
Abstract
Keywords
Attention-deficit–hyperactivity disorder (ADHD) has been recognized as an early onset neuropsychiatric disorder with typical core symptoms of inattention, hyperactivity, and impulsivity [1], lasting until adolescence and even adulthood [2]. Due to its high prevalence in Western countries at 5–10% [3], and in Taiwan at 7.5% [4], and its persistent, pervasive behavioural problems and associated academic underachievement [5, 6], an investigation of the extent of its influence on a variety of domains of parental and family function, in addition to the well-known short-term and long-term impacts of ADHD on individuals [6, 7], is warranted.
Western studies suggest that the presence of ADHD in children is associated with varying degrees of disturbances in family and marital functioning [8, 9], disrupted parent–child relationships [8], high parental expressed emotion [10], more negative and conflicting communication [11], reduced parenting self-efficacy [12], increased levels of parenting stress [13, 14], maternal psychological stress [14, 15], and parental psychopathology [8, 16–18], particularly when ADHD is comorbid with conduct problems [19]. Both inattentive and hyperactive/impulsive symptoms are equally challenging to parents [10, 20].
Although these parental/family processes may not cause the onset of ADHD, they have been reported to contribute to the severity [21] and persistence [22] of ADHD symptoms, adherence to treatment [23], psychiatric comorbidities [21, 24], and long-term outcome [25]. Western literature has documented the impact of ADHD on family functioning, and the latter may modify the course of ADHD [26]; but little is known about the parental/family processes in relation to children with ADHD in non-Western countries. Ethnic Chinese families in Taiwan are greatly influenced by Chinese culture with its Confucian tradition, which emphasizes the patriarchal family, the family over the individual, children's obedience, children's academic achievement, and hierarchical relationships and responsibilities [27]. Like mothers in Western culture, Chinese mothers have the primary responsibility for child care, and are subjected to most of the difficulties of their children's ADHD symptoms and poor school performance [27, 28]. It is expected that having a child with ADHD would be a big challenge for ethnic Chinese parents, particularly mothers. In view of this, the present study aimed to examine the mother's psychological distress, parenting styles, and perceived family support, and the child's active interaction with parents and behavioural problems at home; and to identify the most correlated parental/family factors for ADHD among a large sample of clinical patients with ADHD, as compared with school-based controls. We anticipated that given the nature of the early onset of ADHD and its core symptoms within the context of ethnic Chinese families, raising a child with ADHD should have increased maternal psychological distress and adverse parental and family processes.
Methods
Sample recruitment
The Institutional Review Board of the Department of Health, Taiwan, and National Taiwan University Hospital approved this study prior to the recruitment of clinical subjects and multistage sampling of school controls in September 2003. Written informed consent was obtained from parents and teachers of school-based subjects and parents of clinical subjects after explanation of the purpose and procedure of the study; there was no obligation to participate in the present study, and reassurance of confidentiality was given in a letter from the investigator before recruitment.
Patients with ADHD
The clinical sample included 375 patients (329 boys and 46 girls), with a mean age of 10.7±2.9 years. There was no age difference between male (10.7±2.9 years) and female children (10.6±2.7years) with ADHD (p > 0.1); 274 clinical subjects were recruited consecutively from the psychiatric clinic of a medical center and 101 were recruited through the ADHD Educational Foundation in Taiwan from October 2003 to December 2003. The inclusion criteria for the ADHD group included 6–15-year-old children with a clinical diagnosis of DSM-IV ADHD and/or ICD-10 hyperkinetic disorder, who had been treated with immediate-release methylphenidate (IR MPH) for at least 6 months; and whose mothers were able to complete the questionnaires. Those ADHD patients who were under treatment for psychiatric disorders other than oppositional defiant disorder and conduct disorder, and/or systemic disease, were excluded from the study. Because mothers are the main caregivers of children in Taiwan and most clinical subjects were accompanied by their mothers during their visits, mothers of all the subjects were asked to complete the questionnaires about their psychological distress, parenting, and perceived family support, and their children's behaviours with them.
School controls
The original school-based population consisted of 2584 grades 1–9 students from 108 classes in Taipei, in which all the students were recruited using a multiple stage sampling method. The sampling has been described elsewhere [29]. Parents and teachers reported on the Chinese versions of the Conners’ Parent Rating Scale–Revised: Short Form (CPRS-R:S), and the Conners’ Teacher Rating Scale-Revised: Short Form (CTRS-R:S), respectively [29]. Each of the CPRS-R:S, a 27-item parent-reported rating scale, and the CTRS-R:S, a 28-item teacher-reported rating scale, consist of four subscales: the Inattention, Hyperactivity, Oppositional, and ADHD Index subscales with items rated on a 4-point Likert scale from 0 for not true at all (never, seldom) to 3 for very much true (very often, very frequent) [30]. According to the sex and age structures of the ADHD group, 750 control students were randomly selected from the original school-based subjects whose t-scores on the CPRS-R:S and CTRS-R:S were <70 at the ratio of 1 case to 2 controls.
