
Abstract

Psychopathology in twins: ancient case study
‘The Jealous Twins’ is an Australian Aboriginal story [1]. The Australian Aboriginal culture is the oldest continuous culture on earth, the first members arriving approximately 40–50 000 years ago. At the current time there is no way of knowing precisely the age of this story, which is likely to be 5000 years old.
The aim of this paper is to examine this story using current concepts of mental disorder. Should this examination provide evidence of psychopathology, ‘The Jealous Twins’ would antedate other accounts of psychopathology by millennia.
The first description of major depression is believed to be the story of Job, who lived in the fourth century
Twin studies are important in the study of psychotic disorders because they indicate a genetic contribution. Within twin pairs, differences in clinical presentation are compatible with the continuum model of psychotic illness [3].
A summary of the relevant parts of the story is presented. This is followed by an attempt to identify the psychopathology, and a discussion.
Perindi and Harrimiah were twins. They had a very close relationship. They played together as children, were initiated together and hunted together as adults. Each had great warmth for, and respect for the abilities of, the other. They were attractive and skilled and much admired by the other members of the tribe, although the elders expressed concern that they were so comfortable in their relationship that they had not yet felt the need to take wives.
The first incident of interest began the day before planned tribal contests. A young woman told Perindi that she admired his physique, appearance, hunting ability and wisdom. She went on to say that Harrimiah had been boasting that he was better looking, more skilful and braver than his twin.
Initially, Perindi could not believe that Harrimiah would say such things. Overnight, however, he came to believe what he had been told and decided to teach his twin a lesson.
On the day of the contests they painted each other's body. When Perindi painted Harrimiah's body, he did a very poor job. Harrimiah was unaware of his less than splendid appearance.
When the twins approached the main encampment they were greeted by the young women, but most of them surrounded Perindi. Harrimiah was puzzled, as they usually attracted equal attention.
He sat down on the edge of a pool wondering why he had been largely ignored by the young women. When he bent down to drink he saw in his reflection, his less than splendid appearance and the reason he had attracted little attention. He aside asked his twin why he had painted him so poorly.
Perindi stated that there was nothing wrong with his painting. He said that he had probably attracted more attention because he had a better body than Harrimiah. He went on to say that he was a better dancer, and that this would shortly be revealed. As it happened, there was little to separate the two in the first dance, although both danced better than the other young men.
The following day they performed the frog dance. When this dance ended the young women flocked to Harrimiah and loudly praised his skill and energy. ‘Something seemed to break inside’ Perindi. He was suddenly very angry. He shouted at his twin that he was finished with him and that if he ever saw him again he would kill him. He (Perindi) immediately left the hunting grounds they had shared and set up camp at a far distant site.
The men lived separate lives, for months, or years. Eventually, both married. Harrimiah grieved for his brother.
One day, while out hunting, the twins unexpectedly came face to face. Perindi sprang on Harrimiah, sank his teeth into his throat and tore away skin. Their families were nearby and separated the men.
Perindi's attack alienated his wife and her family and they drove him away from their camp. He then lived alone and ‘developed peculiar habits’.
Harrimiah was also changed after the attack. He spent many nights by himself, away from his camp. He continued to say that he wanted to win back the affection of his twin. He felt his heart ‘would melt with sorrow’.
When hope of a reunion faded, Harrimiah dug a pit and lay down it. The wind blew sand over him, his tears were swallowed up by the sand, and the pit became his grave.
These twins have had a close relationship until adulthood. They were both skilled and competent and well regarded by those who knew them. There is no evidence of early psychopathology
Perindi was the subject of splitting, when a young woman told him that Harrimiah had been claiming superiority. This was almost certainly inaccurate, given the attitude of Harrimiah toward Perindi over subsequent years. Whether this statement was accurate or inaccurate is unimportant. An initial response of anger, such as purposefully painting his twin poorly, would be within the bounds of a normal reaction.
Shortly after the conversation with the young woman, Perindi came to believe what he has been told. This could suggest the prodrome of a psychotic disorder. When accused of having painted his brother poorly, Perindi became boastful, saying that he had a better body than his twin and that he was a better dancer. This is a change from his usual demeanour, and perhaps this suggests mood elevation.
The next day when Harrimiah was congratulated for his dancing, Perindi became very angry, threatened the life of his twin should they ever meet again, and permanently left their hunting grounds. This suggests the irritability of mood elevation, although a paranoid disorder could not be excluded.
On the occasion of their unplanned meeting, Perindi responded with inappropriate violence. His response was not culturally sanctioned, and resulted in his expulsion from his camp by his wife and her relatives. He then lived alone and ‘developed peculiar habits’. These details strongly suggest severe psychopathology.
