
Abstract
In many countries the process of deinstitutionalization has led to the replacement of mental hospitals with community services and general hospital psychiatric units (GHPUs). Yet, acute psychiatric inpatient care still represents a core problem for policymakers, professionals, and for patients themselves, because standards frequently fail to meet their needs and expectations [1–3].
In Italy a 1978 reform law initiated the transition from psychiatric care delivered in large asylums to a community-based system of care, including outpatient services, long-term residential facilities, and GHPUs with no more than 15 beds [4]. Yet, as in other countries, the organization, functioning, and characteristics of inpatient facilities have to date received very limited focus.
In an effort to provide detailed data on acute inpatient care, a national survey called PROGRES-Acute (PROGetto RESidenze, Residential Care Project for Acute patients) has recently been jointly launched by the Italian National Institute of Health and by the Department of Mental Health of Trieste.
The aims of this national survey were to obtain detailed information on the physical characteristics, activities, demographic and clinical characteristics of residents, staffing arrangements, regional provision of care, discharge rates, and admission rules for all Italian public and private inpatient facilities. The present paper focuses on the process of care in public inpatient facilities.
Methods
All 21 Italian regions were asked to participate in the study, and all complied with the exception of Sicily, for a total of 3928 beds in 301 public facilities. The surveyed regions also had 4862 beds in 54 private inpatient facilities, but private facility data were not included in the present analysis because these facilities present very different characteristics in terms of average size and patient casemix.
Assessment
Each region appointed a coordinator, who organized and supervised data collection. Information about the number and location of public inpatient facilities was obtained from regional Health Authorities, and later from the 203 NHS Departments of Mental Health located throughout the country. The project commenced in 2001, and data were collected throughout 2002–2003.
Survey data were collected by structured interview, adapted from the Facility Form used previously for a nationwide survey of non-hospital residential facilities in Italy [5]. Pilot testing was first conducted to test the validity and acceptability of the survey form (Facility Form). A letter describing the study (with an enclosed copy of the Facility Form) was then sent to each facility's head psychiatrist.
The Facility Form included a detailed section concerning the various types of treatment and intervention that each facility provided as well as patient management and facility rules. This section asked for information on biological treatments, psychotherapy and other forms of psychological treatment, rehabilitation, recreational activities, intervention on patient social networks, intervention aimed at involving other health services and agencies, and financial support for patients. The head psychiatrist was asked to indicate whether some form of each type of intervention had actually been provided on a regular basis for at least some of the facility's patients over the last 30 days. Rules during patient stay and limitations to their freedom were also surveyed, such as the possibility for patients to exit the facility while admitted, items banned to patients, and the presence of locked-door policy.
Study questions
In this paper, different combinations of intervention were examined: (i) individual psychotherapy (supportive, dynamic, or cognitive behavioural treatment, CBT); (ii) group psychotherapy (dynamic or CBT); (iii) CBT (individual or group); (iv) dynamic psychotherapy (individual or group); (v) family therapy (psychoeducational intervention or structured family therapy); (vi) structured rehabilitative intervention (individual or group rehabilitation); (vii) any form of rehabilitative intervention (structured individual, group, vocational training, training courses, discussion groups, expressive activity groups, and physical exercise groups); and (viii) any type of intervention on a patient's social network (activities targeted at increasing awareness and involvement for neighbours, friends, or colleagues or at integrating patients with local clubs and associations).
Associations between these groupings as well as facility internal rules and the following variables were investigated: (i) number of beds (it was suggested that a greater number of beds would be associated with both a higher number of different facility-available programmes (due to greater clinical casemix heterogeneity) and with more rules (due to a greater need to maintain more effective control over a greater number of inpatients); (ii) length of stay (predicted to be associated with the delivery of a greater number of programmes and with more rules); (iii) mean working hours per week for psychiatrists, psychologists, psychiatric nurses, rehabilitation therapists, and social workers per bed (presumed to be associated with more specific professional programmes and with fewer rules); and (iv) episodes of physical restraint over the last month per bed (chosen as a proxy of ward climate and hypothesized to be negatively associated with the number and variety of psychosocial programmes, and positively associated with more rules).
