
Abstract
Tobacco smoking remains a neglected issue within general psychiatry despite high rates of associated morbidity and mortality. While there has been a coordinated community campaign to reduce tobacco smoking within the general population, mental health facilities have been reluctant to adopt such regulatory controls, and rarely target smoking prevention or treatment. This paper summarizes and discusses evidence relating to the clinical impact of tobacco smoking within inpatient psychiatric settings. A selective review of psychiatric and psychological research on smoking within inpatient settings was conducted, with a particular focus on the influence of smoking on the physical and mental health, pharmacotherapy, and social interactions of patients during their inpatient stay. Patients frequently alter their smoking habits during inpatient treatment, which can affect both their presentation and pharmacotherapeutic management. Smoking also appears to play a central role in social interactions on the ward, with staff frequently using cigarettes to reinforce certain behaviours. Despite current guidelines, mental health professionals rarely address nicotine use among their patients. Nevertheless, programmes that assist patients to quit during an inpatient stay have been shown to be both efficacious and cost-effective. Strategies that address staff concerns and assist in the implementation of effective smoking bans on psychiatric units are also available. Cessation should be a key component of inpatient treatment planning because this setting provides a safe and timely opportunity to help patients quit. A flowchart of interventions that could be incorporated within standard inpatient settings is proposed.
Tobacco smoking is the leading cause of preventable morbidity and mortality in Australia, killing more than 19 000 people each year [1]. Despite a decrease in smoking prevalence within the general population [2], smoking rates among mental health populations remain high. Indeed, smoking rates among psychiatric patients tend to be two- to threefold higher than the general population [3], and range from approximately 40–50% in patients with depressive and anxiety disorders to 70–90% in patients with chronic schizophrenia [4]. Acknowledgement of the deleterious consequences of tobacco smoking, including the negative effects of passive smoking, has resulted in the introduction of tighter regulatory controls, both locally and internationally, as well as the introduction of smoke-free public places. Hospitals and health-care areas have adopted or are moving towards a smoke-free policy, prohibiting smoking except in designated areas [2]. However, mental health facilities seem to be lagging behind with such policies and cigarette smoking among psychiatric patients remains generally a neglected issue.
Although an admission to a psychiatric ward could be seen as a key opportunity to intervene [5], smoking is typically not a focus of treatment within that setting, despite a high proportion (42–97%) of patients reporting being interested in quitting at some time in the future [6–9]. In the present paper we will use a biopsychosocial perspective to critique current clinical practice based upon a selective review of the smoking literature, and recommend interventions that could be incorporated within standard inpatient care.
Smoking in the inpatient unit
Biological aspects
More than 4000 chemical compounds are known to exist in tobacco smoke [10], of which 43 are thought to be human carcinogens [11]. It is therefore not surprising that for schizophrenia, most of the excess mortality (excluding suicides and accidents) relates to cigarette smoking [12]. Indeed, for lung cancer alone, the mortality ratio is twice that found in the general population. As a group, individuals with major mental disorders die at a relatively younger age, mainly from illnesses for which smoking is a major risk factor (e.g. heart disease, cancer, cerebrovascular and respiratory diseases) [13].
Nicotine, the main addictive component of tobacco, reaches the brain 10 s after inhalation, and stimulates dopamine release within the nucleus accumbens [14], most likely through activation of nicotinic acetylcholine receptors [15]. Interestingly, altered expression and function of brain α7 nicotinic receptors has been implicated in information-processing deficits in schizophrenia [16]. Because a high concentration of nicotine is necessary to activate the altered receptor, it has been postulated that heavy smoking in patients with schizophrenia may be an attempt to correct the receptor deficit and improve cognition [17]. Nicotinic receptors also modulate other major neurotransmitters, such as serotonin, noradrenalin, γ-aminoburtric acid (GABA) and glutamate [18], which may help explain its high level of use in psychiatric disorders in general. Inhibition of monoamine oxidase B by cigarette smoke has been suggested to be one mechanism by which smoking may exert an antidepressant-like effect [18, 19].
