
Abstract
Perinatal mood disorders are common, distressing and have the potential for long-term consequences for both mother and baby [1], [2]. While postnatal depression has received the most attention, antenatal depression is increasingly recognized as a serious problem. Indeed, in some studies the incidence of antenatal depression has been found to be higher than that of postnatal depression [3]. Antenatal depression increases the risk of adverse outcomes for both mother and infant. Pregnant women who are depressed are less likely to attend antenatal care and education and are more likely to smoke, use alcohol and other substances and neglect their diet and self-care [4], [5]. Antenatal depression is also likely to affect the way the woman perceives her fetus, with consequences for her subsequent attachment to her baby.
Depression and anxiety during pregnancy have been shown to be risk factors for postnatal depression [6–8]. Other risk factors for postnatal depression include a past history of depression, marital conflict, single parenthood, young age, lack of support, recent stressful life events, a family history of psychopathology, a history of severe maternity blues, negative cognitive style, depression in the partner, obstetric complications, adverse birth experiences and problems with infant health, temperament and behaviour [8], [9].
Given that antenatal factors can influence postnatal outcomes, an antenatal screening instrument would be very useful. This would potentially identify women at high risk in the antenatal period, enabling appropriate intervention to be provided, and would also identify women at greater risk of postnatal disorders. The APQ is a self-rated instrument developed at the Southwest Sydney Area Health Service, designed to be administered by midwives at antenatal clinics to collect information about a range of psychosocial risk factors and identify candidates for multidisciplinary mental health evaluation and management.
The aim of the present study was to evaluate the usefulness of APQ in women attending the Lyell McEwin Health Service (LMHS) in the northern suburbs of Adelaide. The study examined the prevalence of the various APQ risk factors in this population, and investigated the association between APQ risk factors and depression, measured using the EPDS [10]. The LMHS catchment area is characterized by high rates of unemployment, substance abuse, single motherhood, violence and social dislocation. In 2003 the unemployment rate in the suburbs surrounding the LMHS was 22.1%, with 73.4% of the population dependent on welfare payments [11]. Women living in situations of psychosocial disadvantage are more likely to experience the various risk factors for postnatal depression, and more likely to lack good social and financial support following the birth of their baby.
In 2001, 12.2% of women birthing at LMHS were under 19 years of age. Compared to the state averages, the women birthing at LMHS tended to be younger, more likely to be single mothers and more likely to have complicated pregnancies and deliveries. They were also twice as likely to have had more than four previous live births, and to attend fewer than seven antenatal hospital visits. The perinatal mortality rate was 13.5 per 1000 births, compared with the state mean of 10.4 per 1000 births [12]. These figures indicate that besides psychosocial disadvantage, these women have a number of risk factors for poor obstetric outcome, which also increases their risk of postnatal depression. This population was therefore well suited to assess the utility of the APQ, and the association between risk factors identified on the APQ and antenatal depression.
Method
Participants
All women presenting for antenatal care at the LMHS between June 2003 and December 2003 were offered the opportunity to participate in the study. Of the 431 eligible women, 421 provided complete data. Sixty-six (15.7%) of the women were aged 15–19 years, 240 (57%) were aged 20–29 years and 115 (27.3%) were ≥30 years. The present study was approved by the Ethics Committee of the North West Adelaide Health Service and all women gave written informed consent.
Measures
Study participants completed the 13-item APQ and the 10-item EPDS following their initial triage interview with a midwife. The APQ contains questions about practical and emotional support, emotional problems, self-harm, violence and substance abuse [12], [13]. Responses to individual questions on the APQ were analysed to assess the prevalence of the various psychosocial risk factors. Depressive symptoms were measured using the EPDS, a self-report scale with favourable internal consistency [10], [14] previously validated in Australian samples [15]. We took EPDS scores of ≥10 to indicate depression [16], [17]. This threshold of depressive symptoms has been demonstrated as having optimal sensitivity (86.7%) and specificity (91.5%) among pregnant women [16].
Referral to mental health services
At the initial triage interview the midwives refer women whom they assess as currently depressed or at risk of antenatal or postnatal depression, and women who have a history of depression or other serious mental illness, to LMHS Perinatal Mental Health Service. This service is staffed by a mental health midwife and a psychiatry registrar. These referrals continued during the study.
In addition we were concerned that information collected during the study should be utilized to improve the detection of antenatal depression in study participants. The APQ and EPDS were scored within 1 week and women scoring ≥10 on the EPDS were sent information regarding depression in pregnancy and postnatal depression, along with an invitation to contact the Perinatal Mental Health Service. Women who scored ≥12 on the EPDS and women who responded positively to question 10 on the antenatal psychosocial questionnaire (thoughts of self-harm) were also telephoned by the mental health midwife.