Diagnosis of ADHD
The diagnoses of ADHD were made based on clinical interviews in accordance with the diagnostic criteria of DSM-IV ADHD and ICD-10 hyperkinetic disorder, and further confirmed by the ADHD supplement from the Schedule for Affective Disorders and Schizophrenia for School-Age Children–Epidemiologic Version (Kiddie-SADS-E). The Chinese Kiddie-SADS-E has been widely used in epidemiological studies on childhood and adolescent mental disorders in Taiwan [4, 31]. The clinical diagnosis was made by board-certified child psychiatrists with extensive clinical research experience, who obtained information from parent and child interviews, observation of child's behaviours, and rating scales reported by parents and teachers. The first assessment took around 1.5–2 h. The final clinical diagnosis was made usually after at least three visits of assessment. Methylphenidate and behavioural therapy were the main treatment modalities. In general, methylphenidate was prescribed to those patients with either DSM-IV ADHD combined type or ICD-10 hyperkinetic disorder. The exclusion criteria for the ADHD group have minimized the heterogeneity of the ADHD group.
Measures
Chinese Health Questionnaire
The Chinese Health Questionnaire (CHQ), a 12-item self-reporting questionnaire modified from the General Health Questionnaire [32], includes symptoms of anxiety, depression, insomnia, and somatic complaints, and has been widely used to identify those who have minor psychiatric disorders in primary care and the community in Taiwan [33].
Chinese version of the Parental Bonding Instrument
The Parental Bonding Instrument (PBI) is a 25-item instrument (item-rated on a 4-point Likert scale from ‘very likely’ to ‘very unlikely’) measuring parenting styles during the child's first 16 years with three principal dimensions: care/affection (12 items), overprotection (seven items) and authoritarianism (six items) [34]. A high score on the care/affection subscale reflects affection and warmth, while a low score indicates rejection, or indifference. Overprotection reflects overprotective parenting and denial of the child's psychological autonomy; authoritarianism reflects the degree of parental authoritarian control over the child's behaviour [35]. The reliability and validity of the Chinese PBI has been described elsewhere [36].
Chinese version of the Social Adjustment Inventory for Children and Adolescents
The Social Adjustment Inventory for Children and Adolescents (SAICA), a 77-item scale, is designed for parental reporting about their children's four domains of functioning [37]. A higher mean score (items rated on 4-point Likert scale from 1 to 4) indicates either poorer social functioning or a more severe social problem [37]. Interactions with mother and father, and problems at home were the three selected dimensions of Home Behaviours for this study. Items for the Interactions with Mother (Father) included ‘Does things with mother (father)’, ‘Is friendly/affectionate toward mother (father)’, and ‘Talks with mother (father)’. Items for the Problems at Home included ‘Reject parent's instruction’, ‘Risky behaviours at home’, ‘Destroys household property’, and ‘Physical aggression toward parents’. The psychometric properties of the Chinese SAICA have been described elsewhere [38].
Chinese version of the Family APGAR
Family APGAR, a 5-item measure, is designed to assess the five dimensions of perceived family support by asking whether ‘I am satisfied (i) with the help that I receive from my family when something is troubling me (Adaptation), (ii) with the way my family discusses items of common interest and shares problem-solving with me (Partnership), (iii) that my family accepts my wishes to take on new activities or make changes in my lifestyle (Growth), (iv) with the way my family expresses affection and responds to my feelings such as anger, sorrow, and love (Affection), and (v) with the amount of time my family and I spend together (Resolve)’. Each item was rated on a 3-point Likert scale: 0, hardly ever; 1, some of the time; 2, almost always. A higher score indicates a more highly functional family [39]. The Chinese Family APGAR has been used in assessing perceived family support for individuals with mental problems [40] and for student populations in Taiwan [39].
Statistical analyses
Statistical analyses were performed using SAS 9.1 (SAS Institute, Cary, NC, USA) and RTREE statistic software [41, 42]. The descriptive results of comparing the demographics between the case and control groups were demonstrated in frequency, percentage, and χ2 statistics for categorical variables; and mean, SD, and t statistics for continuous variables.
Analysis of covariance was used to compare the mean scores of parental and family measures between the ADHD and control groups with control for parental age and educational level. The maternal CHQ score was controlled in the model for the analysis of parenting, home behaviours, and perceived family support. Cohen's d was used to compute the effect size (standardized difference between the two means) for the two groups [43].