Finally, it was examined, using a multidimensional approach, whether relevant aspects of the therapeutic process (i.e. presence of any psychotherapeutic or of any rehabilitative intervention) or important ward rules (i.e. locked doors) were related to ward structure (i.e. number of beds and staff provision), patient outcome (i.e. length of stay), and ward social climate (i.e. episodes of physical restraints). Understanding these relationships was considered helpful to clarify processes of care underlying the adoption of specific therapeutic styles (and procedures), as well as to implement interventions more strictly targeted to patient needs.
Statistical analysis
The main analysis focused on descriptive statistics and was conducted separately in function of type of facility (GHPUs; university psychiatric clinics [UPCs], and 24 h community mental health centers [CMHCs]). Given that the sample presented fewer UPCs and CMHCs, data for the three facility types were grouped for some of the analyses.
Associations were tested with Mann–Whitney U-test because of skewed distributions of several of the studied variables. Differences in the proportions of internal rules adopted in the different settings were examined using χ2 tests.
To investigate the relationships between aspects of the therapeutic process or ward rules and ward structure, outcomes and ward social climate, multiple logistic regression models were constructed. For this purpose, number of beds, length of stay, staff provision and episodes of physical restraints were entered as independent variables, whereas the presence of any type of psychotherapy, any form of rehabilitative intervention, or locked-door policy were entered as dependent variables. With regard to the latter variable, 24 h CMHCs were excluded from the analyses because none of these facilities had locked doors. The independent continuous variable was divided into either three or two groups, based on percentile values, and a backward selection procedure was adopted. The results have been reported as odds ratio (OR) and related confidence interval (CI). All analyses were done with SPSS software, version 12 for Windows (SPSS Inc., Chicago, IL, USA).
Results