Statistical analysis
Results are reported as mean±SD. Analysis was undertaken using SPSS version 12.0 (SPSS, Chicago, IL, USA). Logistic regression analysis using the EPDS cut-off as the dependent variable was performed to determine the degree to which the psychosocial variables were associated with EPDS caseness. A stepwise forward procedure was used in the regression modelling process, with the entry threshold set at p = 0.05 and the exit threshold set at p = 0.10 for all variables. Where appropriate, the ‘sometimes’ and ‘yes’ categories for the psychosocial questionnaire were collapsed into one variable for this analysis.
Results
Incidence of antenatal risk factors
Three hundred and seventy-four women (88.8%) responded positively to one or more questions about psychosocial risk factors (Table 1). While data were complete for all other items, not all women answered the questions about substance use. Sixteen women (4%) did not answer the question about smoking, and 70 (20%) and 76 (22%) did not answer with regard to drugs or alcohol, respectively.
Prevalence of antenatal psychosocial risk factors
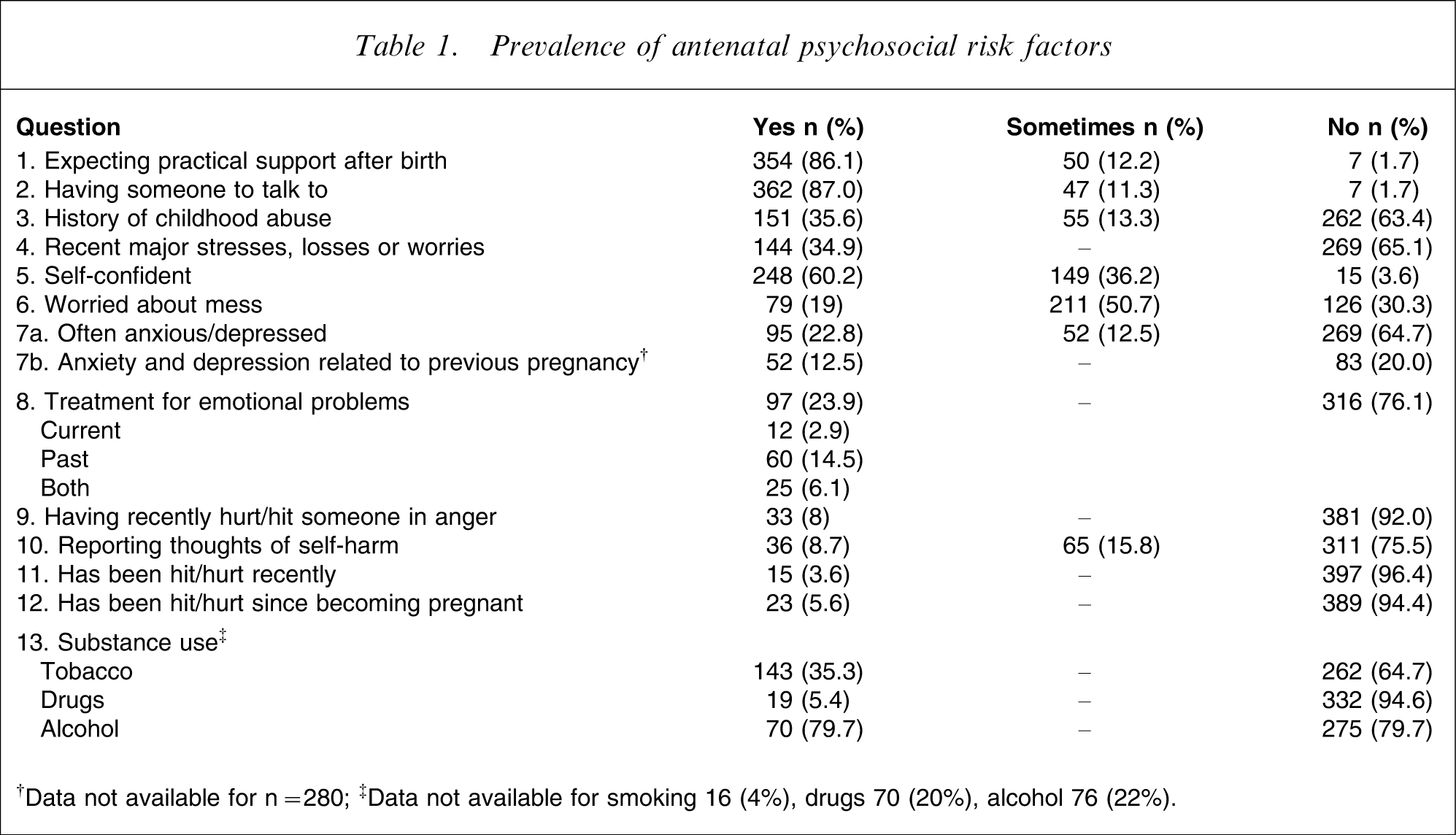
†Data not available for n = 280; ‡Data not available for smoking 16 (4%), drugs 70 (20%), alcohol 76 (22%).