Three-way interactions between sex and school grade levels and the other covariates, as well as two-way interactions between sex or school grade level and the other covariates and all the main effects from parental and family measures were tested in the multivariate logistical regression model with backward selection to identify most associated parental and family factors for ADHD.
RTREE statistical software was used to conduct a tree-based risk factor analysis, a non-parametric multivariate statistical method [41]. Its advantages over parametric multivariate modelling include the fact that it requires no assumption regarding a linear combination of explanatory variables; it is easy to assess the interaction or effect modification because no a priori contrast needs to be specified; it can deal with missing data; and it is suitable for hypothesis-generation analyses. Thus, it provides an integrated picture of explanatory factors that interact with each other, and defines subgroups that are at higher or lower risk. The χ2 test was used to prune the regression tree. The critical value of χ2 test statistics at 1 df was presented, and a probability 0.01 was used to prune the tree. The odds ratio (OR) and 95% confidence intervals (CI) were provided for each splitting variable based on the Cochran-Mantel-Haenszel test. The aforementioned independent variables were used to distinguish the ADHD group from the control group.
Results
Sample description
There was no difference in sex and age distributions between the ADHD group (329 boys and 46 girls, mean age±SD = 10.7±2.9 years) and school controls (658 boys and 92 boys, 10.6±2.5 years, F1,1122=0.77, p = 0.38). The ratio of male to female was 7.2. Mothers of children with ADHD (college and above, 42.9%; senior high, 45.0%; junior high and below, 12.1%) were more highly educated than those of the controls (college and above, 40.3%; senior high, 39.3%; junior high and below, 20.5%; χ2=11.95, df = 2, p < 0.003). Fathers of children with ADHD (college and above, 53.1%; senior high, 35.8%; junior high and below; 12.1%) were higher educated than those of controls (college and above, 49.4%; senior high, 30.5%; junior high and below, 20.1%; χ2=14.41, df = 2, p < 0.001). Despite statistical significance (p = 0.002) due to large sample size, there were similar ages between mothers of ADHD children (40.2±5.1 years) and mothers of school controls (39.2±4.8 years). There was no difference in fathers’ ages between the two groups (p = 0.099).
Individual effects