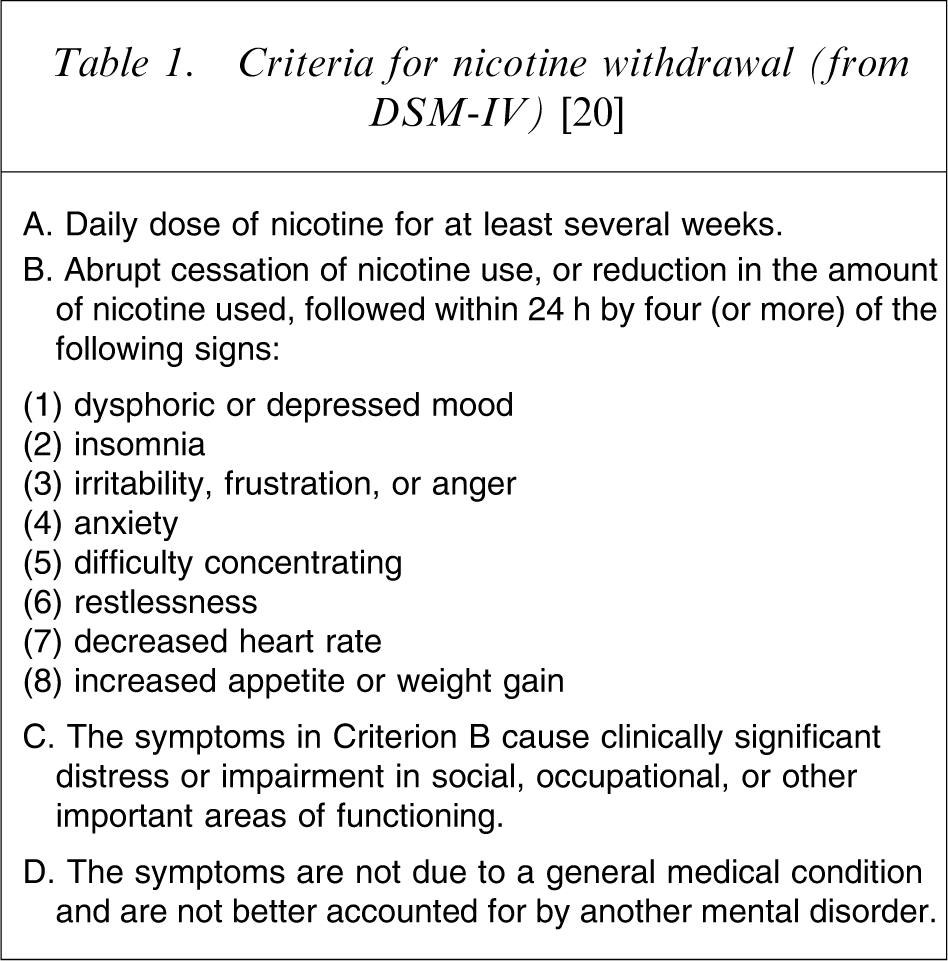
For patients who are dependent on nicotine, it is important to recognize symptoms of nicotine withdrawal on the inpatient unit, given that patients will often be admitted in a chaotic state without cigarettes or money, and will sometimes not smoke for the first few hours or days of admission. Nicotine withdrawal symptoms (Table 1) usually occur within the first 12–24 h of smoking cessation, and may be confused with a range of psychiatric symptoms and disorders, including alcohol or drug withdrawal, affective disorders, sleep disorders, neuroleptic-induced akathisia and exacerbation of the negative and positive symptoms of schizophrenia [3].
Criteria for nicotine withdrawal (from DSM-IV) [20]
One clinically important factor to consider is that hydrocarbon agents within tobacco smoke increase the metabolism of numerous psychotropic drugs through induction of the liver cytochrome P450 1A2 isoform [21]. Indeed, its activity has been shown to be 1.72-fold higher in heavy smokers than in non-smokers [22]. This means that blood levels of numerous psychotropic medications (Table 2) can significantly change if patients alter their smoking habits on the ward or following discharge (for comprehensive review see [21]). For example, the difference between the mean daily dose of clozapine needed by smokers and non-smokers to reach a given blood concentration has been reported to be 50% [23]. For benzodiazepines, diminished end-organ responsiveness following cigarette smoking may also play a role in the attenuated sedation observed in smokers compared to non-smokers [24].