Depression
One hundred and sixteen women (29.7%) had scores indicative of clinically relevant depression (≥10 on the EPDS). Sixty-nine women (17.7%) scored ≥13 on the EPDS, indicating a very high likelihood of current depression. The mean EPDS score was 7.54±5.26.
Relationship between antenatal psychosocial risk factors and antenatal depression
Of the 13 psychosocial risk factors examined using a stepwise (entry/removal criteria) logistic regression procedure for associations with caseness on the EPDS, seven risk factors remained significant in the final model, indicating that they are predictive of EPDS caseness (Table 2). Violence (either hitting others or being a victim of violence), having feelings of depression/anxiety, requiring both past and current treatment for emotional problems, and obsessionality significantly increased the risk of antenatal depression, while having someone to talk to and feeling confident significantly reduced the risk of antenatal depression.
Stepwise logistic regression predicting antenatal depression.
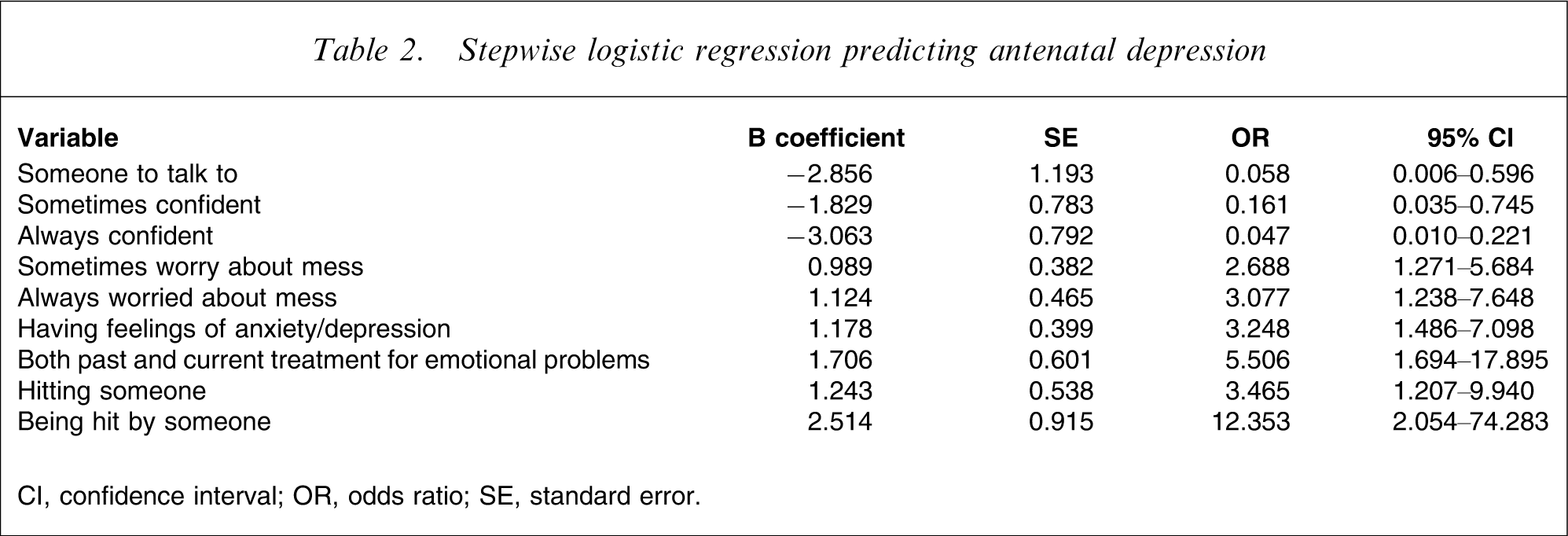
CI, confidence interval; OR, odds ratio; SE, standard error.
Discussion
We found a high prevalence of psychosocial risk factors in women attending the LMHS antenatal clinic. Comparison with data from South West Sydney [13] shows that 88% of the LMHS women and 52% of the South West Sydney women endorsed one or more risk factors. In particular, women attending the LMHS antenatal clinics were more likely to have been abused as children (35.6% vs 8.0%), to have suffered recent major life stresses (34.9% vs 24.5%), to have thoughts of self harm (24.5% vs 4.3%), to have been victims of violence since becoming pregnant (5.6% vs 1.5%) and to admit to recently hitting or hurting people in anger (8% vs 3.8%). It is likely that these differences reflect the social disadvantage experienced by women living in the LMHS catchment area. The high rates of endorsement of the various risk factors indicate that women birthing at the LMHS are a very vulnerable group.