Table 1 presents the mean scores of the CHQ and the subscales of the Chinese PBI, Family APGAR, and Home Behaviours of the Chinese SAICA for the ADHD and control groups. The analyses were controlled for the parents’ current ages and education levels, and maternal CHQ score. Compared to the mothers of the controls, the mothers of children with ADHD had greater psychological distress, perceived less family support, and showed less affection/caring parenting style (effect sizes ranging from 0.43 to 0.69). Compared to the controls, children with ADHD had less active interaction with their mothers and fathers and had more severe behavioural problems at home (effect sizes ranging from 0.78 to 0.85). Moreover, mothers of children with ADHD may have greater overprotection, and an authoritarian controlling parenting style toward their children than their counterparts with small effect sizes (Table 1).
Parental and family measures
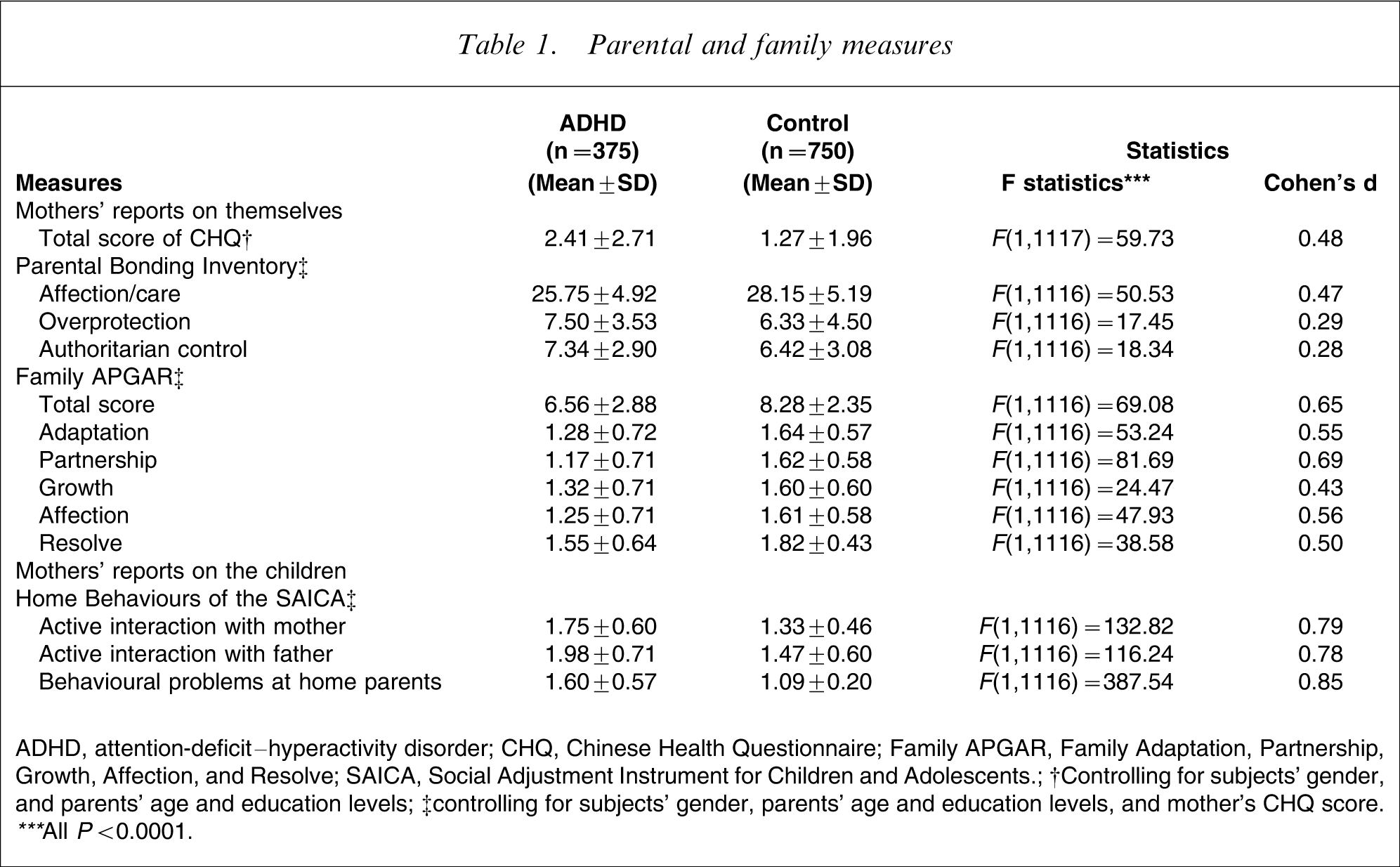
ADHD, attention-deficit–hyperactivity disorder; CHQ, Chinese Health Questionnaire; Family APGAR, Family Adaptation, Partnership, Growth, Affection, and Resolve; SAICA, Social Adjustment Instrument for Children and Adolescents.
†Controlling for subjects’ gender, and parents’ age and education levels; ‡controlling for subjects’ gender, parents’ age and education levels, and mother's CHQ score.
∗∗∗All P<0.0001.
Modification from age and sex
There was no sex or age difference in most of the parental/family measures (p = 0.062–0.880) with the following exceptions. Boys had less active interaction with their fathers (p = 0.003) and mothers (p < 0.0001), and experienced more authoritarian control from their mothers (p = 0.003) than girls. In terms of the age effect, increased age of subjects was associated with decreased affection/care (p = 0.0003) and authoritarian control (p = 0.0018) from their mothers, and less active interaction with their mothers (p < 0.0001) and fathers (p < 0.0001).
Regarding the modification effect of age, the gap between the less maternal perceived family support in the ADHD group and the control group increased with the children's age only in the domains of family adaptation (β = − 0.032, t = − 2.14, p = 0.033). There was no interaction between age and ADHD status on other parental or family measures. Moreover, the magnitude of difference in parental and family measures between the ADHD and controls did not vary between boys and girls.
Final fitted model
Table 2 presents the OR and 95%CI for the parental and family variables significantly associated with ADHD after backward selection in the multivariate logistical regression model. The most significant correlates for ADHD were less active interaction with fathers and mothers, more severe behavioural problems at home, and maternal perception of less family support. Maternal psychological distress and parenting styles were not included in the final fitted model.
