
Abstract
Much has been done recently both within psychiatric circles and in society at large to understand public [1] and personal [2] attitudes towards mental illness. This has led to efforts to reduce negative opinion [3–5], but such work has largely ignored personality disorders. Despite the absence of clear evidence, there has long appeared to be a reluctance to use the term ‘personality disorder’ in mental health services except as one of criticism or rejection [6]. The reasons why personality disorder should be singled out for opprobrium are difficult to disentangle but almost certainly multifactorial. Factors such as a lack of training, therapeutic nihilism, negative countertransference or poor diagnostic reliability may all play a role. The attitudes of mental health workers may also play a significant role in the negative attributions associated with this diagnostic label and this has not been well researched.
Goffman described stigma as ‘an attitude that is deeply discrediting within a particular interaction’ [7]. Receiving such attitudes may lead to negative self-appraisal [8] and make developing a therapeutic interpersonal relationship difficult. Such relationships are important in the management of personality disorder [9], despite the difficulties inherent in the diagnosis. An awareness of stigmatizing attitudes enables clinicians to be reflective, an important facet of many treatment approaches towards personality disorder [10], [11].
This is clinically important because personality disorders are common in community mental health settings, where they present in more than half of all patients [Newton-Howes G: unpublished data, 2008, [12]. This compares to rates of between 4% and 12% in the community [13]. They are distressing conditions for patients and are associated with poorer outcomes for those with comorbid axis I disorders [14]. Despite this, the assessment of personality is often negligible in a clinical setting and its impact poorly considered [15]. Although this may be due to an implicit recognition of the current stigma attached to this diagnostic term, such a stance may prevent management options from being considered, and reflection within the clinical team.
Some work has already been done to identify the beliefs and attitudes of patients [16] and society [17] towards a diagnosis of personality disorder. The present study reports the attitudes of mental health clinicians towards patients with a diagnosis of personality disorder. By comparing this group to a group with personality disorder whose diagnosis is not known by mental health professionals, the attitudes of clinicians towards the diagnostic label, rather than the behavioural manifestations of that label can be made. The primary null hypothesis was that there would be no measurable difference in the attitudes of mental health professionals to patients with a clinical diagnosis of personality disorder and those with an instrument-rated diagnosis of personality disorder. The secondary null hypothesis was that any difference, if found, could be explained due to greater global psychopathology, need, social functioning or documented aggression, these being potential confounders.
Methods
The primary aim of this research was to identify the perceived difficulty in managing patients with personality disorder by staff in a secondary mental health setting. In order to do this a secondary analysis of the Comorbidity of Substance Misuse and Mental Illness Collaborative (COSMIC) [18] data set was undertaken.
Sample
The data set was collected between January 2001 and February 2002 in four urban centres in England: two from greater London, Nottingham and Sheffield. A two-phase approach was used. The complete population in secondary treatment within addiction and community mental health settings were identified on the census date and staff were asked to complete a questionnaire about each patient (phase I). All staff were mental health professionals, primarily from medical, nursing and social work backgrounds. Of this sample 400 patients were chosen at random and interviewed. Their case notes were also reviewed. The patients within a community mental health setting who were interviewed are reported on here. All community mental health teams conformed to English standards [19], including having an assigned mental health professional. Ethics approval was obtained from the four local ethic research committees. Each patient had the study explained to them and gave written informed consent to participate.
From this sample four groups of patients were identified: those without clinical or instrument-derived personality disorder; those without instrument-derived but with clinically derived personality disorder; those with personality disorder identified by instrument but not clinical diagnosis (‘covert personality disorder’); and those with clinical diagnosis and instrumental diagnosis of personality disorder (‘overt personality disorder’).