A total of 262 GHPUs were surveyed, with a total of 3431 beds and a mean of 13.1 beds each. Twenty-three UPCs, operating with 399 beds and a mean of 17.3 beds each, were also surveyed. There were also 16 24 h CMHCs, located in the Friuli-Venezia Giulia Region (n = 10) and in Campania (n = 6), with 98 beds and a mean of 6.1 beds each. Nearly all public inpatient facilities participated in the survey. There were only four refusals: three GHPUs and one UPC (all located in the Lombardy Region).
All but two GHPUs and only a few UPCs and 24 h CMHCs were legally able to admit compulsory inpatients. Average length of stay was 12.0±3.4 days for GHPUs, 18.5±7.1 days for UPCs, and 37.0±55.3 days for 24 h CMHCs.
Biological treatment
Pharmacotherapy was provided by all facilities. Electroconvulsive therapy and light therapy were very rarely delivered. Only one UPC reported using transcranial magnetic stimulation (Table 1).
Treatments and interventions provided by public acute inpatient facilities
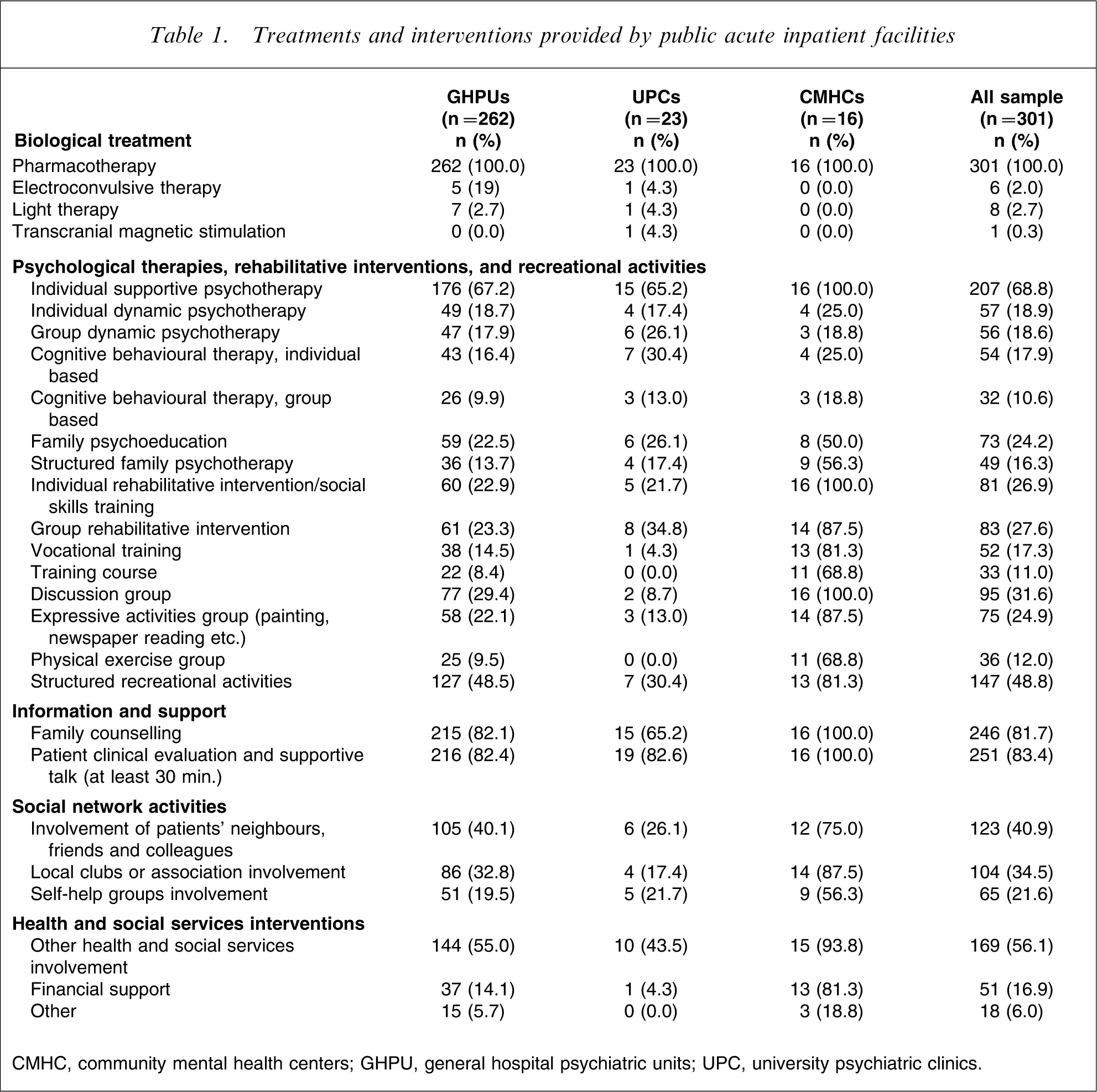
CMHC, community mental health centers; GHPU, general hospital psychiatric units; UPC, university psychiatric clinics.
Psychotherapy
Individual supportive psychotherapy was reported by approximately 70% of inpatient facilities. Family psychoeducation was provided by only one out of four facilities. Group or individual dynamic psychotherapy, individual CBT, and structured family psychotherapy were provided by approximately one out of six facilities. Provision of group CBT was rare (approximately one out of 10 facilities).
Overall, individual psychotherapy (either supportive, dynamic, or CBT) was delivered by fewer than three out of four facilities. It was used more frequently, however, than group psychotherapy (dynamic or CBT), which only one out of four facilities provided.
Individual- or group-based dynamic or CBT psychotherapies had a similar distribution (approx. one out of four facilities). Family-based intervention, including psychoeducation and structured family therapy, were not widely available (approx. one in three facilities). More than 20% of the facilities surveyed provided no individual-, group-, or family psychotherapy.
Rehabilitation and other supportive activities
Discussion groups were held in one out of three facilities. Structured rehabilitative intervention, in individual or group format, and expressive activity groups were conducted in one-quarter of inpatient facilities. Vocational training programmes were less common, and physical exercise groups were rarely available (approx. one out of 10 facilities). Approximately half of the facilities provided no form of rehabilitative intervention.