Final fitted model for ADHD
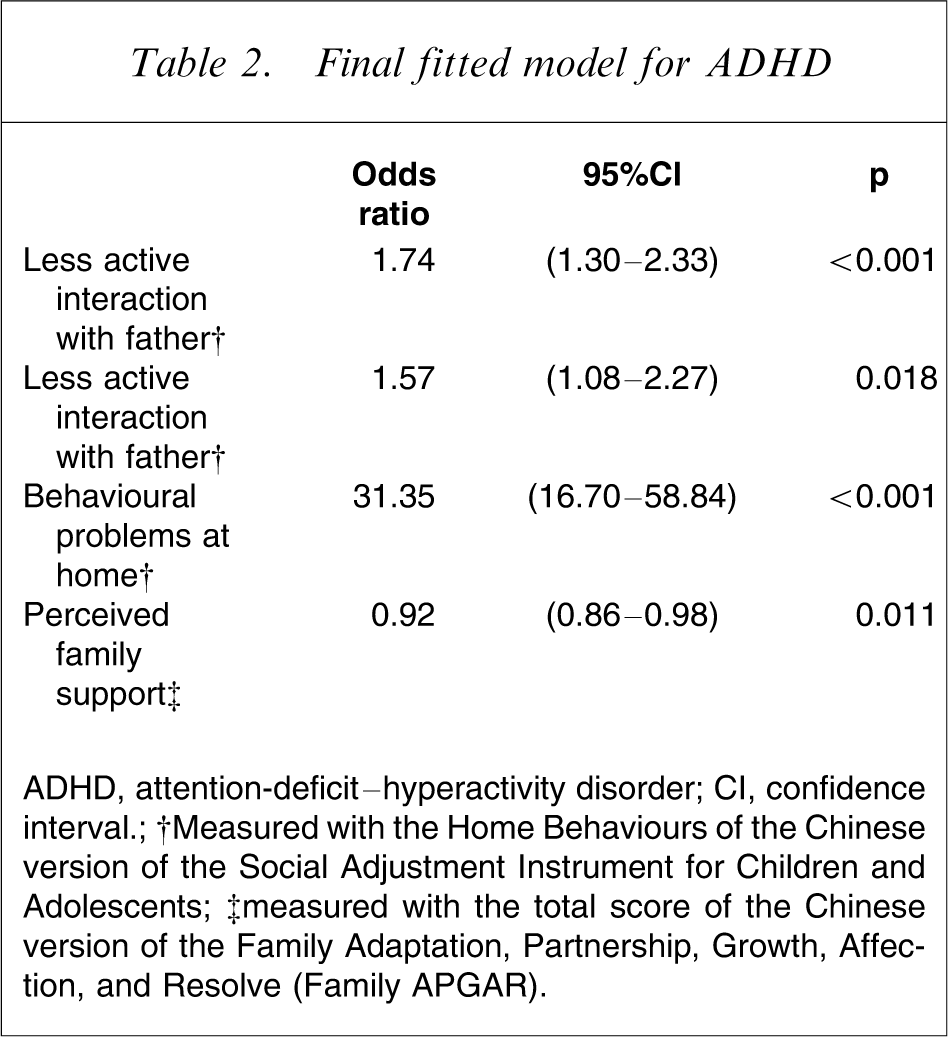
ADHD, attention-deficit–hyperactivity disorder; CI, confidence interval.
†Measured with the Home Behaviours of the Chinese version of the Social Adjustment Instrument for Children and Adolescents; ‡measured with the total score of the Chinese version of the Family Adaptation, Partnership, Growth, Affection, and Resolve (Family APGAR).
Multivariate analysis using tree-based regression model
Figure 1 presents the results of tree-based regression analysis. The circles represent internal nodes, including the root node. The internal node is defined as a node with daughter nodes. The square boxes represent terminal nodes, which are defined as nodes without any daughter nodes. The number of subjects with ADHD and controls, and the χ2 statistic are shown inside the circles or square boxes. The identifying number of nodes and each terminal node are shown at the borders of nodes [44]. Figure 1 also displays the splitting variables and values for each note of the regression-tree model for the ADHD and control groups. Table 3 provides the OR and its 95%CI corresponding to each internal node in Figure 1.
