
Abstract
Research has consistently found that those who care for a relative with psychosis are at increased risk of developing clinically significant levels of anxiety, depression, guilt and loss [1–3]. In addition, carers may be increasingly vulnerable to social pressures such as social stigma [4], and self-blame [5]. Poor psychological well-being, in turn, is associated with a poorer experience of caregiving for the carer, and is related to a poor quality of life and high levels of symptomatology for the psychosis sufferer [6]. Improving carer well-being may therefore improve the experience of caregiving and outcome for both carer and sufferer.
Learning that your child has a life-threatening illness is a criterion A event for post-traumatic stress disorder (PTSD) [7], for which prevalence rates are estimated at between 11% and 44% [8]. The incidence of PTSD is highest when a loved one has undergone aversive medical procedures, the outcome is uncertain, or when the onset occurred in distressing circumstances [7–9]. Research indicates that, at the onset of psychosis, conditions are often medically aversive and distressing for patients and carers [10], [11]. Furthermore, while psychosis may not be viewed as life threatening from a medical point of view, carers can interpret the risk of suicide and stigma [12] as potentially threatening. As suggested by previous research [13], [14], cognitive appraisals alone can lead to significant trauma reactions. Moreover, some carers become the subject of paranoid ideas or delusions, which result in their relative threatening, or causing them, actual bodily harm [5]. Thus, it is feasible to suggest that an episode of psychosis could qualify as a criterion A event for trauma.
Writing about traumatic events (written emotional disclosure) may ease the distress that those events cause [15–17]. Studies have demonstrated improvements in physical health and psychological well-being. Meta-analyses estimate the effect size of this intervention as between d = 0.15 and d = 0.47 [18], [19]. While there does not appear to be a consensus in how these findings should be interpreted [20], it is worth noting that most studies of emotional disclosure concern two key groups: physically healthy participants, and those with pre-existing physical health conditions. For these groups, who may not necessarily experience clinically significant levels of psychological distress, it is difficult to establish a significant reduction of distress due to potential ceiling effects. Furthermore, there is emerging support for the theory that written emotional disclosure is effective through the mechanism of exposure to previously avoided thoughts and feelings about the traumatic event [19], [21]. The enforced exposure may facilitate processing of the traumatic memories, in accordance with cognitive theories of traumatic reactions to events [22]. Therefore, it is possible that only participants experiencing post-traumatic stress at baseline may benefit from the intervention.
