
Abstract
One of the most relevant psychopathological debates of the last decades has been centred on the relationships between melancholic (or endogenous) and non-melancholic depression. Is melancholia only a severe variant of major depression [1], or is it qualitatively distinct from the ordinary form of depression [2]? A long series of studies led Parker and Hadzi-Pavlovic to define melancholia exclusively on psychomotor disturbances (assessed by an observational scale named CORE) [3, 4], and to propose a modified dualist hypothesis, ‘with there being one entity (i.e., melancholia or endogenous depression) but with the remaining depressive disorders being a heterogeneous residue rather than a true entity or distinct class’[5]. Subsequently, Parker et al. developed a self-rating personality instrument, the Temperament and Personality Questionnaire (T&P) to explore the temperament and personality dimensions of the different types of depression [6]. One of the major tenets of dualist theories is that non-melancholic depressions arise in more personality disordered individuals, compared to melancholia [5, 7, 8], although in a latent classes analysis only 59 out of 185 non-melancholic depressed patients were judged as personality disordered [9]. The main aim of the present investigation was to assess personality with the T&P to verify whether the correspondence of personality disorders with non-melancholic depression, and of better psychosocial functioning with melancholia was confirmed by both CORE and DSM-IV melancholia. We wished also to compare CORE with two other well-known criteria sets, that is, Research Diagnostic Criteria (RDC) [10] for Retarded and Agitated Depression. Higher scores on the eight personality scales of the T&P (especially on Social Avoidance [5]) were taken as indication of disordered personality, while higher scores on the two global functioning scales (Effectiveness and Cooperativeness) were considered as indicative of better personality functioning.
Methods
Sample
The sample consisted of 188 consecutive inpatients of a metropolitan university psychiatric department. Their mean age was 51.9 years (SD=14.8 years, range=18–80 years), and 73.4% were female. The CORE group (n=62) had a mean age of 53.3 years (SD=13.6), which was not significantly different from the non-CORE group (n=126) with its mean age of 51.3 years (SD=15.4). The CORE group consisted of significantly fewer women (61.3%) compared to the non-CORE group (79.4%). Inclusion rules were: DSM-IV diagnosis of major depressive disorder (confirmed on structured interview [11]), MMSE >23, and absence of psychotic symptoms. Patients were enrolled only if they were at the nadir of their episode, according to the CORE system (63 unipolar depression patients were not included for this reason).
Assessment of melancholic subtypes
All patients were rated during the second or third day of hospitalization by two trained independent judges, strictly following the guidelines of the CORE system [3] (intraclass correlation coefficient (ICC)=0.87), and the classification criteria of DSM-IV Melancholia (ICC=0.86), RDC Retarded Depression (ICC=0.90), and RDC Agitated Depression (ICC=0.88). ICCs were calculated on presence/absence of each diagnosis. Cases of disagreement were settled by discussion.
Measures of personality disorder and disordered functioning
The T&P [6] was administered as part of the global psychometric routine, and only after the patient's symptomatology was stabilized. It is a 109-item self-report instrument, with a yes/no response format. The following eight personality scales are derived: Anxious–Worrying, Irritability, Perfectionism, Self-Criticism, Social Avoidance, Personal Reserve, Rejection Sensitivity, and Self-Focus. Two measures of global functioning are also provided by the T&P, one on Cooperativeness and one on Effectiveness.
Statistical analysis
Inter-group comparisons were performed with one-way ANOVAs, controlling for age and sex.
Results
As hypothesized, CORE patients scored significantly lower on Social Avoidance and significantly higher on the two measures of functioning, that is, cooperativeness and effectiveness (Table 1); unexpectedly, they displayed a significant and marked higher mean score of Perfectionism.