Assessment tools
Axis II diagnoses were generated using the Quick Personality Assessment Schedule [20], a rapid and easily applied form of the Personality Assessment Schedule (PAS) [21] that allows for both categorical and cluster diagnosis of personality disorder to be measured. Although no one assessment of personality disorder can be regarded as superior to any other, the PAS has been shown to have good psychometric properties with a four-factor structure [21] that has been replicated many times since; high cross-national interrater reliability [22]; and independent support for its validity in longitudinal studies of self-harm and in those with anxiety and depressive disorders [23], [24].
Potential confounders were measured in a variety of ways. Overall psychopathology was measured using the Comprehensive Psychopathological Rating Scale (CPRS) [25]. Social functioning was assessed in two ways. First an objective measure of social need was obtained using the Camberwell Assessment of Need [26]. It measures the objective needs of patients across 22 domains. The scores indicate whether a need is met, partially met or unmet and a larger score indicates a greater level of unmet need. The Social Functioning Questionnaire [27] was used to provide a subjective assessment of social functioning from the patient's perspective. It measures eight domains of social functioning on a Likert-type 4-point scale and gives a total score (range = 0–24), with higher levels indicating worsening social functioning. Physical aggression was chosen as an objective measure of aggression because it is objective and quantifiable.
Mental health professionals were directly asked for their beliefs about managing patients. Their answers were recorded using five bipolar domains on a Likert scale. The five domains were (i) Difficult to manage–Easy to manage; (ii) Stable–Chaotic; (iii) Aggressive–Docile; (iv) Good engagement–Poor engagement; and (v) Compliant–Non-compliant.
Statistical analysis
All data were analysed using SPSS (SPSS, Chicago, IL, USA). Mann–Whitney U-tests were used to compare the data relating to the five perception domains because the data were skewed. Student's t-tests were used to compare social and psychopathological morbidity outcome scores because these data were normally distributed. Only predetermined analyses was undertaken testing a priori hypotheses to minimize the possibility of type I error.
Results
Demographic characteristics
Patient characteristics are shown in Table 1. This shows a secondary care population with a high degree of psychiatric morbidity and poor social functioning. The average patient within a community mental health setting was 40 years old (range = 29–52 years), Caucasian and currently unemployed. They typically had one psychiatric diagnosis and two of every five had at least one personality disorder diagnosis.
Patient characteristics
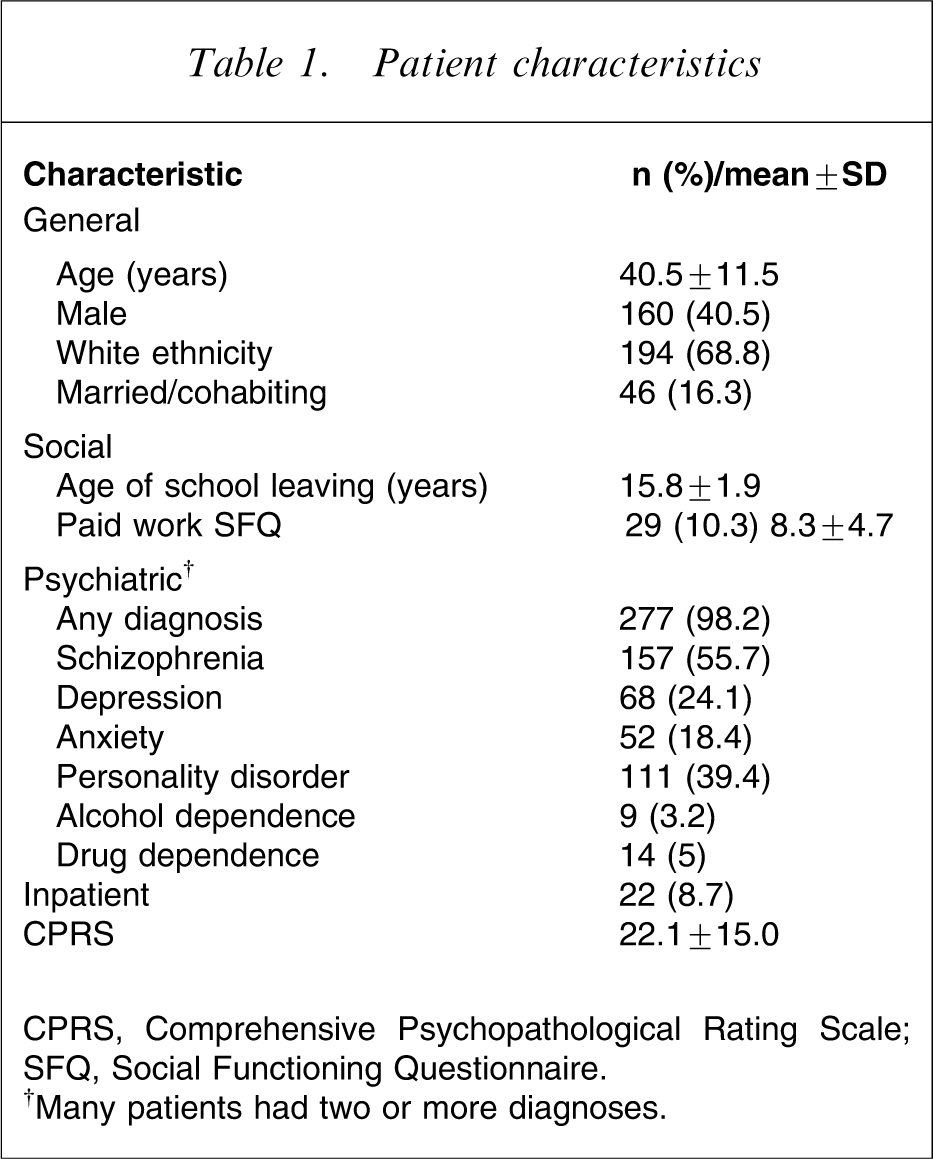
CPRS, Comprehensive Psychopathological Rating Scale; SFQ, Social Functioning Questionnaire.