Throughout the story there are mentions of Harrimiah's grieving for his brother. After the attack he felt his heart ‘would melt with sorrow’. He became socially withdrawn. He dug a pit in which he lay. He cried and did not resist as he was buried by sand blown over him by the wind. These details indicate distress beyond the normal reaction/grieving, and suggest major depressive disorder with suicidal behaviour.
The quality of the information is insufficient to make firm diagnoses. The story is thousands of years old, it was not investigated by a clinician with access to the DSM-IV, there was no psychological autopsy after the death of Harrimiah, and it has been recorded by oral means rather than written form. In contrast, the information that is provided on symptoms is presented in ordinary, clear language rather than technical terms. Over recent centuries, in the description of cases, the use of technical terms such as delirium and melancholia (which have meant different things at different times) has made recognition difficult.
The early life of the twins was unremarkable, except that they were both well regarded. The anger that Perindi displayed on at least two occasions and the fact that his behaviour was considered culturally inappropriate indicate a psychotic disorder. The sorrow that Harrimiah felt over the loss of his brother, his social withdrawal and his suicidal behaviour indicate more than a normal reaction and suggest major depressive disorder.
The fact that these men were twins does not add to our understanding of the genetics of psychopathology. It does burden us, however, with the task of attempting to reach a unifying diagnosis. Perindi may have suffered a paranoid psychosis and Harrimiah a major depressive disorder. It would be parsimonious and reasonable to conceptualize these twins as having suffered variants of bipolar disorder. This account of psychopathology antedates most others by millennia.
Hyperglycaemia secondary to mirtazapine therapy in a 37-year-old man
A 37-year-old man, currently out of work, with a history of major depression and marijuana abuse was referred from the Community Mental Health Service to his general practitioner for treatment with antidepressants. He was initially prescribed venlafaxine. When he developed urinary symptoms, this was ceased and after a washout period he was prescribed mirtazapine.
Baseline bloods prior to commencement of mirtazapine indicated a fasting blood sugar level of 7.9 mmol L−1. Mirtazapine 30 mg nocte was commenced approximately 1 week later. After 1 month his fasting blood sugar level was 16.8 mmol L−1, and 23.3 mmol L−1 1 week after that.
Metformin 500 mg b.d. was then commenced. Random blood sugar level 10 days later was 18.8 mmol L−1 and gliclazide was added. This was increased to 160 mg b.d. over the next week. Fasting blood sugar levels remained high: between 12.5 and 22.1 mmol L−1, and random blood sugar levels peaked at 30 mmol L−1. Insulin was contemplated but the patient refused.
Approximately 2 months after commencement, mirtazapine was ceased. Blood sugar levels were closely monitored and gliclazide was withdrawn. Five days after cessation of mirtazapine, fasting blood sugar had dropped to 9.4 mmol L−1 and post-prandial blood sugar levels were 9.3, 6.2 and 6.5 mmol L−1. The patient had remained asymptomatic throughout.
Reports of glucose dysregulation due to mirtazapine are rare, but hyperglycaemia or worsening of glycaemic control has been reported in patients with or without diabetes who were receiving long term mirtazapine or other antidepressant therapy [1]. Hyperglycaemia or worsening of glycaemic control has been reported in patients with or without diabetes who were receiving long-term mirtazapine or other antidepressant therapy [2].
Chen et al. reported a 44-year-old woman with a history of depression and obsessive–compulsive disorder. She was diagnosed with hypertriglyceridaemia, acute pancreatitis and diabetic ketoacidosis 2 months after mirtazapine was prescribed [1].
It is well-known that many antidepressant medications increase the risk of appetite and weight gain, which may exacerbate type 2 diabetes [3]. Fisfalen and Hsiung reported a 32-year-old woman who sustained glucose dysregulation secondary to mirtazapine-induced weight gain [4]. (This patient also had a history of substance abuse, including marijuana). The present patient, however, actually lost weight during the period in which his blood glucose escalated. He had a rapid rise and fall in blood sugar levels corresponding to the institution and cessation of mirtazapine. This suggests that other mechanisms are at play.
Theoretically, one might expect mirtazapine to negatively affect insulin levels because increases of noradrenaline normally decrease insulin release, and mirtazapine increases noradrenaline [1]. But this is obviously a rare side-effect. In two out of three published cases of glucose dysregulation secondary to mirtazapine the patients used marijuana and further study is needed to ascertain if marijuana abuse interferes with glucose regulation during mirtazapine therapy. We have presented an unusual case of increasing hyperglycaemia presumably secondary to mirtazapine therapy. To avoid this complication we recommend baseline serum glucose and regular monitoring of blood sugar levels during mirtazapine therapy, particularly if marijuana is being used.