The aims of the present study were therefore to investigate whether carers experience trauma associated with a first episode of psychosis in their relative, and to evaluate an intervention, which may help them adapt to any such trauma. The following hypotheses were tested: (i) those who engage in written emotional expression of events related to their relative's psychotic experiences would experience greater physical well-being than those who write about neutral events; (ii) those who engage in written emotional expression of events related to their relative's psychotic experiences would experience greater psychological well-being than those who write about neutral events; and (iii) those who experience a significant level of trauma at baseline are more likely to benefit from writing about their relative's psychotic experiences than those who do not.
Methods
Research design
In order to test the aforementioned hypotheses, participants were randomly allocated to two groups. Each group had instructions to write either about their thoughts and feelings concerning the time that their relative first experienced psychosis (intervention group), or their own time management (control group). As participants were blind to the potential effect of their writing, it was important to clarify that the two groups had indeed written about qualitatively different experiences.
Participants
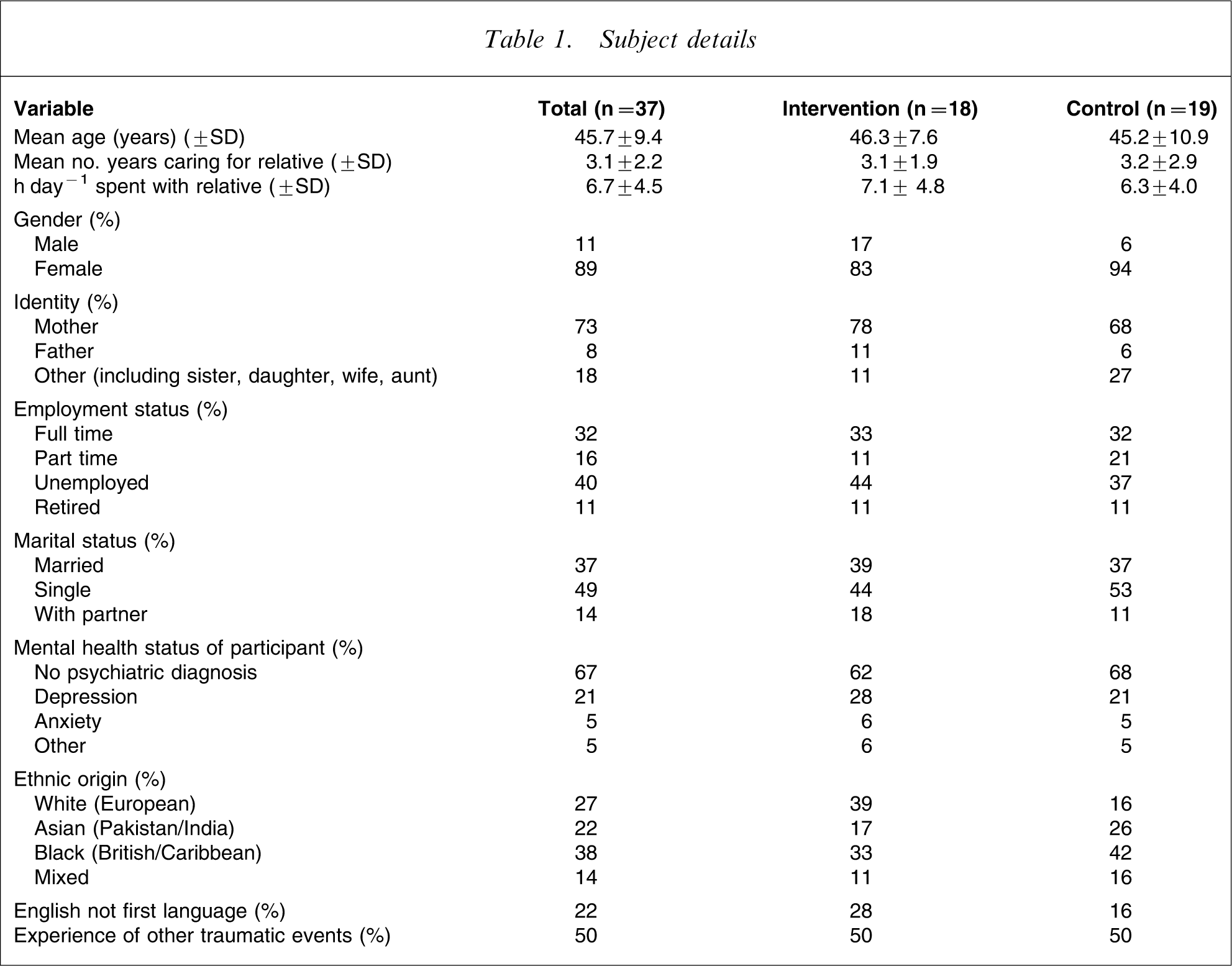
Carers of individuals whose difficulties met the ICD-10 criteria for a diagnosis of psychosis (F20; F22; F23; F25) from Early Intervention in Psychosis Services and a local charitable carers group were invited to take part. In terms of demography, those aged under 18 years were excluded because it was felt that their experiences would be different from those of adult carers. Also excluded were those unable to complete the assessment measures in English, because of difficulty in translating key concepts of those measures. While these were the a priori exclusion criteria, progress of referrals through the Consolidated Standards of Reporting Trials (CONSORT) diagram (Figure 1) shows that a further 36% of potentially eligible carers were excluded for clinical reasons. This may reflect the social and clinical complexity that exists not only for patients who experience psychosis, but for their families too. Thirty-seven people were recruited; demographic details of the sample are given in Table 1. Eighteen people were assigned to the intervention group and 19 to the control group. The average age of the sample was approximately 45 years and the majority were female (principally mothers of the psychosis sufferer). χ2 test indicated that there were no significant differences in sociodemographic details between the two groups, including factors that have been suggested to contribute to psychological burden (e.g. length of time spent caring and amount of time spent with the sufferer [6]). Forty-one per cent of those approached were recruited to the study (Figure 1), with a 10.8% attrition rate. The majority of the sample completed three writing sessions, although four intervention participants and five control participants completed fewer sessions. This was an intention-to-treat analysis.