Regression-tree models of attention-deficit–hyperactivity disorder (ADHD). CHQ, Chinese Health Questionnaire; Family APGAR, Family Adaptation, Partnership, Growth, Affection, and Resolve.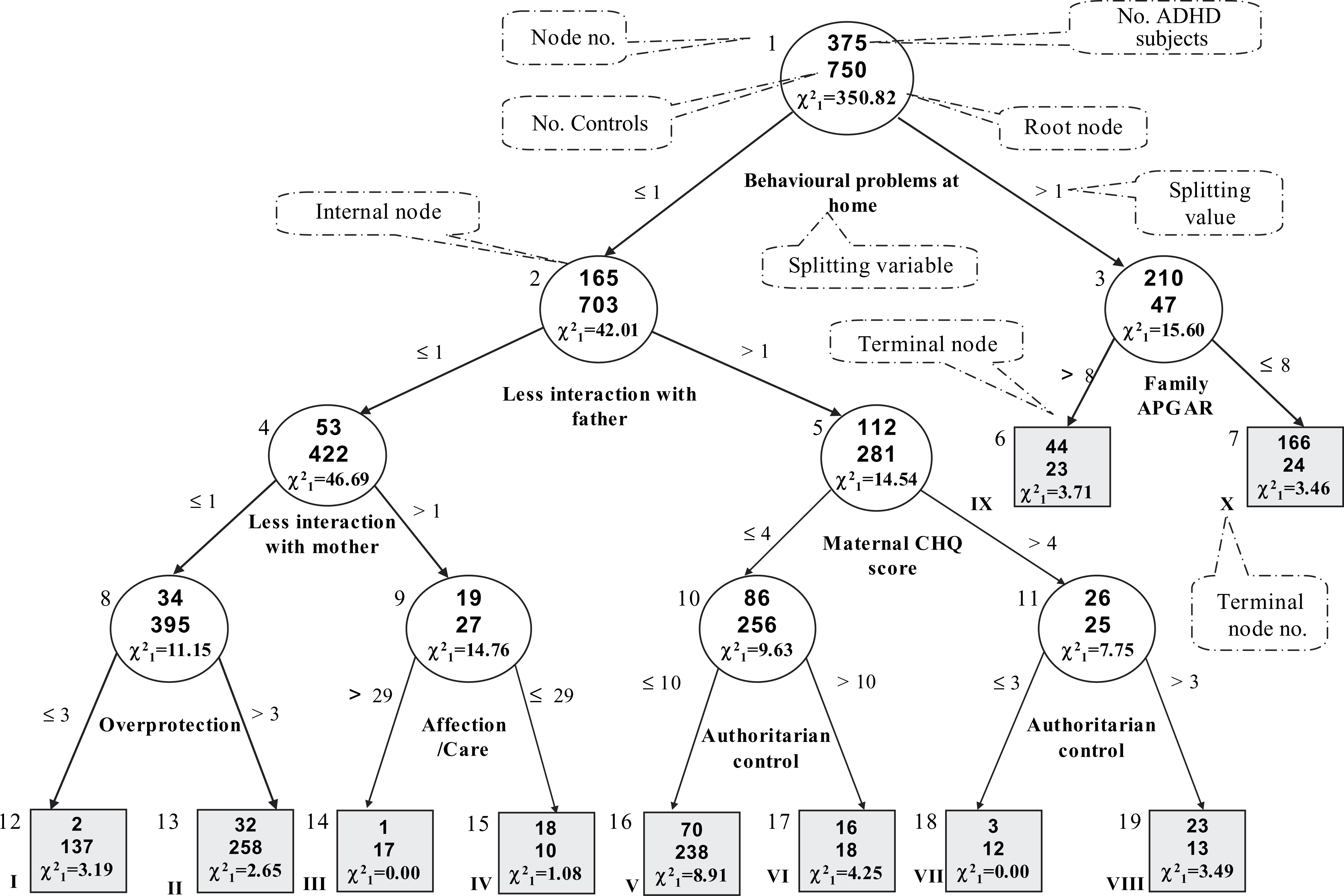
Association between ADHD and splitting variable at each node
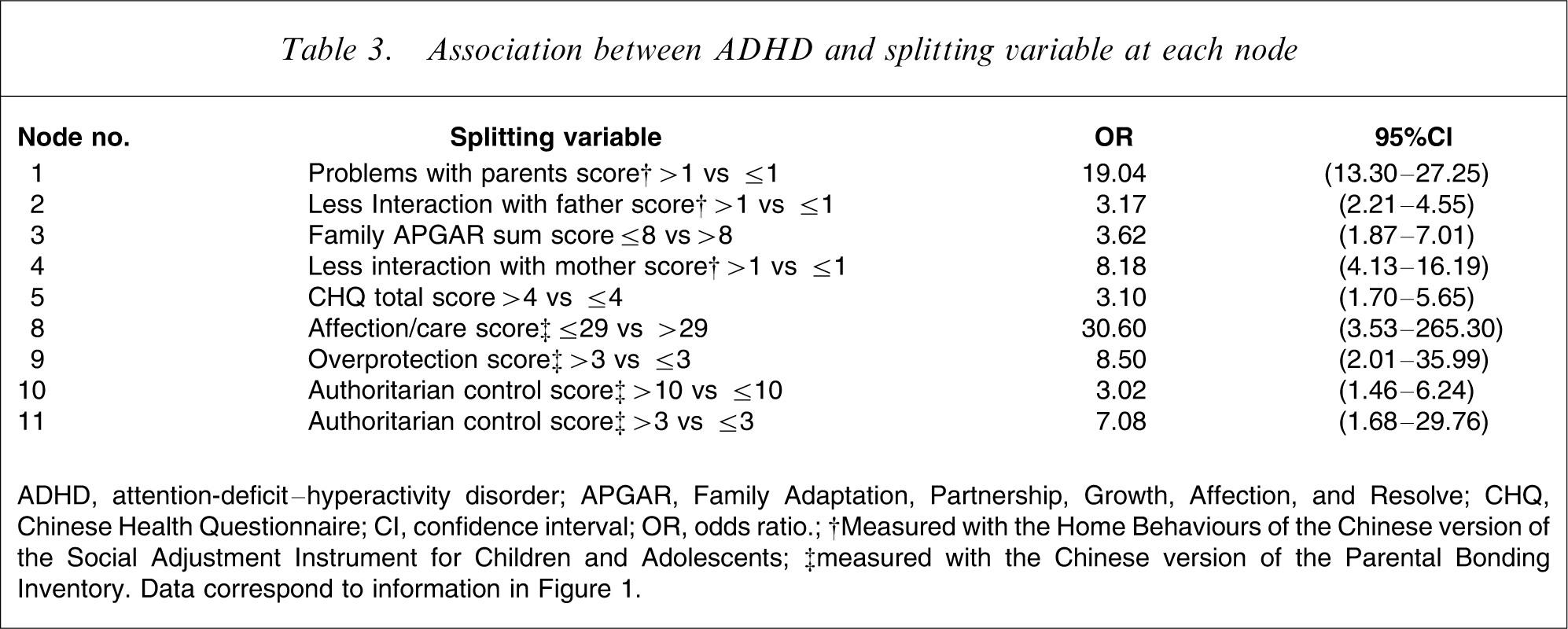
ADHD, attention-deficit–hyperactivity disorder; APGAR, Family Adaptation, Partnership, Growth, Affection, and Resolve; CHQ, Chinese Health Questionnaire; CI, confidence interval; OR, odds ratio.
†Measured with the Home Behaviours of the Chinese version of the Social Adjustment Instrument for Children and Adolescents; ‡measured with the Chinese version of the Parental Bonding Inventory.
Data correspond to information in Figure 1.
Figure 1 shows that ‘behavioural problems at home’ was used to split the entire sample (the root node). Four pathways favour ADHD, as shown by the most significant terminal nodes (i.e., IV, VIII, IX, and X). One pathway comprised more problems at home with perception of less (NODE X) or more (NODE IX) family support measured by the Family APGAR. The other two pathways, given less severe behavioural problems at home were: one comprising less interaction with father, greater maternal distress, and greater maternal authoritarian control (Node VIII); and the other, given more interaction with father, less interaction with mother and less affectionate/caring parenting from mothers (Node IV). In short, the leading familial variables to distinguish the ADHD group from the control group included child's behavioural problems at home and less active interaction with his/her father, and decreased maternal perceived family support.
Discussion
The major findings of the present study are that many more boys than girls with ADHD were identified in clinical settings; and mothers of children with ADHD in Taiwan tended to report anxious/depressive symptoms, to have less affectionate and probably more controlling/ overprotective parenting styles, to perceive less family support from their family, and to report that their children interacted less with them and the fathers and had more severe behavioural problems at home. The increased inappropriate parenting, parent–child conflicts, and inadequate parental support cannot be explained by maternal psychological distress. Both the parametric (multivariate logistic regression model) and non-parametric (tree-based regression model) approaches