Psychotropic medications with smoking-induced metabolism
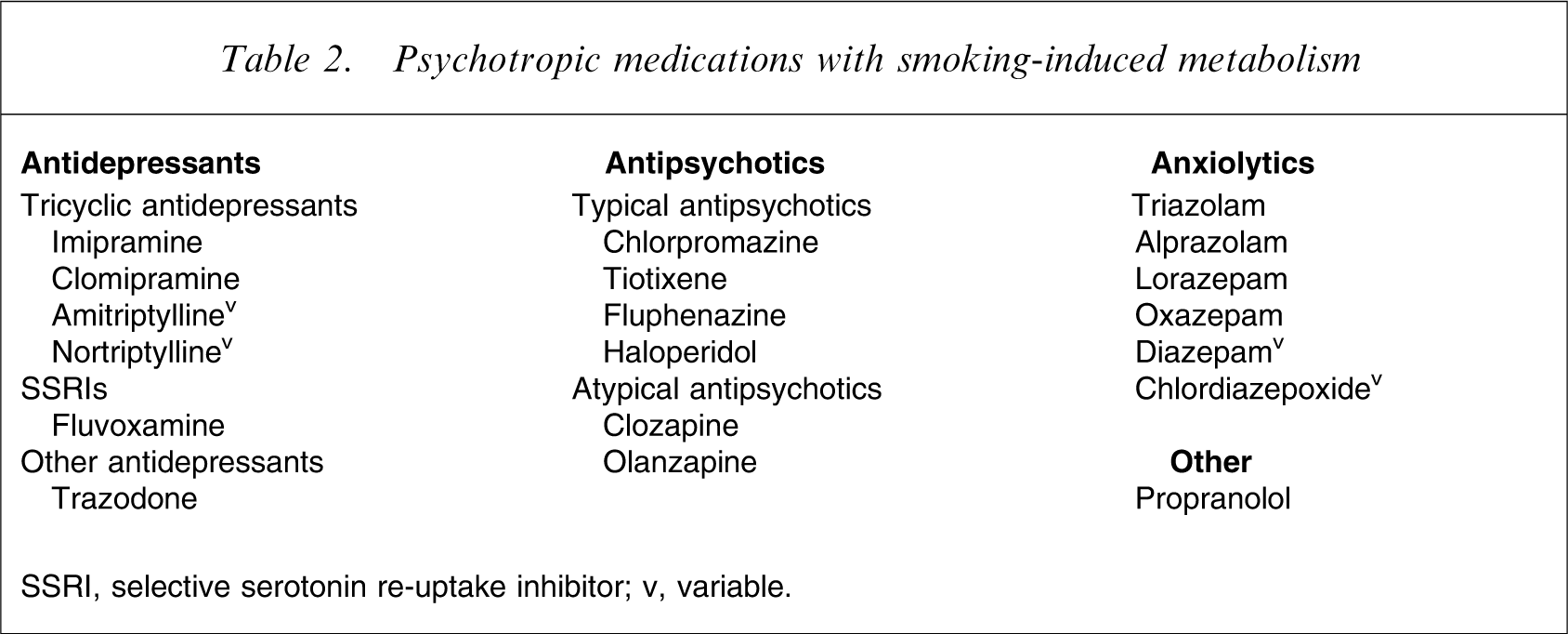
SSRI, selective serotonin re-uptake inhibitor; v, variable.
Numerous case reports have described adverse reactions caused by elevated concentrations of clozapine or olanzapine after smoking cessation [25, 26]. One study that assessed the time course of CYP1A2 activity changes after smoking cessation in heavy smokers suggested that doses of substrates of those enzymes with a narrow therapeutic range (e.g. clozapine) should be decreased immediately on cessation of heavy smoking (≥20 cigarettes/day) [27]. As a rule of thumb, the authors recommended a stepwise daily dose reduction of approximately 10% until the fourth day after smoking cessation, accompanied by therapeutic drug monitoring, to account for individual variation.