Most facilities (83%) reported performing regular clinical inpatient evaluations and at least 30 min-long supportive psychotherapy sessions on a regular basis. Counselling aimed at providing patients with information on their disorders and available treatment were implemented on a large scale (80%).
Recreational and social network activities
Structured recreational activities, such as playing chess or cards, were conducted in fewer than half of the facilities, although the remaining facilities offered less structured recreational activities.
Two out of five facilities conducted activities targeted at fostering the involvement of patients’ neighbours, friends, and colleagues, and one out of three provided activities aimed at integrating patients with local clubs or associations. Only a limited number of facilities (22%) promoted patient self-help groups.
Approximately half of the facility managers stated they were committed to involving other health and social services in patient treatment. Financial support for patients delivered during inpatient stay was infrequent (17%).
Rules regulating facility and patient management
In general, GHPUs adopted more rules, and CMHCs showed the least restrictive environment (Table 2). Rules most frequently concerned a ban on metal knives during mealtimes (χ2=7.24, df = 2, p = 0.03), on cutting objects (χ2=110.80, df = 2, p = 0.000), and on the personal possession of medication (χ2=11.11, df = 2, p = 0.004). Policy regulating patient exit from facilities was strikingly more restrictive for GHPUs than it was for UPCs and CMHCs. Last, entrance doors were locked in most GHPUs, in many UPCs, but not in CMHCs (χ2=52.19, df = 2, p = 0.000).