identified decreased interaction with parents, behavioural problems at home, and low maternal perceived family support as the most associated parental/family variables to distinguish children with ADHD from school controls. These results strongly support the notion that the overrepresentation of boys in clinical subjects with ADHD and the relationship between ADHD and parental/family dysfunction not only exists in Western countries, but also in Taiwan, which is substantially influenced by traditional Confucian principles that emphasize parental authority and children's obedience and academic achievement [45].
In Chinese families, mothers play the leading role in child-rearing and are responsible for children's academic performance [27, 28]. In addition, good school grades and diplomas have been emphasized in a way that children are expected to bring honour to the family by getting good grades and entering a good senior high school and college [27, 28]. In such situation, having a child with ADHD brings even greater pressure to Chinese parents, particularly the mothers. Also, mothers of children with ADHD may be blamed for their children's behavioural problems and academic underachievement [26, 27]. Although a lack of psychiatric diagnoses for mothers limits our ability to examine whether mothers of children with ADHD are more likely to suffer from mental disorders such as ADHD, anxiety disorders, and major depression [17, 18], we found increased symptoms of anxiety, depression, somatic complaints, and sleep problems in mothers of children with ADHD. The present study demonstrates similar findings to Western studies [14, 16] that mothers of children with ADHD were more likely to suffer from psychological distress.
The results of the present study lend evidence to support the notion that families of children with ADHD are more likely to have inappropriate parenting strategies [15], impaired family relationship [9], and increased parent–child conflicts [11]. Moreover, like others, the present study also suggests that low parental care and high parental overprotection may be associated with ADHD [46–48], and negative parent–child relationships are more prevalent in families of children with ADHD than in control families (reviewed by Johnston and Mash) [19]. We assume that persistent ADHD symptoms may be attributable to maternal psychological distress, inappropriate parenting styles, and problems in parent–child interactions [16].