Psychosocial aspects
While tobacco use appears to be higher among patients with mental health problems [28, 29], the underlying biological and psychological factors that drive this association are far from clear. For patients with schizophrenia, many explanations have been proposed, including self-medication in order to alleviate the cognitive [17] or negative [30] symptoms of the illness or the side-effects associated with medication [31], to reduce boredom or social inhibitions [32], or because of the differential effects of nicotine on disordered reward pathways [33]. Nicotine-induced improvement in cognition, transient mood elevation [18] and its potential anxiolytic effects support the notion of self-medication in both depressive and anxiety disorders [34, 35]. However, longitudinal studies have also demonstrated that smoking can increase the risk of subsequent panic attacks/disorder [35]. In bipolar disorder, smoking has been associated with illness severity and the occurrence of psychosis [32, 36].
Cigarette use has traditionally occupied a very important role on psychiatric wards. On an inpatient unit in the USA, up to 80% of patients’ interactions were found to be centered on smoking [37]. Historically, cigarettes have often been used as a token economy, with smoking privileges utilized as reinforcers for medication compliance and control of assaultative behaviours [6, 38]. But those privileges can also represent a potential cause of violence, especially if cigarettes are requested outside designated times. Indeed, one study found that patients were frequently told to wait for cigarettes, with staff responding only when a patient's behaviour appeared to escalate or when the patient was threatening to act out [6], therefore providing a positive reinforcer for such behaviours.
It also appears that if a non-smoking patient is admitted to a psychiatric ward where smoking is allowed, he/she is at risk of leaving the inpatient unit as a smoker because of peer pressure to smoke, the lack of other ward activities and reinforcement by the institution [6]. Indeed, a recent study has shown that 3 days after psychiatric admission, 74% of heavy smokers had decreased their consumption, but 80% of light and 57% of moderate smokers had increased their consumption [39].
It is important to note that admission to a smoke-free ward is tolerated by the vast majority of psychiatric patients who smoke, particularly if nicotine replacement therapy (NRT) is available [5]. However, most return to smoking within 5 weeks of hospital discharge [5], suggesting that inpatient settings provide a potential site for initiating smoking cessation programmes, but greater support is needed to support patients following discharge.
Although in terms of lives saved, quality of life, and cost efficacy, treating smoking is considered to be one of the most important activities a clinician can undertake [29], psychiatrists seldom discuss the issue with their patients [40] and only very rarely is the diagnosis of nicotine dependence recorded in patients’ notes. In addition, patients are rarely advised to quit smoking, referred to smoking cessation counselling or provided with NRT on discharge [5, 29]. This may be explained by mental health workers’ concerns about taking away a patient's only pleasure, as well as hindering their recovery by preventing them from using what is thought to be a way to decrease stress and to relax [41–43]. Yet, psychiatric patients’ motivation to quit smoking has been found to be similar to that of the general population [44, 45], including within inpatient [5] and long-term care settings [48]. Indeed, a positive attitude towards quitting is also encountered within drug and alcohol treatment settings [9], where an inpatient stay is considered an opportune time to provide smoking-cessation interventions [47, 48].
However, interviews with inpatient nursing staff raise concerns that restricting patients’ smoking would be like enforcing a double dose of suffering, by adding nicotine withdrawal symptoms to their illness [6]. Staff also report using cigarettes to improve safety in the work environment, by offering them to de-escalate aggressive behaviours in patients. Some patients report that their most comforting time in hospital was when their nurse was spending time with them smoking [6]. Studies comparing the prevalence of smoking in psychiatric nurses with nurses of other specialties are contradictory, finding both higher and lower rates [49, 50]. Nurses who smoke are significantly more likely than nurses who do not smoke to state that staff should be allowed to, and that it may be therapeutic to smoke with patients [51]. They are also less in favour of encouraging patients to stop smoking. Psychiatric staff do not tend to see it as their job to help people stop smoking [52], suggesting that there is a need for a substantial shift in staff attitudes.