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of progress through the trials.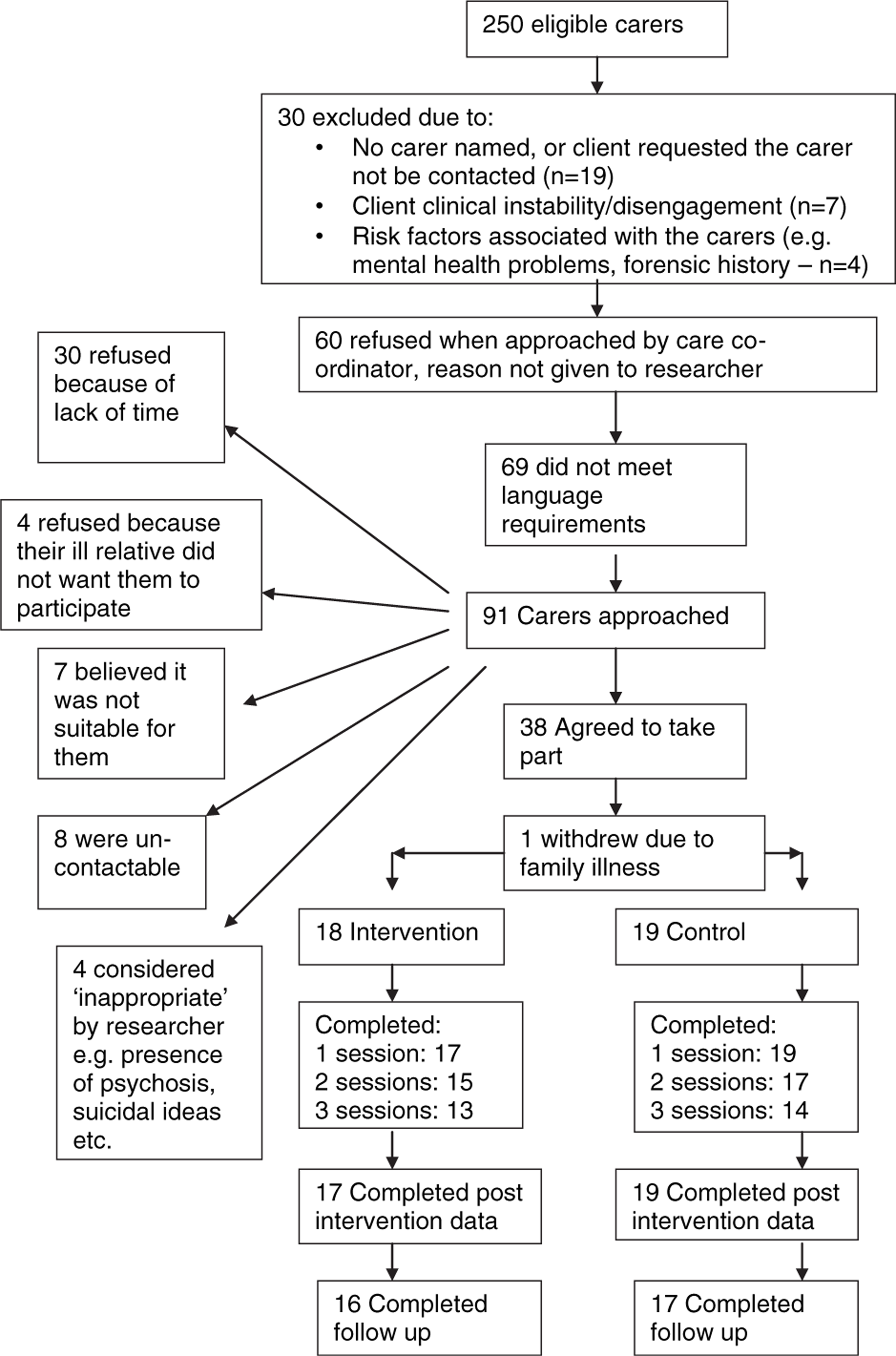
Subject details
Procedure
After completing baseline measures, participants picked one of several pre-prepared blank envelopes [23] containing the writing instructions. Participants were asked to write on three occasions for 20 min, over a 3 week period. Sessions occurred at a place of the participant's choosing; the majority (90%) elected to do so in their own home, in the presence of the researcher. Because of varying levels of literacy, and English often being only their second language, participants were offered the choice between writing and speaking about their experiences. Eight participants opted to speak about their experiences, recorded using audio equipment; the researcher gave no prompts or discussion. Previous research has shown that there are no significant differences between participants who write or speak about their experiences [24]. For ease of reference, the intervention will be described as ‘writing sessions’.
Following each writing session, participants were asked to complete a questionnaire that assessed their attitudes towards their essays. In previous research this questionnaire has been designed to ensure that participants in the two conditions are writing about qualitatively different topics, termed ‘condition manipulation’ [23]. Writing sessions were completed within an average of 21 days. After the third writing session participants re-completed the dependent measures. Three people wished to retain their writings and were therefore excluded from the condition manipulation data. All participants re-completed the dependent measures an average of 8.3 weeks after their final session.
Dependent measures
Demographics
Participants were asked their age, gender, relationship with the ill relative, marital and employment status, number of years caring and number of hours spent with that person per day, personal psychiatric history and whether they had previously experienced anything that they considered to be traumatic.