Rules adopted by public acute inpatient facilities
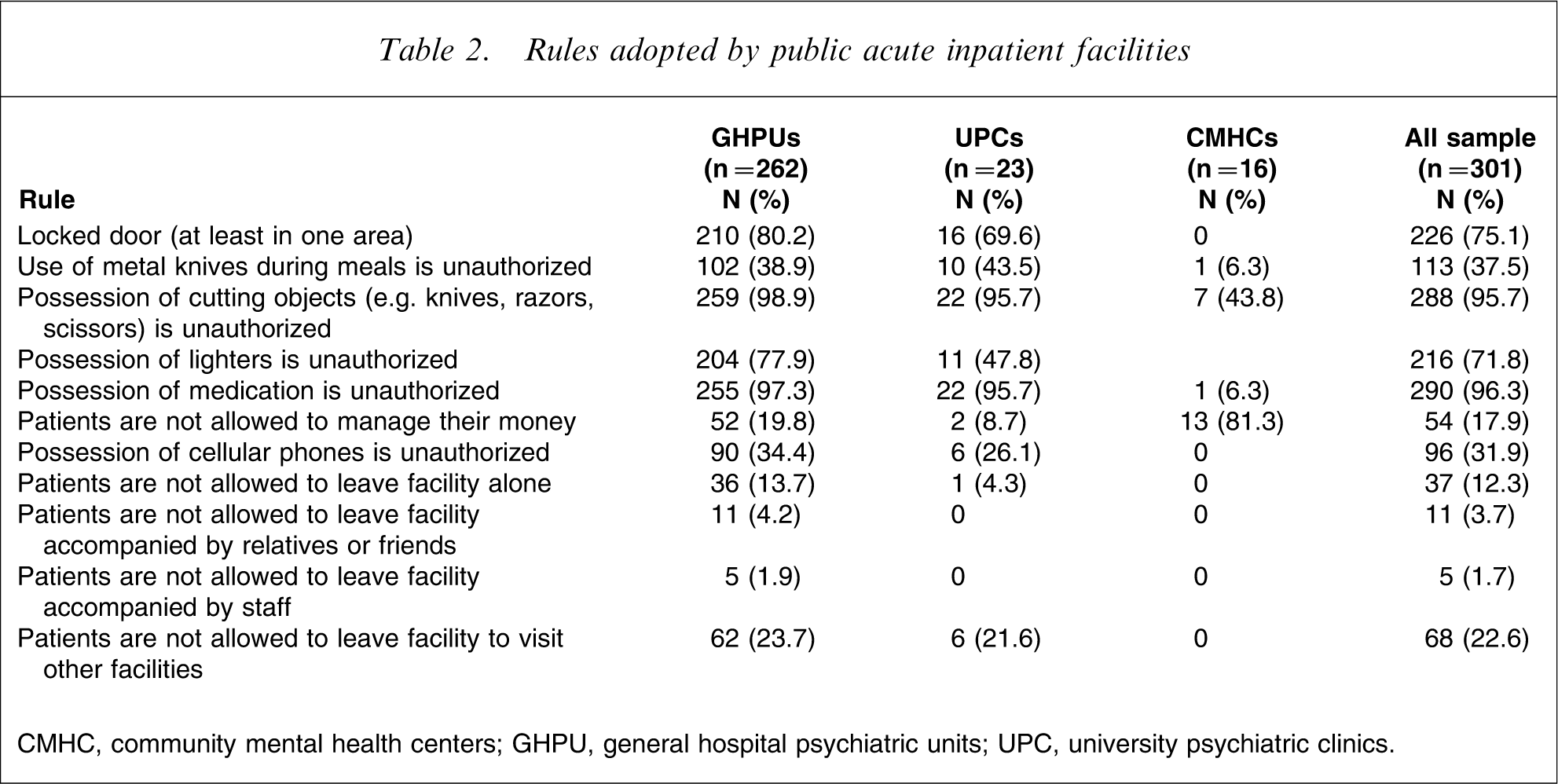
CMHC, community mental health centers; GHPU, general hospital psychiatric units; UPC, university psychiatric clinics.
Variables associated with specific types of treatment or intervention
Presence of rules was mostly associated with a higher number of beds and shorter length of stay. A lower provision of psychiatrists and nurses’ hours was associated with a locked-door policy. A lower number of episodes of physical restraint was associated with the provision of individual psychotherapy or CBT. A higher number of rules was associated with more episodes of restraint. Higher presences of various staff members, was associated with a greater availability of different types of therapy or intervention (this effect was more evident for psychologists), whereas presence and number of rules was generally associated with fewer staff working hours (mostly for psychiatrists and nurses; Table 3).
Association between specific treatments/interventions and rules, and selected variables
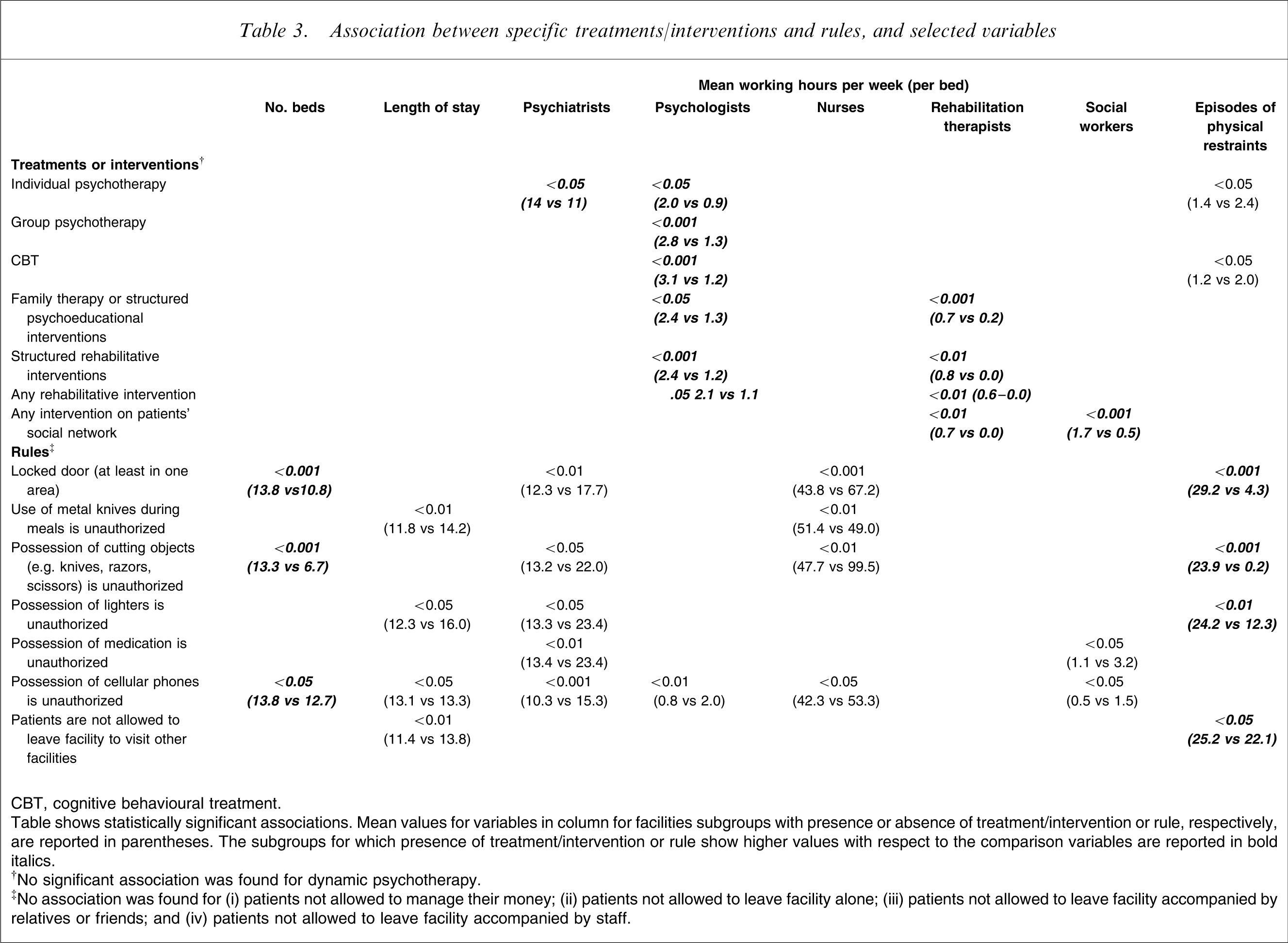
CBT, cognitive behavioural treatment.
Table shows statistically significant associations. Mean values for variables in column for facilities subgroups with presence or absence of treatment/intervention or rule, respectively, are reported in parentheses. The subgroups for which presence of treatment/intervention or rule show higher values with respect to the comparison variables are reported in bold italics.
