim of the present study was to investigate the relationship between trauma work and the constructs of STS, VT, and burnout among mental health professionals in community-based and private clinical practice. More specifically, the aims were to determine the validity of each construct, the degree to which they overlap, and how each contributes to the prediction of affective distress among this sample of therapists. The research found that STS, VT and burnout are highly convergent constructs, but the measures for STS and VT do not display construct validity whereas burnout does. It was found that work-related stressors (such as burnout and being new to the profession) best predicted therapist distress. The finding that beliefs about one's safety (a component of VT) also contribute to therapist distress was significant, because to date research has focused on the trauma-related and organizational factors contributing to therapist distress. It is also noteworthy that the average levels of STS, VT and burnout within this sample of therapists were relatively low.
It was found that the three constructs of STS, VT and burnout mainly appear to measure the same phenomenon, and both STS and VT are better predicted by the model for burnout than their own theoretical models. It was apparent that the three constructs are predominantly measuring the same phenomenon, burnout, and that exposure to patients’ traumatic material had no significant impact on STS, VT or burnout. This finding contradicts the theory and research of Figley [17] and Pearlman and Saakvitne [8], the originators of these constructs. This finding supports recent research by Van Minnen and Keijsers [26], who also found that the impact of working therapeutically with traumatized patients appears to be overestimated. It was found that work-related stressors (such as burnout and being new to the profession) best predicted therapist distress. The finding that beliefs about one's safety (a component of VT) also contribute to therapist distress was significant, because to date research has focused on the trauma-related and organizational factors contributing to therapist distress. It is also noteworthy that the average levels of STS, VT and burnout within this sample of therapists were relatively low.
As predicted, it was found that there was no significant difference in VT or STS for those with high exposure to trauma patients compared to those with low exposure to trauma patients. Similarly there was no significant difference between the two groups for burnout. Exposure to trauma cases appears to have little impact on the development of STS, VT or burnout among therapists. These findings run counter to a significant body of research that has found that working therapeutically with trauma patients has deleterious effects on therapists [10, 11, 24, 40]. Irrespective of other concerns regarding the research design utilized in these other studies, the primary concern is their failure to incorporate a control group of non-trauma therapists in their samples. In doing this they have tacitly accepted that STS and VT are phenomena observed only in those working with traumatized people. This research, along with that of Van Minnen and Keijsers [26] and Raquepaw and Miller [6], suggests that this assumption may be false and that STS and VT are not measuring phenomena that are necessarily trauma related.
It was found that both VT and burnout contributed significantly to the prediction of affective distress. Combined, they predicted 37% of the variance observed in affective distress scores. Both predictors were found to contribute significantly to affective distress irrespective of which was entered into the model first. This was somewhat surprising, considering the high degree of shared variance between the two constructs, and supports the earlier finding that each is measuring something independent of the other. Burnout, however, explains more variance in affective distress than does VT, although VT contributes something beyond burnout, supporting the findings of McLean et al. [13].
The significant predictors for affective distress were burnout, ‘duration of career as a mental health professional’, ‘beliefs about safety of the self’ (VT), and ‘beliefs about intimacy with others’ (VT). This model predicted 44% of the variance observed in affective distress. This was a considerably better model than that incorporating burnout and VT alone (not separated into subscales), which predicted 37% of variance in affective distress. A regression analysis for affective distress was then run using the most significant predictors: burnout, ‘duration of career as a mental health professional’, and ‘beliefs about self-safety’. The VT subscale ‘beliefs about intimacy with others’ was eliminated from this analysis because it was a less powerful predictor of affective distress than the other variables. This more parsimonious model also predicted 44% of the variance observed in affective distress scores, indicating that one subscale of VT, ‘beliefs about safety of the self’, contributes more to affective distress than all of the other VT subscales combined.
The findings indicate that burnout, with its basis in work-related stressors, is the strongest predictor of therapist distress. Despite the degree of concern among ‘traumatologists’ and trauma support organizations around the world with respect to the proposed deleterious effects on therapists of working with trauma patients, the findings of this research suggest that such claims are overestimated, supporting the findings of Van Minnen and Keijsers [26], Jenkins and Baird [41], and Kadambi [12]. In light of this, we suggest that the approach of singling out trauma therapists for special treatment runs the risk of iatrogenic effects and may also be perceived by non-trauma therapists as minimizing the personal involvement and commitment they have to their work.