Trauma
Participants completed the Impact of Events Scale–Revised (IES-R) [25]. Respondents were asked to rate 22 statements relating to the first time their relative was ill, on a 5-point scale from 0 (not at all) to 4 (extremely). The revised version includes three subscales, based on the DSM-IV criteria for PTSD (intrusions, avoidance and hyperarousal). Although the factor structure of the IES-R does not support its use as a measure of PTSD, it is a reliable measure of post-traumatic stress [26]. It has high test–retest reliability for use as a repeated measure [27]. Cronbach's alpha for each subscale in the current study was also deemed to be very good (0.85–0.94). The IES-R correlates highly with the PTSD checklist (PCL), suggesting that scores >33 provide optimum diagnostic accuracy against the PCL [26], a score ≥33 will consequently be used to indicate post-traumatic stress.
Physical and psychological symptoms
The General Health Questionnaire-28 (GHQ-28) measures participants’ symptoms [28]. There are four subscales: somatic symptoms; anxiety and insomnia; social dysfunction; and depression; measured on a 4-point Likert scale ranging from 0 (not at all) to 3 (much worse than usual). A score ≥24 suggests ‘psychiatric caseness’ [29]. The validity of this scale is good (receiver operating characteristic = 0.88) [29]. Cronbach's alpha for subscales of the current data study ranged from 0.84 to 0.89.
Caregiver burden
The experience of burden was measured using the Experience of Caregiving Inventory (ECI) [30]. The 10 subscales group into two dimensions of burden: positive and negative. In the current study Cronbach's alpha coefficient ranged from 0.73 to 0.91. The measure asks participants how often they have considered each item during the month before the interview on a scale of 0 (never) to 4 (nearly always). A high score indicates greater difficulties on the negative subscales or more positive experience on the positive ones.
Condition manipulation checks
After completing their writing, participants were asked to complete a five-item measure with a 7-point Likert scale to measure mood, how meaningful, personal and emotionally revealing their essays were. Scales ranged from 1 (a lot) to 7 (not very much). This questionnaire was to ensure a subjective difference between the two conditions [23]. To verify that participants had written about qualitatively different topics the number of positive and negative emotion words in each essay were summed, as were the number of illness-related words (e.g. hallucinations, hospital, medication), cognitive insight words (e.g. knew, realized, understand) and personal and social pronouns (e.g. I, we, me). Categories reflected those used by Bernard et al.[31] and were analysed using a t-test.