Abiotrophia endocarditis: the great masquerader
A 67-year-old man presented to St Vincent's Hospital, Melbourne, with increasing fatigue, poor concentration, anhedonia and increasing tearfulness. The patient also reported a loss of appetite, dyspnoea and significant weight loss of 10 kg over the prior 6 months. He had a previous history of mitral valve prolapse and bicuspid aortic valve disease that was under regular review by his physician and had recently been diagnosed with atrial fibrillation. He denied any history of fever, night sweats or arthralgia. On examination he was cachectic with evidence of a depressed affect and would frequently and unpredictably burst into tears during consultations. A psychiatric evaluation felt that the sudden and frequent bouts of emotional lability suggested the possibility of an underlying organic cause.
Inflammatory markers at presentation indicated an erythrocyte sedimentation rate f 10 mm h−1, white cell count of 7.2×109 L−1 and a slightly elevated C-reactive protein of 31 mg L−1. He also had a normocytic anaemia with a haemoglobin of 96 g L−1, which was felt to be consistent with anaemia of chronic disease. His albumin was 28 g L−1, which was initially attributed to his poor oral intake secondary to his possible depressive illness. Neurological imaging (magnetic resonance imaging/magnetic resonance angiography) indicated subacute right insular cortical infarct involving the middle cerebral artery territory (Figure 1).
T2-weighted magnetic resonance imaging of the head showing right insular cortical infarct.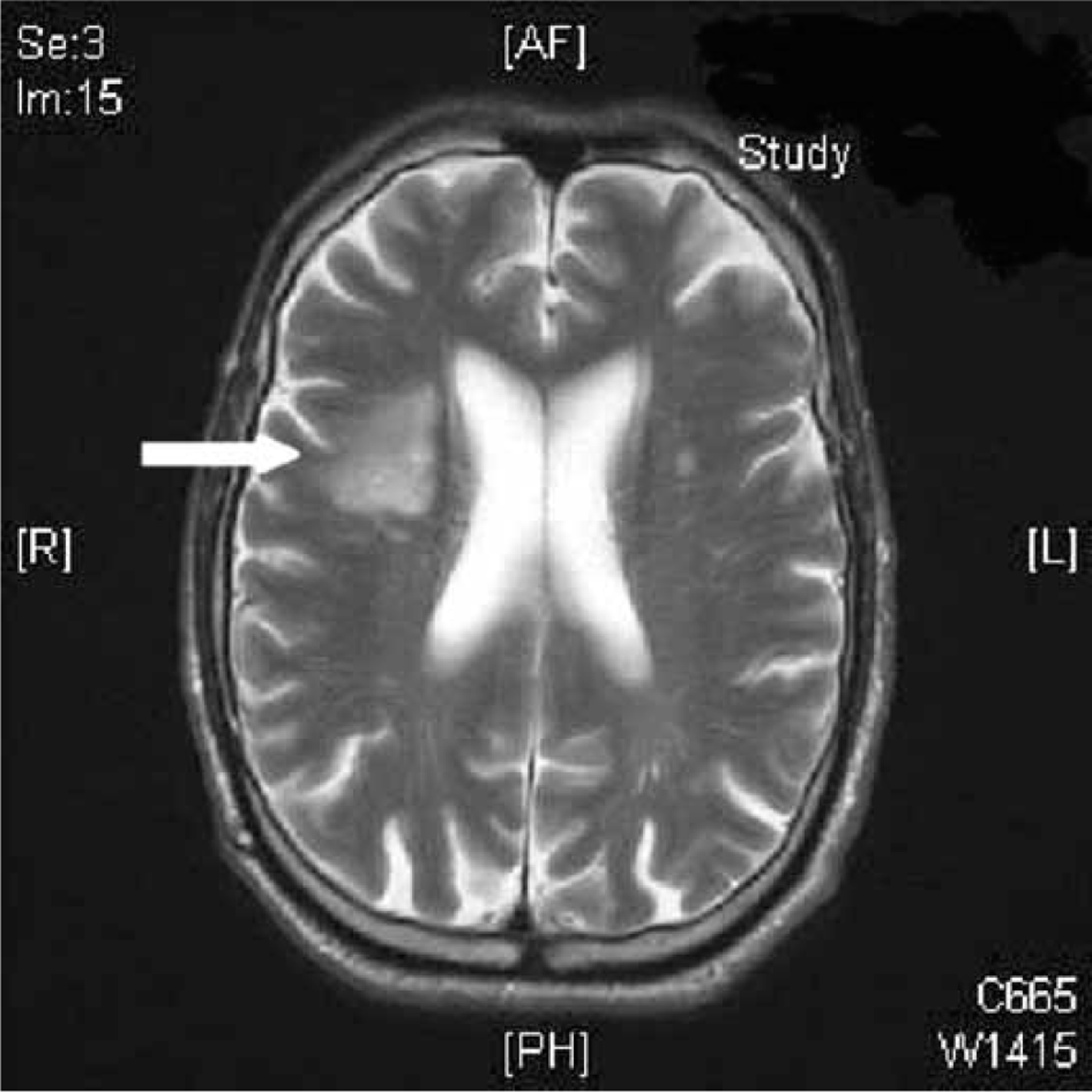
A transthoracic echocardiogram showed severe mitral valvular incompetence secondary to prolapse of the posterior mitral valve leaflet and an unchanged mean aortic valve gradient of 20 mmHg. Importantly there was no vegetation seen on initial echocardiographic evaluation. Eventually, after 4 days, blood cultures indicated Gram-positive cocci further characterized as Abiotrophia defectiva. Subsequent trans-oesophageal echocardiography indicated a small mobile mass on the anterior mitral valve leaflet consistent with a vegetation (Figure 2). A provisional diagnosis of abiotrophia endocarditis was made and the patient was commenced on i.v. gentamicin and benzylpenicillin. The patient was treated with 6 weeks of antibiotics and gradually his clinical condition improved. His appetite, weight and albumin increased. Importantly, his mood also significantly stabilized.
Trans-oesophageal echocardiogram showing vegetation on the anterior mitral valve leaflet (arrow).
Abiotrophia defectiva, formerly known as nutritionally variant streptococci, is part of the normal flora of the mouth and was first described in 1961 as an ungroupable viridans species [1] that has a high affinity for the endocardium [2]. It is responsible for 5% of all cases of streptococcal endocarditis [3] and has a higher mortality than endocarditis caused by other streptococci [4]. It can be difficult to identify because it does not grow on regular blood agar [5]. Combination therapy with benzyl penicillin and gentamicin