Interventions
The American Psychiatric Association recommends that psychiatrists assess the smoking status of all patients, including their readiness to quit, their level of nicotine dependence, and their previous quitting history [53]. It also suggests that an inpatient stay may be an opportune time for initiating treatment for nicotine dependence because of the intensity of exposure to medical staff, diagnosis of comorbid medical conditions, and being removed from usual smoking cues (Figure 1).
Flowchart of interventions for smoking on the inpatient unit. IPU, inpatient unit; NRT, nicotine replacement therapy.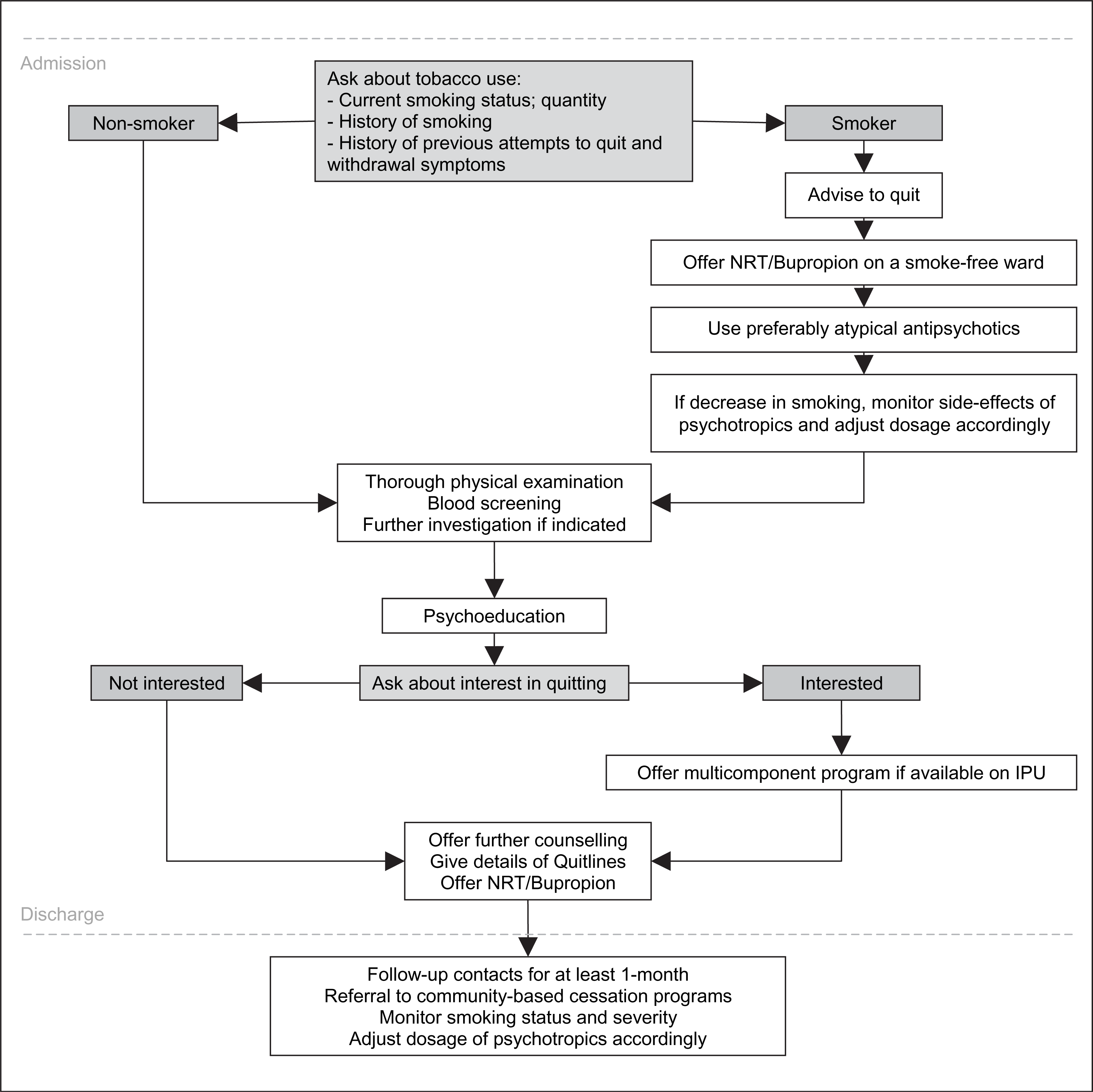
Biological interventions
Given the high morbidity associated with smoking, an inpatient admission is an excellent opportunity to screen for physical illnesses, with a low threshold for further investigations, such as a chest X-ray, if clinically indicated.