‡No association was found for (i) patients not allowed to manage their money; (ii) patients not allowed to leave facility alone; (iii) patients not allowed to leave facility accompanied by relatives or friends; and (iv) patients not allowed to leave facility accompanied by staff.
A higher probability of delivering psychotherapy was associated with more numerous nurse provision, whereas rehabilitative programmes were more frequently available in facilities with both a longer length of stay and more psychologists (Table 4). The presence of locked doors was associated with more frequent episodes of physical restraint.
Variables associated with treatment and interventions: multiple logistic regression models
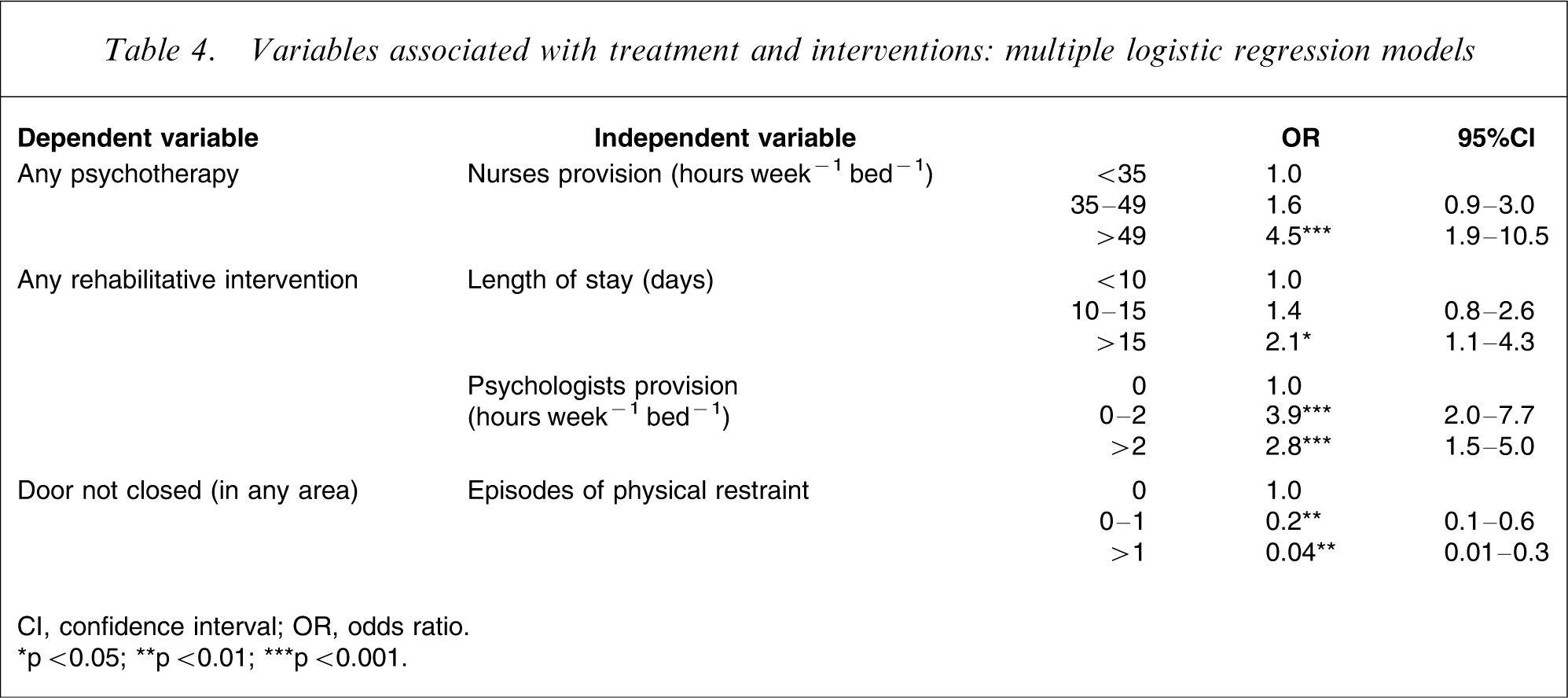
CI, confidence interval; OR, odds ratio.
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Discussion
The present study represents the first nationwide survey of acute inpatient facilities conducted in Italy. Previous studies did not go beyond the regional or local level nor had they provided substantial information on inpatient facilities and the process of care [6].
Primacy of pharmacotherapy versus integrated treatment
As expected, pharmacotherapy was the most commonly reported intervention. Surprisingly, more than 13% of facilities reported that they delivered no additional psychotherapeutic or rehabilitative intervention of any type.
Many official governmental reports have underscored the need for the provision of a wide range of psychosocial programmes in the acute management of psychiatric inpatients [1, 7]. Yet many forms of psychosocial intervention (e.g. cognitive behavioural and dynamic focused psychotherapies, patient or family psychoeducation, some rehabilitative intervention) were available for only some patients in merely one-quarter of Italian facilities. The observed association between psychoeducation and the availability of psychologists and rehabilitation therapists suggests that a more widespread implementation of these types of intervention can be achieved by increasing the availability of these professionals in psychiatric facilities.
Similarly, few head psychiatrists reported CBT being used on a regular basis. Yet a growing literature suggests that CBT can be used during inpatient care [8, 9], and there is evidence that it can reduce both negative and positive symptoms, accelerate recovery, and decrease time to discharge [10].
Overall, our findings suggest that acute facilities are dominated by a strictly medical approach. Yet the centrality of pharmacological therapy in acute inpatient facilities is often at odds with patient expectations. Other studies, conducted in Germany [11] and in the UK [12], found that patients welcomed more interpersonal contact with staff and were dissatisfied with the limited amount of time they had available to talk with doctors.