The incidence of depression, measured using an EPDS cut-off of ≥10, was 29.7% for the LMHS women, again higher than the rate of 23.5% reported in South West Sydney [13]. This rate is also above the national average (19.6%) reported in a recent Australia-wide population survey of more than 40 000 women using the same EPDS caseness criterion [18].
The APQ was effective in identifying psychosocial risk factors associated with antenatal depression. Some of these results are especially worrying. Eight per cent of women admitted recently hitting or hurting people. These women may have difficulties with impulse control and anger management, which could have implications for the safety of the baby. We found that 5.6% of the LMHS women were currently victims of domestic violence, comparable to the prevalence (5.8%) reported by Webster et al. for pregnant women in Australia [19], but higher than that of Matthey et al. who reported a 1.5% prevalence among pregnant women in South West Sydney [13]. A study of pregnant urban Aboriginal and Torres Strait Islander women found that 15.1% were victims of domestic violence, although it is not clear whether this is current violence, and the researchers did not ask about violence by the women towards others [20]. A recent report of antenatal screening of a large number of pregnant women did not identify violence as a risk factor for antenatal depression [18]. It is not clear whether this reflects failure to ask about violence, or whether violence is more prevalent in socially deprived regions. The present results do suggest that, given the high risk of harm to the woman and her children as well as the association with depression, attention should be given to asking about and addressing violence by or towards pregnant women. A recent study in Ireland demonstrated that questions about violence are acceptable to 99% of pregnant women [21].
The high proportion of women endorsing the item regarding child abuse is concerning given that childhood abuse is associated with depression in later life [22]. Surprisingly, thoughts of self-harm were not associated with current depression.
We identified two protective factors. The first was emotional and social support (having someone to talk to) and the second was self-confidence. These factors can potentially be strengthened by targeted perinatal programs for those women who struggle in these areas.
The APQ was acceptable to the women with high rates of participation in the study. The present study demonstrated that risk factors can therefore easily be identified at antenatal intake interview. However, some women avoided answering the questions about substance abuse, suggesting that this information may need to be addressed using other methods, for example as part of the initial triage interview.
The APQ provided data that were valuable at both an individual and a clinic level. Comparison between the present results and those for the South West Sydney women shows an overall pattern of greater risk among the LMHS women. The use of screening instruments can therefore be useful in identifying the populations in greatest need, with implications for resource allocation. However, there are other antenatal psychosocial risk instruments available, for example the Antenatal Psychosocial Health Assessment (ALPHA) developed in Canada [23]. It would be helpful if there was international agreement on the best instrument to use, to allow comparison of data and meta-analytic research.
These antenatal risk factors can potentially be countered with early intervention and treatments prior to birth. Unfortunately, although the benefits of identifying at risk women seem intuitive, evidence in this area is limited. A systematic review has found that there is a paucity of rigorous randomized and controlled trials of antenatal interventions [24]. Nevertheless, the concept of identifying women at risk using brief, well-validated screening instruments measuring psychosocial risk factors and current depression, as in the present study, is likely to be beneficial in measuring the effects of targeted interventions in future studies.
The public health importance of perinatal depression screening is highlighted in a recent large-scale Australian study [18]. However, screening is of little benefit without easily accessible perinatal mental health services to provide appropriate support, treatment and follow up. The Perinatal Mental Health Service at LMHS includes specialized psychiatric and mental health midwife services, assertive outreach, a closed 10 week cognitive behaviour therapy group and an open support group, and close liaison with obstetricians, midwives and social workers.
The limitations of the present study include use of a self-report measure of depressive symptoms rather than a structured psychiatric interview to determine caseness for depressive disorders. Anxiety symptoms were not measured and these are well known to be related to depression among pregnant women [25]. Women were recruited from a single disadvantaged region, and this may limit the conclusions drawn from this study. Also, we have used a psychosocial risk questionnaire that did not allow calculation of a total risk score.
Since the present study was completed we have continued regular screening with the EPDS, but have replaced the APQ with the Pregnancy Risk Questionnaire [26]. This is similar to the APQ but has the advantage of enabling calculation of a score to guide referral to perinatal mental health services. We have since adapted the Pregnancy Risk Questionnaire scoring to trigger differential referral to either psychiatric or social work services. We have also used the present findings to improve our input into antenatal classes, for example addressing the need to develop practical and emotional supports and discussing strategies to address perfectionism and obsessionality.
In conclusion, the present study demonstrates that antenatal screening is acceptable and effective. We discovered high rates of psychosocial risk factors and antenatal depression among this socioeconomically disadvantaged population. These women and their children are very vulnerable and the public health implications in terms of optimal allocation of resources are obvious.
Footnotes
Acknowledgements
The authors thank the midwives at the LMHS Maternity Service for their help. We also thank Professor Bryanne Barnett, of Southwest Sydney Area Health Service, for her help and support.