is a recommended initial treatment strategy [6], but A. defectiva is often resistant to conventional treatment, requiring definitive surgical intervention to avoid fatal sequelae [7]. Neurological complications are the most common extracardiac manifestation of infective endocarditis, occurring in approximately 20–40% of cases [8]. Acute depression and mood instability are extremely rare presenting features. There is no evidence to suggest that there are increased neurological complications with A. defectiva.
This case highlights the diversity in presentation of endocarditis and that it should always be considered as a differential diagnosis in any patient who presents with initially unclear diagnostic features with pre-existing valvular disease. In this particular patient a presentation with depressed affect and weight loss without significant features of active infection predominated. The diagnosis was only established because blood cultures were collected, and those results directed further investigations for endocarditis. In patients with atypical neuropsychiatric presentations, careful clinical assessment is warranted to exclude organic disease.
Clinical applications of massage therapy for the management of psychiatric disorders besides anxiety
I read with great interest the recent pilot study by Garner et al. [1]. The authors have clearly shown that massage therapy may be a significant tool in decreasing stress as well as anxiety in psychiatric patients. The Garner et al. findings corroborate recent studies that suggest a significant role for massage therapy in the management of psychiatric disorders besides anxiety.
For instance, massage therapy improves depressive symptoms when used in patients with depression as well as in patients with bipolar disorders. In fact, a decline in the Hamilton Depression Rating Scale (HAM) by as much as 40% may occur in patients with depression [2]. Massage therapy is also effective in the management of eating disorders. For instance, Hart et al. have reported accentuation of dopamine levels and a decline in the body dissatisfaction element of the Eating Disorder Inventory in patients with anorexia nervosa [3]. Interestingly, massage therapy such as qigong massage therapy also improves language skills as well as social interactions in children with autism, while simultaneously decreasing stereotypic behaviour in these patients [5]. Interestingly, massage therapy such as qigong massage therapy also improves language skills as well as social interactions in children with autism [4]. For instance, Field et al. have shown that massage therapy administered on a daily basis to school children for as short a duration as 10 days is associated with decreased teacher-assigned hyperactivity scores [5].
Clearly, massage therapy has a significant adjunctive role to play in the management of a spectrum of psychiatric disorders ranging from depression to autism. There is a clear need to increase awareness about the usefulness of massage therapy both among psychiatrists as well as patients so as to fully make use of its beneficial effects.