Statistical analysis
Data were analysed using SPSS version 12.0 (SPSS, Chicago, IL, USA). A 2×3 repeated measures ANOVA model was used, in which group (treatment or control) formed the between-subject factor and time (baseline; after writing; and follow up) formed the within-subject factor. Previous work has suggested that there is greatest change among people who have experienced trauma [21]. Therefore, where the ANOVA reached significance, a further post-hoc analysis was used to ascertain the nature of this difference. The experimental groups were therefore divided according to whether they exhibited traumatic stress or not, according to IES-R caseness criteria [26].
Results
Essay manipulation checks
To verify that the two groups had written about qualitatively different topics, two manipulation checks were carried out. First, the content of the essays written in both groups was analysed using independent t-test statistics (Table 2).
Manipulation check of essay content (n = 32)
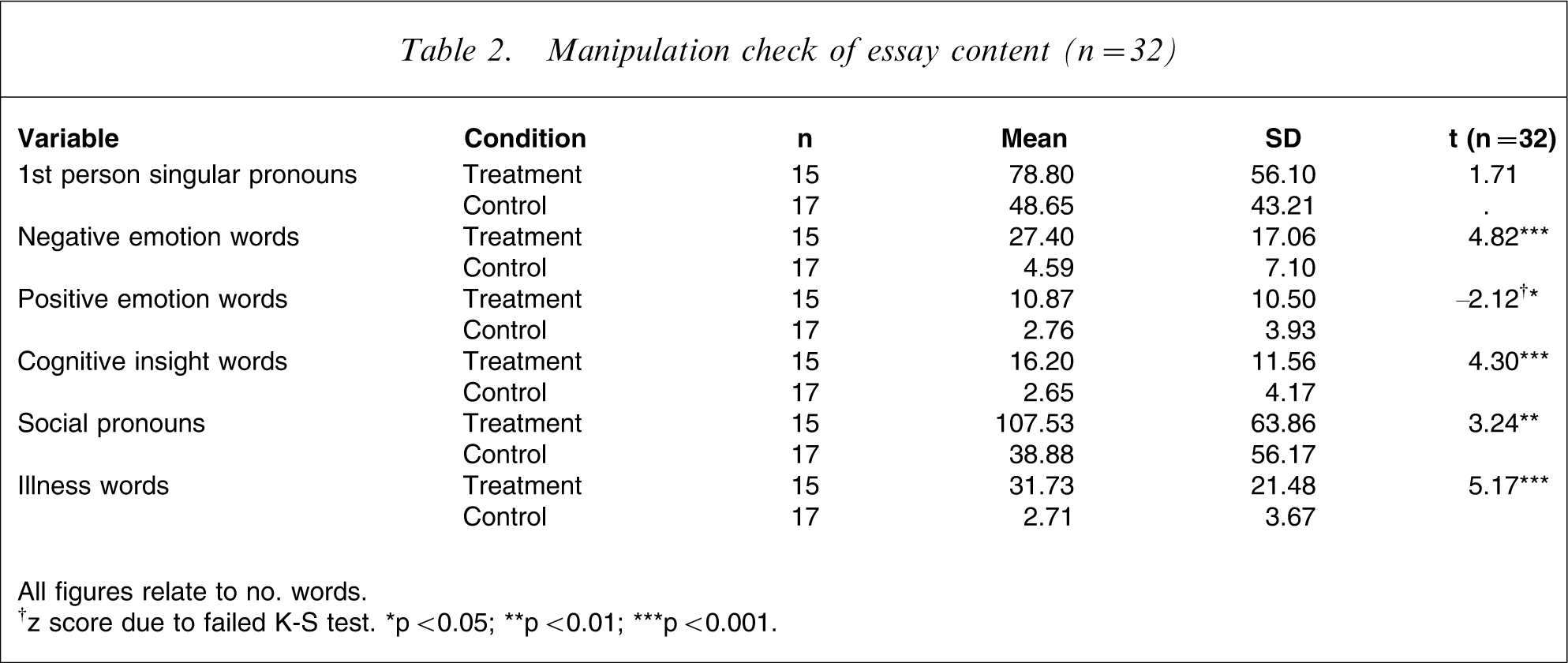
All figures relate to no. words
†z score due to failed K-S test. ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
The experimental group used more negative (t = 4.82, p < 0.001) and positive (z = 2.12, p < 0.05) emotion words as well as illness-related words (t = 5.17, p < 0.001) than did the control group. They also used significantly more insight words (t = 4.3, p < 0.001) and social pronouns (t = 3.24, p < 0.01). The increased number of first person pronouns among intervention participants failed to reach significance (p = 0.09).
Table 3 shows results of participant subjective essay ratings using independent t-tests. It suggests that participants in the treatment condition rated their writing as significantly more meaningful (z = 2.85, p < 0.01), more personal (t = 2.85, p < 0.001) and more emotional (t = 3.11, p < 0.001) than those in the control group. The frequency of discussing the topic with others was not significantly different between the groups (t = 0.75, NS). Nor was there any difference between conditions with regard to post-writing mood (t = 1.34, NS).
Manipulation check of essay evaluations (n = 32)
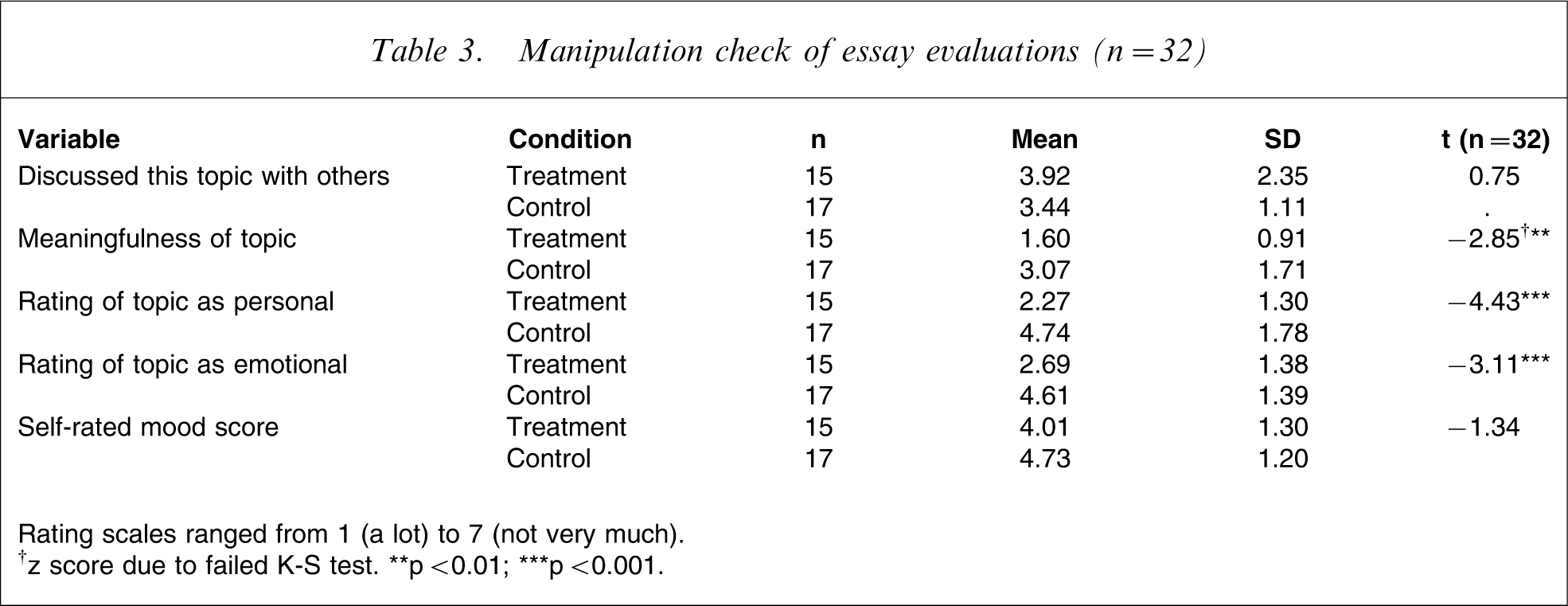
Rating scales ranged from 1 (a lot) to 7 (not very much)
†z score due to failed K-S test. ∗∗p < 0.01; ∗∗∗p < 0.001.