†Many patients had two or more diagnoses.
Personality disordered versus non-personality disordered patients
Of the four patient groups only three patients (1%) had a clinical diagnosis of personality disorder without an instrument diagnosis and were therefore omitted from further analysis. When all personality disordered patients, using clinical or instrument diagnosis, were compared to non-personality disordered patients, mental health professionals believed those with personality disorder to be more globally difficult to manage, more aggressive and less compliant, as shown in Table 2.
Perceived difficulty in managing PAS-Q-diagnosed PD vs no PD
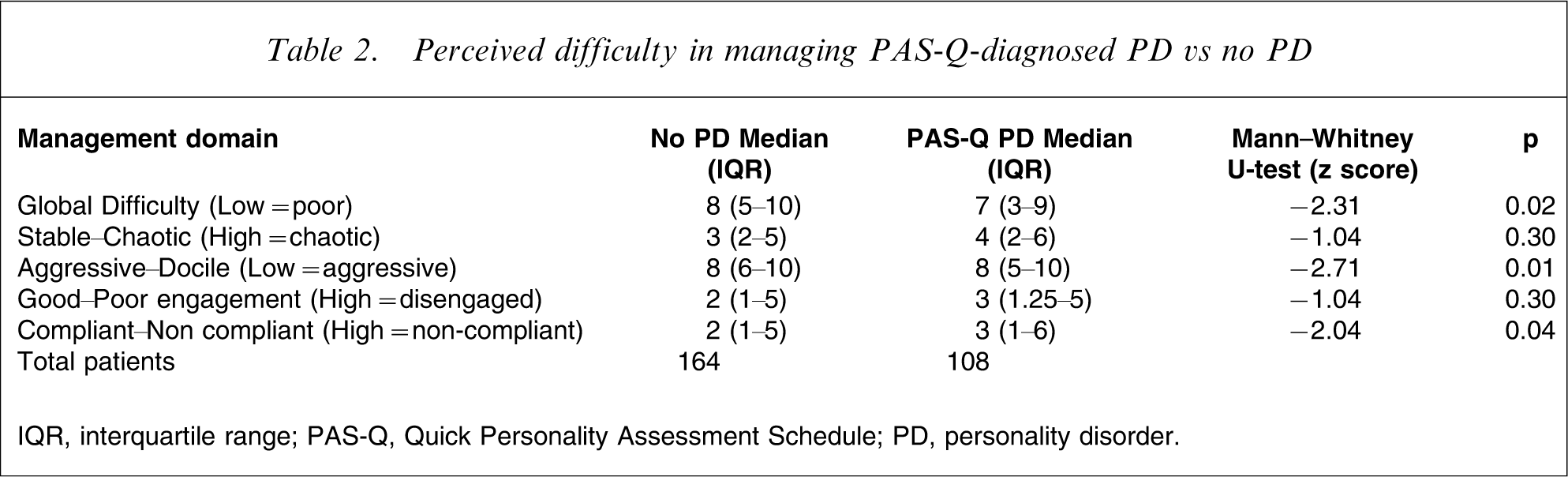
IQR, interquartile range; PAS-Q, Quick Personality Assessment Schedule; PD, personality disorder.
Overt versus covert personality disorder
The group of 108 personality disordered patients were then sub-analysed. This group was divided into the overt and covert personality disordered patients, allowing diagnostic labelling to become the independent variable. When these two groups were compared, mental health professionals considered overt personality disordered patients to be globally more difficult to manage, more chaotic and more aggressive (Table 3).
difficulty in managing clinically diagnosed vs PAS-Q-diagnosed PD
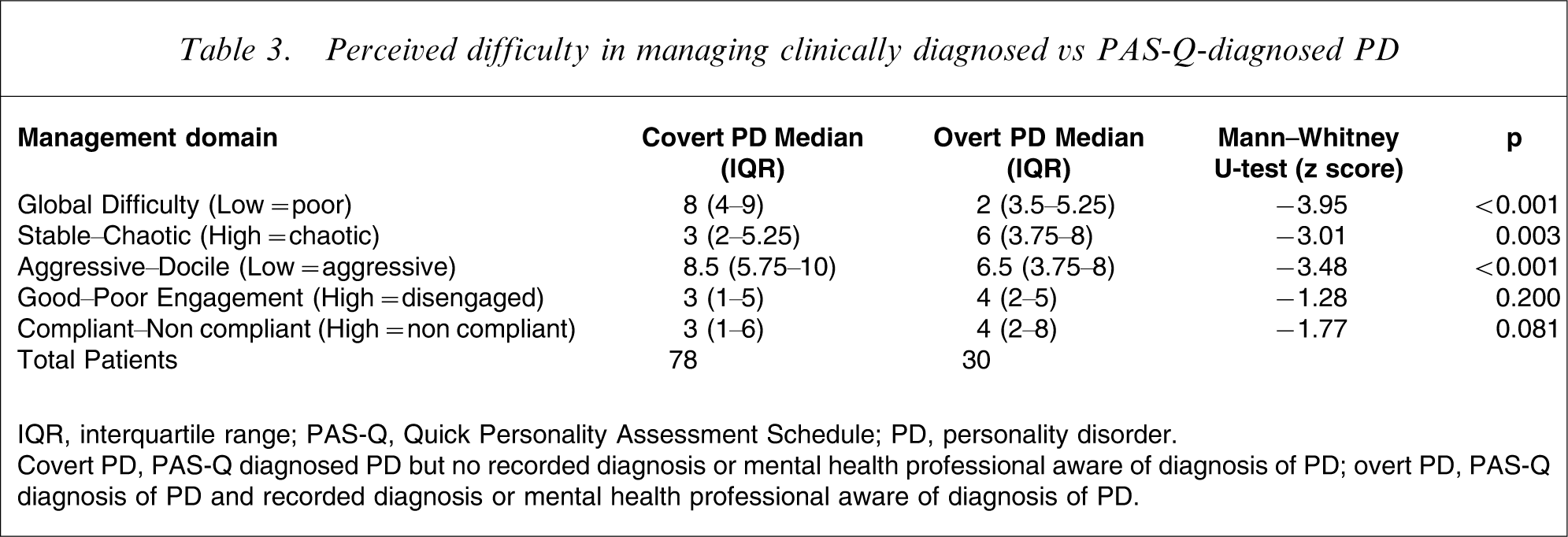
IQR, interquartile range; PAS-Q, Quick Personality Assessment Schedule; PD, personality disorder.