Prophylactic NRT is recommended because it not only alleviates withdrawal symptoms and decreases smoking [53], but also reduces the rate of discharges against medical advice on smoke-free psychiatric inpatient settings [29]. NRT formulations available in Australia and New Zealand include patches, gum, lozenges and the oral inhaler. Although all are effective in alleviating withdrawal symptoms [54], the transdermal patch requires only once-daily administration, which can increase compliance [3], especially for those patients on the ward who are too disorganized to ask regularly for other NRT formulations. It also delivers a fixed dose of nicotine continuously [55], producing a blood nicotine level closer to patients’ usual daily nicotine intake [5], although usually only half that obtained through smoking [56]. It is commenced on the first morning of smoking cessation with either a 21 mg 24 h patch or a 15 mg 16 h patch [53], and can therefore be offered by staff on a daily basis with other morning medications. For patients who also continue to occasionally smoke cigarettes, there does not appear to be significant risks associated with concurrent administration of patches [53].
However, highly nicotine-dependent patients may prefer to use more than one form of NRT [29] and it appears safe and possibly more effective to use gum [57] or an inhaler [58] in combination with a patch. A 2 mg gum can be offered either regularly or on an as-needed basis in those already using a patch, while inhalers may be puffed on continuously during the day. The 2 mg and 4 mg lozenges deliver approximately 25% more nicotine than the equivalent dose of nicotine gum [59], and are recommended to be used every 1–2 h during the first weeks of treatment [53]. Given that patients with serious mental illnesses appear to make appropriate use of NRT devices [60], and that gum, lozenges and inhalers do not increase fire risk, we believe that more responsibility could be given to most patients in managing their smoking cessation.
While more placebo-controlled trials are needed to assess the efficacy of NRT within populations of smokers with co-occuring psychiatric disorders, studies with patients suffering from schizophrenia offer preliminary evidence that patches are both well-tolerated and effective in smoking cessation, especially over the short term (<6 months) [60, 61]. Bupropion has also proved to be efficient in decreasing withdrawal symptoms and in helping patients quit smoking [62]. Bupropion and NRT can be used concomitantly, but the evidence for additional benefits of using both together remains unclear [63]. Atypical antipsychotics, especially clozapine, also appear to have a positive effect on smoking cessation, compared with typical antipsychotics, in patients with schizophrenia [31, 61].
Psychological interventions
All patients should receive psychoeducation about the constituents of cigarettes, the long-term risks, the interaction with psychotropic medications, and the features of nicotine dependence.
Cognitive behavioural therapy (CBT) should also be provided as part of a multicomponent programme to help patients stop smoking [4]. It should be comprehensive and delivered by a clinician employed and trained for the task, rather than a staff member who is trying to fit it into their other duties [64]. Some have suggested that a proportion of the time used by staff to provide cigarettes (up to 4 h a day) should be shifted to the delivery of cessation counselling services [5]. In general medicine, such multicomponent programmes initiated during hospital stays have been shown to be efficacious, cost-effective [65] and feasible within a wide range of hospital settings [65, 66]. The support of hospital management appears to be critical for success.
In psychiatry such data are lacking, but a recent randomized controlled trial of individually administered motivational interviewing and CBT plus NRT has shown promising results regarding smoking cessation in an outpatient sample of individuals suffering with psychotic disorders [67]. A few group programmes using CBT and motivational enhancement techniques have been developed and adapted for individuals with mental illnesses [4, 60, 68]. However, to our knowledge, none has been studied within inpatient settings. Nevertheless, we recommend that targeted action-oriented strategies should be offered to those patients interested in quitting during their inpatient stay.