Dependent variables
The Kolmogorov–Smirnov test demonstrated that all data were normally distributed. t-tests of baseline data shown in Table 4 indicated that there were no significant differences in dependent variables between the groups at baseline. Mann–Whitney U-tests showed no significant differences in baseline data between participants who did and did not complete follow-up measures.
Impact of writing on all dependent measures (mean±SD)
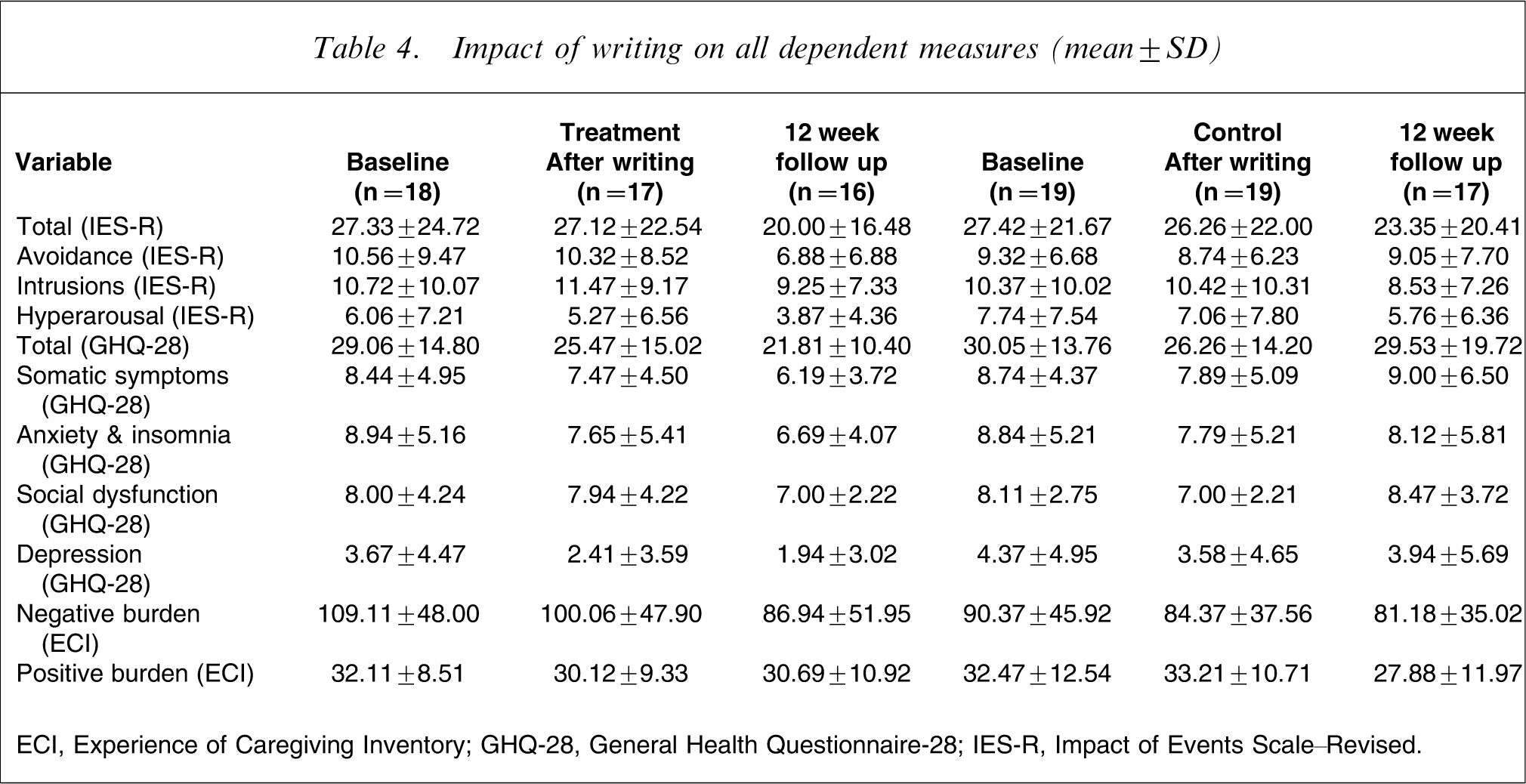
ECI, Experience of Caregiving Inventory; GHQ-28, General Health Questionnaire-28; IES-R, Impact of Events Scale–Revised.