CORE and non-CORE melancholia on T&P subscales (univariate tests controlling for sex and age)
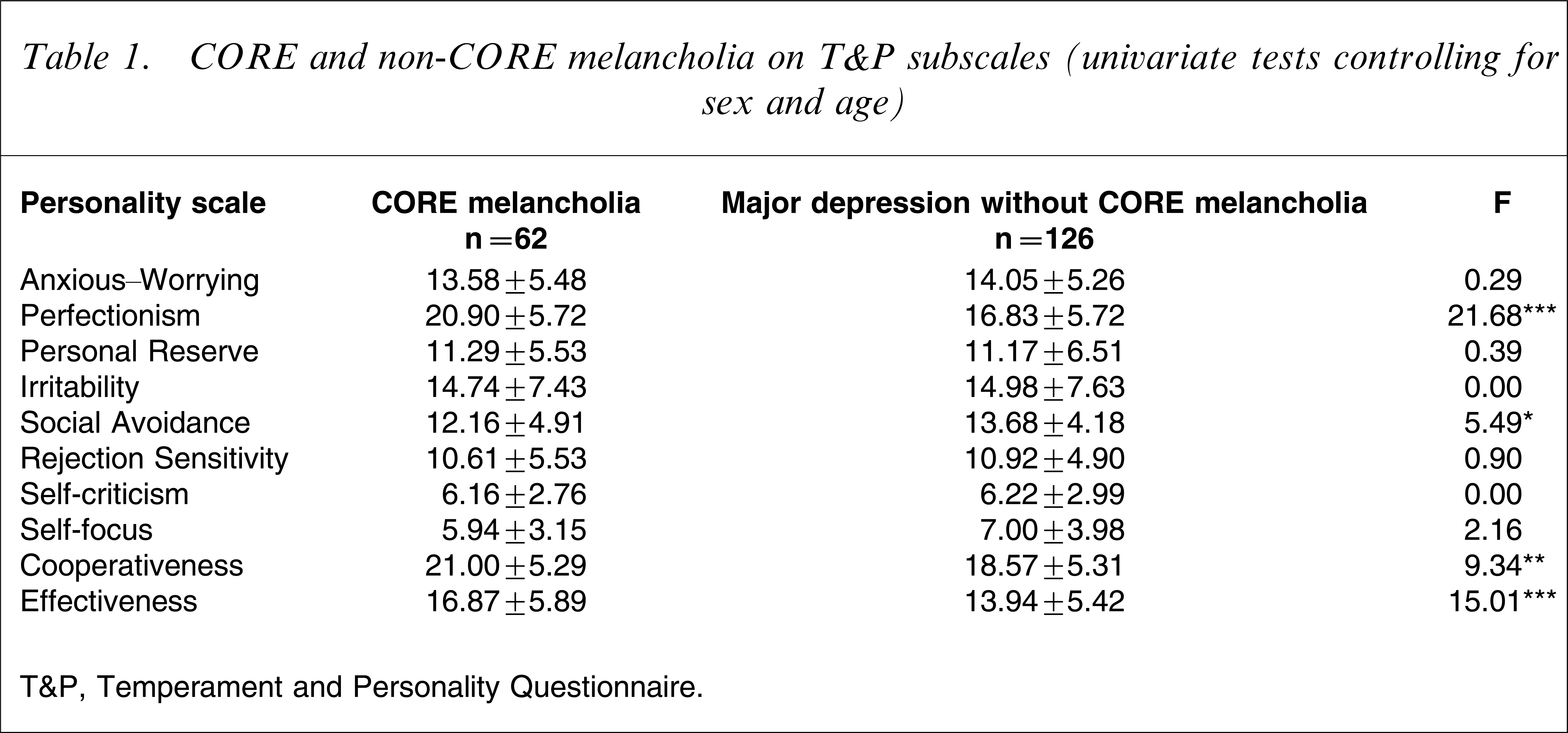
T&P, Temperament and Personality Questionnaire.
In contrast, patients with DSM-IV Melancholia scored significantly higher on Irritability and significantly lower on Cooperativeness, thus totally countering the hypotheses (Table 2). As regards RDC Retarded Depression, endogenous patients scored significantly lower on Anxious–Worrying but also (against the hypotheses]) on Cooperativeness. The RDC criteria set for Agitated Depression yielded findings that were in fair agreement with predictions: endogenous patients had significantly lower mean scores of Anxious–Worrying, Social Avoidance, and Rejection Sensitivity, and significantly higher mean scores of Effectiveness. It is to be noted that, like the CORE system, the RDC criteria set for Agitated Depression also produced markedly higher mean scores of Perfectionism in the endogenous group.