Covert PD, PAS-Q diagnosed PD but no recorded diagnosis or mental health professional aware of diagnosis of PD; overt PD, PAS-Q diagnosis of PD and recorded diagnosis or mental health professional aware of diagnosis of PD.
Global psychopathology, need, social morbidity and aggression were compared between the overt and covert groups to assess if they accounted for the beliefs of mental health professionals in an objective fashion. The two groups showed no difference in aggression towards staff, overall social need or social functioning. The overt group did, however, have statistically more psychopathology as rated by CPRS (Table 4).
Psychiatric and social morbidity (mean±SD)
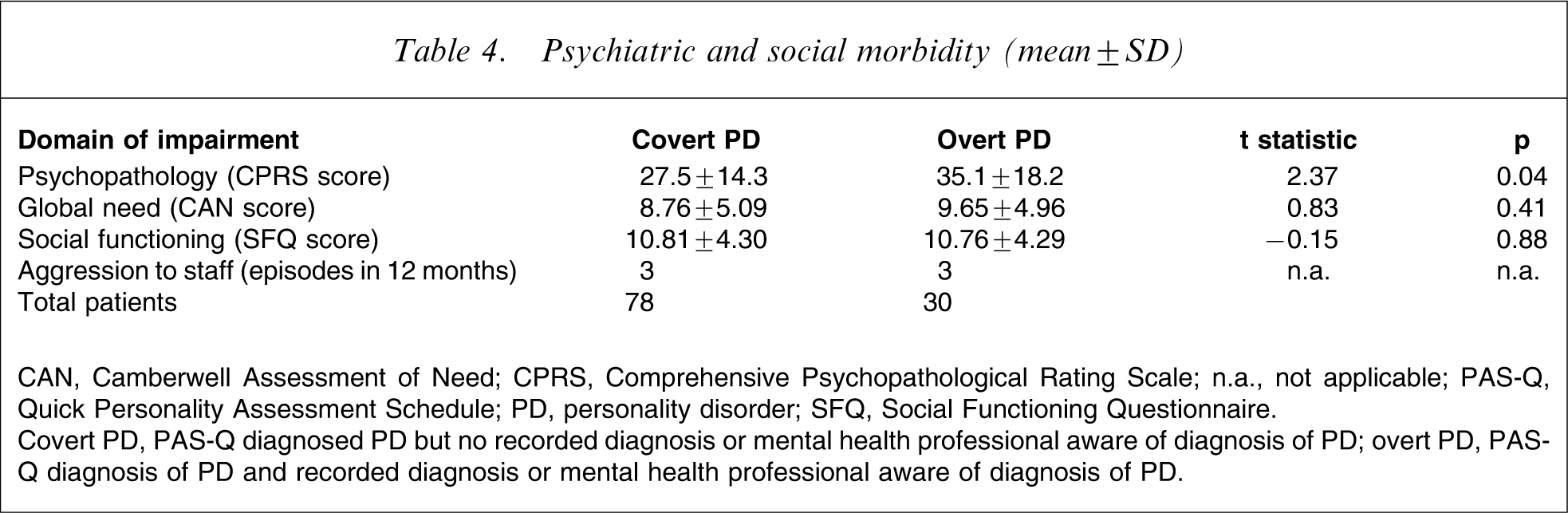
CAN, Camberwell Assessment of Need; CPRS, Comprehensive Psychopathological Rating Scale; n.a., not applicable; PAS-Q, Quick Personality Assessment Schedule; PD, personality disorder; SFQ, Social Functioning Questionnaire.