Trauma (IES-R)
Using the Creamer et al. (2003) criterion (IES-R >33) [26], 32.4% (n = 12) of the sample met ‘caseness’ criteria for post-traumatic stress at baseline: five in the experimental group and seven in the control group.
In order to examine the effect of the intervention on individual symptoms of trauma, separate ANOVA calculations were carried out on the three IES-R subscales. This indicated an interaction effect (F(2,62) = 3.84, p = 0.05) on the avoidance subscale. There was, however, no interaction effect on the other two subscales: intrusions (F(2,62) = 2.17, NS) or hyperarousal (F(2,62) = 2.63, p = 0.08). There was no interaction effect on the total scores of the IES-R (F(2,62) = 0.27, NS).
Post-hoc analyses were carried out to further investigate the results. Table 4 shows high variation in the data. Although this did not violate assumptions required to calculate parametric statistics (Levene's F(1,31) = 2.77, p = 0.10), it was hypothesized that this may reflect distinct populations within the data; namely those who did and did not experience post-traumatic stress. In view of this, and in light of the small group sizes that resulted, Wilcoxon signed–rank tests were carried out to test whether those with high levels of traumatic stress were more likely to benefit from the writing intervention. The data were therefore split according to those who had and had not experienced trauma, according to the caseness criteria previously discussed. The results show a significant decrease in overall trauma symptoms (total IES-R) for those in the treatment group who experienced traumatic stress (z = −2.02, p = 0.03). This group also showed a decrease in avoidance scores between baseline and follow up, with a trend towards significance (z = −1.83, p = 0.06). Those in the control group both with and without trauma and those in the experimental group without trauma showed no significant changes in overall trauma or avoidance scores over time. These results are given in Table 5.
Overall trauma or avoidance scores over time (mean±SD)
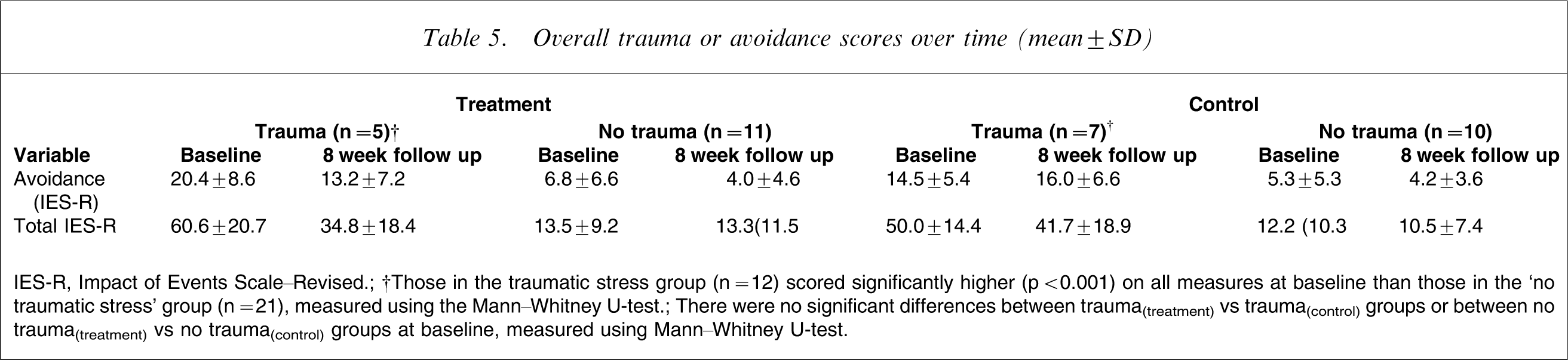
IES-R, Impact of Events Scale–Revised.
†Those in the traumatic stress group (n = 12) scored significantly higher (p < 0.001) on all measures at baseline than those in the ‘no traumatic stress’ group (n = 21), measured using the Mann–Whitney U-test.
There were no significant differences between trauma(treatment) vs trauma(control) groups or between no trauma(treatment) vs no trauma(control) groups at baseline, measured using Mann–Whitney U-test.