A systematic review of inpatient interventions within medical settings has found that quit rates are higher if individuals are followed up for at least 1 month after discharge [65]. We would therefore suggest that inpatient programmes include outpatient face-to-face or phone call follow-up contacts for at least 1 month after discharge, or referral to community-based cessation programmes that are able to offer ongoing counselling, support and subsidized nicotine replacement [69]. Such recommendations should be included within the patient's discharge plan, so that outpatient services or their GP can offer support and prescribe further NRT if required. We also recommend that all smokers are given details of specific Quitline programmes, which provide inexpensive, proactive and targeted interventions for patients with mental illness, in accordance with current clinical guidelines [2].
Social and cultural interventions
Staff, as well as patients, should receive psychoeducation about the reasons for a smoking ban within psychiatric units, so that they do not perceive it as punitive or as a way to increase control. While many potential difficulties have been highlighted with the implementation of such bans, two recent reviews have demonstrated that more problems were anticipated than actually encountered [69, 70]. Despite a few case reports [71, 72], overall there appear to be no increases in aggression, use of seclusion, discharge against medical advice or use of as-required medications, especially where bans were total and not partial (e.g. indoor ban only).
Reports of an increased risk of relapse following smoking cessation in patients with a history of depression [73] raises important issues regarding the effect of a total ban on this population, but it is not clear whether this relates to the biological effects of nicotine withdrawal or the associated psychological stress [74]. Nevertheless, close monitoring is certainly warranted, particularly following discharge, and use of NRT could be especially important in such patients. Conversely, recent research suggests that clinicians should not be discouraged from helping patients with schizophrenia stop smoking for fear of worsening symptoms [31, 60, 61].
Given the many preconceived notions about the value of smoking among psychiatric patients, considerable resistance is likely to emerge from staff when proposing to implement such bans. Lawn and Pols have outlined a number of measures that require consideration when introducing effective smoking bans, many of which relate to staff [69]. Educational programmes that help staff to distinguish nicotine withdrawal symptoms from other psychopathology are vital, and outcomes appear better when staff view the ban as an opportunity to develop new clinical skills. Collaboration across specialties and consistency of approach is also important for success. A preparation period is recommended, in order to advertise the impending change and to provide education to staff as well as associated community agencies. Interestingly, the level of patient and staff support for such policies appears higher after the bans have been implemented than before, especially when the bans are total [69, 70].
Ethical considerations are particularly relevant to the issue of smoking bans. Given the serious risks that smoking represents for patients’ long-term health [11], we believe that health-care facilities should certainly not encourage smoking, such as providing or selling cigarettes to patients admitted onto the ward. Rather, they should encourage and support patients in quitting, especially if they are motivated. However, when patients are detained in hospital against their will or are living in long-term facilities that may be considered their home, the issue of forced abstinence becomes more important [75]. In these circumstances, it has been argued that beneficence is not adequate to justify placing restrictions on patients’ autonomy and liberty to smoke [75].
Nevertheless, hospitals have a duty to protect non-smoking patients and staff from the effects of passive smoking [11]. While many facilities will allow patients to smoke only in open-air areas or in special rooms, supporters of total bans highlight the importance of promoting a healthy lifestyle and reducing any potential fire hazard [76]. In addition, a number of studies have found that selective bans tend to cause more disruption than imposing a total ban, due to their frequent fragmentation and inconsistent application [69, 71]. Although more research is clearly warranted, especially in terms of implementation strategies, introducing smoke-free wards is an important step in addressing the high rates of smoking among mental health populations.
Conclusion
The current literature suggests that an inpatient stay on a smoke-free unit provides a safe and potentially efficacious opportunity to either initiate an attempt to quit, or at least to provide information to help patients move towards this. Smoking cessation should be a common component of an inpatient treatment plan, and a combination of NRT and structured behavioural support should be offered during admission and after discharge. Greater efforts also need to be made to develop effective strategies to assist smokers with mental illness to quit.