It was also found that being new to the profession, and beliefs regarding one's safety and intimacy with others predicted affective distress. This finding supports the Cotton and Hart position in their review of organizational health research, that workplace experiences such as support and satisfaction with the job are better predictors of distress in those engaged in people work, than ‘operational’ experiences such as exposure to traumatic material [42]. The findings also support Pearlman and MacIan's research, which found that new therapists are more likely to experience affective distress [10]. This is likely due to having less experience, and a lower sense of self-efficacy than a more experienced therapist. The finding that beliefs regarding one's safety also contributed significantly to the model of affective distress adds weight to the McClean et al. finding that unhelpful beliefs about therapy were more predictive of burnout and VT than situational variables such as work stress [13]. With this knowledge (that the best predictors of affective distress are burnout and being new to the profession), efforts to reduce stress among therapists can be focused on further exploring and refining our understanding of burnout and its measurement within this population.
In respect to therapists’ ‘history of personal trauma’ it was found that those who reported high exposure to trauma cases reported a greater ‘history of personal trauma’. This suggests that people who have been exposed to primary trauma themselves tend to see more traumatized patients or are more likely to conceptualize their patients’ experiences as ‘traumatic’. This finding is in contrast to research by Schauben and Frazier [11], but was consistent with the findings of Pearlman & MacIan [10] and Follette et al. [14]. Those who reported more ‘work stress’ were more likely to be low in exposure to trauma cases, which may indicate that people who see more traumatized patients either work in more supportive environments, are better able to tolerate work stress or are not deleteriously affected by the need to research and treat a plethora of presentations because they specialize in only one field. It may also indicate that the less experienced therapists, who are more likely to experience burnout through work stress, also work with fewer trauma patients. Finally, exposure to trauma patients appears to have little impact on the development of STS or VT among therapists. This directly supports the findings of Van Minnen and Keijsers [26], but provides a larger sample and more targeted measures.
The representativeness of the sample was limited by the fact that although therapists were randomly selected from publicly available databases, there was no way to control for the propensity of some therapists to decide to participate and others to decide otherwise. It was assumed that some therapists would respond because they have a special interest in the topic, or possibly believe themselves to suffer from STS, whereas others may, for the same reasons, have decided not to participate. This potential bias in responding would suggest that the data might not be representative of all therapists engaged in clinical practice in Australia. Without forcing therapists to take part, however, this problem is unavoidable and we believe that we have a random sample that is as representative of the true population as ethically possible. The fact that the response rate for the study was relatively low at 32% needs to be considered with respect to the representativeness of the findings, yet is consistent with other research into this topic. The majority of participants in the research were women, which is indicative of the gender bias within the mental health profession (male: female = 45:107), and 74% of the sample were aged >38 years. It is likely that these older participants have worked within the field for longer, and have managed to cope with the stressors of therapeutic work, whereas newer professionals might have dropped out of the work due to stress, burnout or lack of job fit. Another important aspect is the ability of therapists to maintain clinical and personal boundaries, and obtain and utilize appropriate professional supports. It may well be that individuals who fail such a prerequisite are more affected by the struggles faced by their patients (all patients) and leave the profession earlier. More research in clinical practice elements and supervision is required to satisfactorily explain how much of the variance in therapist affect is due to these elements.
This research has identified that workplace burnout, being new to the profession, and shifts in beliefs about one's safety, lead to distress among therapists. It would be useful for future research to utilize longitudinal research designs and identify what predicts affective distress among therapists, and what factors are protective. This research suggests that both workplace and individual factors contribute to the development of affective distress among therapists and although workplace factors have been well researched, primarily through the burnout literature, individual vulnerability factors remain relatively unexplored. Ultimately, the findings support recent research and theory around individual resilience, which has indicated that the impact of working with traumatized patients is overestimated [26, 43].