Physical and psychological symptoms (GHQ-28)
Using World Health Organization (WHO) criterion, (GHQ-28 > 24) 59.5% (n = 22) of the sample met psychiatric caseness criteria at baseline. While there was a change over time in total GHQ-28 scores with a trend towards significance (Mauchley's W = 0.754, G-G F(1.61,62) = 2.65, p = 0.08), there was no interaction effect Greenhouse–Geiser (G-G) F(1.61,62) = 1.6, NS).
Burden (ECI)
The ANOVA showed that both groups experienced significantly less negative burden over the time period (F(2, 62) = 6.82, p < 0.01). But there was no significant interaction effect, nor was there a time or interaction effect for positive burden. The ECI provides two scales of a relative's perceptions of their ill relative's symptoms: difficult behaviours and negative symptoms. Levels of negative symptoms are highly correlated with negative burden (r = 0.86, p < 0.01). When ‘negative symptoms’ was entered as a covariate into the ANOVA model, the effect of time was no longer significant for negative burden (F(2,60) = 0.73, NS).
Discussion
More than one-third of this sample (35.1%) reported symptoms of traumatic stress, defined here as IES-R > 33 [26]. This figure is similar to that reported by carers of children with physical health problems [8], [9]. To the authors’ knowledge this is the first study to examine traumatic stress in carers of people with psychosis and to suggest that writing about their experiences can help alleviate these problems. Specifically, that those who exhibited traumatic stress at baseline were most likely to experience reduced trauma as a result of the intervention. The post-intervention reduction in ‘avoidance of intrusive thoughts’ can be considered crucial, because avoidance may contribute to the inhibition of emotions and cognitive processes [22], [32]. Therefore, in those individuals who avoid emotions, reducing that avoidance may provide other psychological benefits. Furthermore, if emotional disclosure through writing is a means of encouraging exposure to previously avoided events, it is possible that it will be effective only when high levels of avoidance exist. Although other studies have found similar results [33], [34], to our knowledge this is the first to differentiate between those who do and do not experience traumatic stress within a clinical population.
Those who wrote about emotive experiences did not experience fewer intrusions or hyperarousal than those who did not. The impact of exposure on avoidance is likely to be more immediate than on the other symptoms of trauma [31]. The lack of change in the two subscales may have contributed to a non-significant change in overall trauma symptoms. It might be helpful to examine this result in a larger sample.
The number of people meeting WHO criterion (GHQ-28 > 24) for psychiatric caseness (59.5%) in this sample is similar to levels found in other studies of carers [34]. In contrast, however, to some previous writing studies [18], there were no significant differences between the two groups in levels of physical or psychological symptoms after writing. Again this may be due to the degree of variation in the data, which may reflect two distinct populations in terms of the amount of post-traumatic stress experienced. But it may also be an artefact of the methodology; in contrast to previous research [18], the present study asked people to write about a specific event, not any event in their lives, which they found to be traumatic. This may explain why those who found this event traumatic experienced significant changes in levels of trauma and psychological symptoms, but those who did not failed to experience the same benefit. Also in contrast to previous research, there was an absence of an increase in negative mood among the treatment group (Table 3). This may suggest that participants did not fully explore their thoughts and feelings as they had been instructed and, consequently, did not experience reduced burden, physical or psychological symptoms as would have been predicted. While it is possible that the number of years spent caring for a relative and the amount of contact with that person may impact on the amount of burden experienced by the sample [6], there was no difference between the two groups and therefore it should not have impacted on the principal analysis here.
The principal limitation to the conclusions drawn by this research is the small number of participants, increasing the possibility of a Type-I error. Although this was a risk, the number of participants recruited (41% of those approached), is similar to that used in other published research on this population [35] and the dropout figures were low (n = 4, 10.8%), these results may therefore be representative in this field. It should also be noted that, as a pilot study, the sample size presented here (n = 37) exceeds that of recently published studies within this field [31], [36]. Recruitment of this magnitude is to be expected within this population, in which there is still a high level of instability among sufferers, contributing to stress within families who often have other children to care for, some of whom are themselves experiencing problems. There were also high numbers of carers in the present study for whom English was not the first language, reflecting the inner city population from which the sample was drawn, and the relatively high degree of diagnosis within an immigrant population [37]. Therefore, in order to aid generalizability, it may be helpful for future studies to recruit from and compare a variety of sites, for example inner city and rural, and to be more precise with health staff about reasons for non-participation.
The present study, when analysed without differentiating between those who did and did not experience traumatic stress, supports the opinions of some researchers and reviewers [20], [38], [39] who suggest that writing about trauma produces little or no clinical benefit. But future work should consider screening participants for trauma-like symptoms, because an increasing number of studies have suggested that writing has been specifically effective in alleviating trauma and ruminative symptoms [19], [21], [40]. Not only does the present study support the use of this intervention to alleviate trauma, it also provides evidence that carers can also experience trauma as a result of witnessing a psychotic episode in their relative, and that writing about that experience can help.