Similar to the findings of previous studies that parenting stress and inappropriate parenting and parent–child interactions are related not only to children's behavioural problems but also to maternal psychopathology, such as depressive symptoms [13, 25, 49], our findings showed that maternal psychological distress was low to moderately correlated (Pearson correlation) to decreased perceived family support (–0.35), problems with parents at home (0.33), and less interaction with mothers (0.18) and fathers (0.25). Surprisingly, maternal psychological distress was not correlated with their parenting styles (0.04–0.07). This may imply that parenting styles are more like a characteristic or trait, in which mothers demonstrate their attitudes toward their children with little influence from their current psychological status. This assumption should be investigated in future studies. In contrast to previous studies showing that parental emotional distress may bias their reports on parental and child problems [50], maternal psychological distress cannot explain our findings of increased inappropriate parenting, inadequate family support, impaired parent–child relationships, and the more severe behavioural problems at home of methylphenidate-treated children with ADHD. Therefore, the finding of increased parental/family dysfunction in families of children with ADHD is convincing in our Taiwanese sample.
Limitations
Several methodological limitations should be considered while interpreting our results. First, the cross-sectional study design limits the inferences that can be drawn about causal relationships on ADHD and parental/family measures as addressed by other studies [46, 51]. However, longitudinal studies have provided evidence of a bi-directional association between negative parenting and persistence of behavioural problems among children with ADHD [24, 52, 53]. Second, lack of psychiatric interviews in the school controls limited the ability to ensure that the controls were free from ADHD; but the likelihood of ADHD among controls was thought to be very low because of the screening procedure. Third, because the controls were not recruited from the clinically referred sample as the cases, the findings of group differences in parental/family process may have been related to referral rather than to ADHD. For example, the present study may have over-sampled clinical subjects who had more severe behavioural problems or whose parents were distressed by their ADHD symptoms; and the finding of the parental/family difference possibly can be found with any child psychiatric disorder. The potential sampling bias should be considered when we interpret the findings. Fourth, the present study did not examine the effect of ADHD subtypes and other comorbid conditions. Because previous studies have shown that ADHD subtypes [10, 20] and oppositional defiant symptoms [15] do not influence the severity of parental distress and coping related to ADHD, the lack of examination of the effect of subtypes and comorbid conditions of ADHD on parental/family measures in the present study is justified. Fifth, the finding of higher parental education in the case group suggests that the ADHD patients who visit the medical center or their parents who agreed to participate in the present study may be more educated than the general population. Because parental educational level was not used to match the selection of controls, the influence of this unequal distribution was adjusted for by controlling for parental education in all the analyses. Last, the mothers were the only informants in the present study and may not accurately report the nature of the child relationship with the father. Moreover, maternal psychological distress may have biased their reports on parenting/family measures [50]; therefore, it was controlled for in the statistical models to minimize its potential confounding effect.
Counteracting the limitations, several major features of the current study constitute improvements over previous research on this topic. In addition to the clinical samples from a medical center, subjects with ADHD were recruited from several community psychiatric clinics through the ADHD Educational Foundation in Taiwan, thereby increasing the representative nature of the sample of patients with ADHD. The controls were recruited from a representative school-based sample with a very high response rate. Moreover, the sample size of the present study was large compared to those of similar studies. Last, four Chinese versions of the cross-culturally valid instruments were used to assess different aspects of parental/family domains.
Clinical implications
The present finding shows that medicated children with ADHD still significantly encounter more impaired parental/family function in Taiwan, suggesting that stimulant medication alone may not be enough in managing behavioural problems and improving parental processes. Because stimulants have been reported to be effective in improving negative parental practice and parent–child interaction [54–56], assessment of medication adherence and optimal dose of medication should be emphasized in clinical practice. Although some studies failed to prove the effectiveness of psychosocial or parenting training on the improvement of positive [54–56] or negative parental practice [54, 55] or family distress [56], there is some evidence supporting the idea that behavioural/parental intervention produces beneficial changes in negative parental practice [56, 57] and parent–child interaction [54, 58]. Hence, the combination of medication with good drug adherence and behavioural/parental intervention should be the optimal treatment strategy for ADHD in terms of improvement in maternal distress, parental practice, and child behavioural problems, particularly in the ethnic Chinese families.
Footnotes
Acknowledgements
This work was supported by grants from the National Science Council (NSC91-2314-B-002-223, NSC 93-3112-H-002-005), Taiwan. The preparation of this manuscript was supported by a grant from National Health Research Institute (NHRI-EX94-9407PC), Taiwan The author would like to thank all the participants and their teachers and parents for their contribution.