Covert PD, PAS-Q diagnosed PD but no recorded diagnosis or mental health professional aware of diagnosis of PD; overt PD, PAS-Q diagnosis of PD and recorded diagnosis or mental health professional aware of diagnosis of PD.
Discussion
This paper identifies that patients with an overt diagnosis of personality disorder are believed to be harder to manage by clinicians than those with a covert diagnosis of personality disorder. This attitude is not a direct consequence of greater need, social functioning or aggression. Although it is not possible to identify why this is the case, a diagnosis of personality disorder was the variable used to differentiate the groups and such diagnostic labelling is most likely to be the reason for this finding. This would be in line with historical attitudes towards personality disorder [6] and is not countered by the findings of research into attitudes towards mental illness, which tend to overlook personality pathology.
Although the present study is indicative of a negative attitude towards a diagnosis of personality disorder, it has a number of limitations. The most significant, as is common with personality disorder studies, is the debate about the diagnostic validity of this label and the variation between clinical and instrumental measures. For the COSMIC study the interviewers all received formal training using the PAS and were not permitted to proceed to formal evaluation until good agreement on rating had been reached. All formal personality assessments yield greater numbers of individuals with personality disorder than do clinical assessments and the PAS errs on the conservative side, by ignoring present pathology if it is present, and assesses only the premorbid personality of the subject, even if this was present only many years earlier. Clearly we do not have evidence that a PAS rating of personality disorder is superior to a clinical one but the additional evidence from the present study suggests that there are no clinical reasons for suggesting a fundamental difference between those diagnosed using the research instrument and those diagnosed clinically. This is, for example, highlighted by the similarities between the two personality disordered groups in ratings of social functioning. Second, the overt personality disordered group of patients had greater psychopathology than the covert group. The finding of greater global psychopathology in this group has been identified in other research studies [28] and might partly explain the more negative attitudes towards the overt, personality disorder-labelled group. Both groups, however, had very high CPRS scores, suggesting both groups had significant clinical symptomatology. It is therefore unlikely that this accounts for all of the difference in clinician attitudes towards these two groups. Third, many other measures could have been used to assess possible confounding variables. The clinical outcomes chosen aligned with the five bipolar domains of attitudes tested and were selected as quantifiable, objective outcomes. Although other measures, such as perceptions of threat, could have been chosen, these would have been subjective and directly linked to the primary measures of attitude. Fourth, no account was taken of the treatment being received by each patient. It was not clear if management was directed towards any recognized personality disorder or the management of any major mental disorder. It would have been expected, however, if personality management was active in the overt group that mental health professionals’ attitudes would have been more positive, because part of the management of personality disorder usually involves managing countertransference and developing a positive therapeutic relationship. This was not the case. Finally, because this was a cross-sectional study, the association between negative beliefs and overt personality disorder is associative not causative.
Despite these limitations the present paper highlights the need within a secondary care setting, where personality pathology is significantly higher than in the general population, to be aware of not only the possibility of a personality diagnosis but also the need to address a potentially negative professional attitude towards it. Negative attitudes are part of the stigmatizing position, as outlined by Goffman, and cannot only hinder management but can also have a negative impact on outcome.
Footnotes
Acknowledgements
This work was undertaken by the authors who received funding under the Department of Health's Drug Misuse Research Initiative (grant no.: 1217194). The views expressed in this publication are those of the authors and not necessarily those of the sponsors. The authors would like to express their gratitude to the sponsors for supporting this work.