Endogenous/melancholic and non-endogenous/non-melancholic depressed inpatients on T&P scales (Fs, controlling for sex and age), measured using non-CORE system
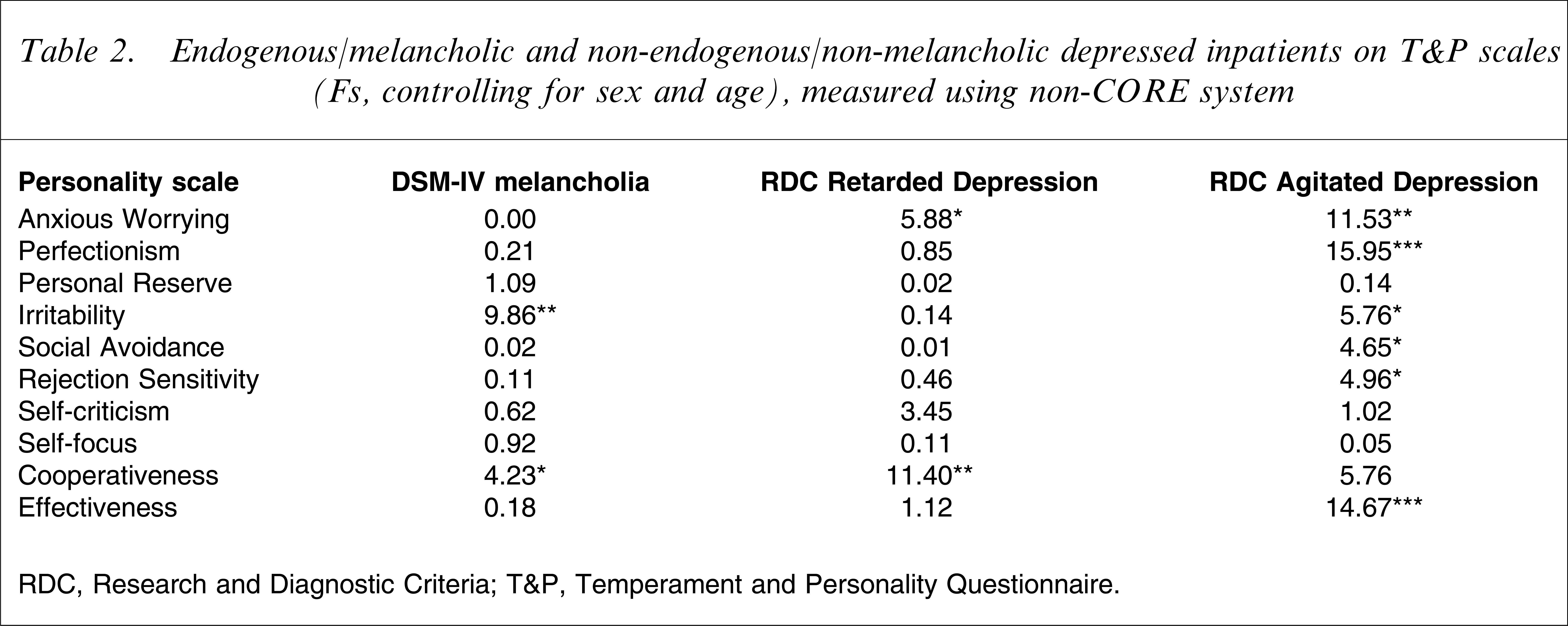
RDC, Research and Diagnostic Criteria; T&P, Temperament and Personality Questionnaire.
Discussion
The hypothesis of less personality dysfunction in melancholic/endogenous depression, compared to the other types of depression was partially supported by present findings. CORE melancholia, RDC Agitated Depression, and, less clearly, RDC Retarded Depression confirmed the assumption, while DSM-IV melancholia did not, thus suggesting that DSM-IV criteria for melancholia may not be adequate [12]. Among the T&P scales, however, only Social Avoidance was significantly linked to non-CORE depression, instead of a larger spectrum of personality traits, as could have been expected, and this does not allow a full confirmation of the hypotheses.
We did not predict a significant elevation of scores of Perfectionism in CORE melancholia or in RDC Agitated Depression; but this finding is reminiscent of the personality features outlined in the past for Tellenbach's typus melancholicus [13], that is, orderliness, seriousness, reliability and so on, and suggests that the personality background of melancholia is more specific than the barely negative notion of a lack of personality dysfunction. Because statistical comparisons were controlled for age, it seems unlikely that the higher evidence of perfectionism among endogenous patients could be due to age-related characteristic (such as vascular brain alterations). Further studies should compare the Parker and Tellenbach models of personality in melanchonia.
The major limitation of the present study was that personality dysfunction was measured only by a self-report instrument and not also by a structured interview. Furthermore, the T&P does not include a scale for hysterical, immature, reactive traits, which were the ones most significantly associated with non-melancholic depression in some of the previous studies [14]. In contrast, the T&P is explicitly aimed at differentiating between different types of depression.
Present findings are congruent with both the dualist hypothesis [2] and the modified dualist perspective [5] because it is not easy for the unitary-dimensional model to explain why a better personality functioning should correspond to severe psychomotor disturbances, such as those assessed by the CORE and the RDC.