The central role assigned to pharmacological interventions may also affect staff morale and increase rates of turnover and sick leave. Ward psychiatric nurses report being particularly dissatisfied with the difficulty in forming therapeutic relationships, which is at least in part due to the environment organization: much of their time is spent on administrative or executive tasks (e.g. phone calls, paperwork, dealing with unexpected incidents etc.) and in the nursing station, rather than in face-to-face contact with patients [13].
Experience of acute psychiatric admission and the process of care
Admission to an acute psychiatric inpatient facility is often a distressing experience, and all too frequently the first days of stay are particularly confusing and boring for patients and their families, who do not yet understand how the unit operates [14]. Although provision of counselling can represent a useful form of intervention for helping patients and their relatives cope with this event, this type of intervention was not provided in approximately 20% of the facilities surveyed. This finding is in contrast with the observation that lack of information is significantly related to inpatients’ and relatives’ dissatisfaction with GHPU care [15].
Regular clinical evaluation and supportive sessions represent the core of inpatient care, and also allow for the regular monitoring of patient clinical condition. Nonetheless, regular clinical evaluation and at least 30 min-long supportive sessions were not conducted in approximately 20% of the facilities: a finding that raises concern.
Rehabilitative intervention was available in only half of the facilities. It may be argued that structured rehabilitation should ideally be provided after discharge into community services, but even socializing activities that are easy to conduct, such as physical exercise groups, discussion groups, or expressive activity groups, are not in widespread use, another finding that raises concern. Poor amenities and the lack of structured occupational or recreational activities can lead to risk situations because most aggressive acts occur when no activities are taking place. In the present study inpatients in approximately half of the acute units were uninvolved in any structured social or recreational activities. This finding is consistent with a recent UK national survey reporting that 40% of inpatients were involved in no form of social or recreational activity [1].
Evidence-based activities such as vocational and social skills training, and programmes to teach or enhance skills in coping with stress and anger were also rarely provided, although their inclusion in individual patient care plans is recommended [14].
Potentially contributing factors for the primacy of pharmacotherapy in acute inpatient facilities
Various factors most likely contribute to the primacy placed on pharmacotherapy in psychiatric inpatient settings, for example (i) the fact that, upon admission, most patients are suffering from acute psychotic disorders – a phenomenon placing clinicians under pressure to achieve rapid treatment effectiveness; (ii) lack of (or reduced) professional input from clinical psychologists, occupational therapists, and social workers; (iii) a general lack of professional training in various types of psychosocial interventions and (iv) the commonly held belief that psychosocial intervention should be conducted mainly by community-based services.
With regard to the first point, medication can be more effective when administered in conjunction with appropriate psychosocial intervention [10]. Second, the present study found that the provision of rehabilitative intervention was associated with greater professional input from psychologists and rehabilitation therapists; this result suggests that the limited provision of psychosocial intervention may also be related to poor availability of these specific professional figures in acute inpatient facilities.
An unexpected result was the association observed between higher nurse provision and delivery of psychotherapy. A higher nurse provision most probably represents a proxy for better quality of care, including the provision of a wider range of programmes.
The problem of insufficient staff training in various forms of psychosocial intervention, including CBT techniques, has also been observed abroad [16]; the latter have been suggested as the standard for training staff working in inpatient units [16].
As to the fourth point, it is questionable that community-based services can offer a comprehensive range of psychosocial interventions. At the same time, however, these types of intervention are widely unavailable in GHPUs, where people are most ill, vulnerable, and in need of help: service users in acute care should have priority access to various types of programmes [6]. Moreover, the event of inpatient admission provides an ideal opportunity to embark upon compliance therapy [17] and to foster the necessary therapeutic alliance with the service that will eventually be responsible for aftercare. Interestingly, we found that more than 40% of admitted patients were at their first-ever contact with the inpatient facility, and it is likely that most of them were in the early phases of their disorder – a critical period for establishing an effective therapeutic alliance. Providing these patients with medication only may lead to a higher risk of drop-out from post-discharge care, because patients are unlikely to continue treatment if they are dissatisfied with their inpatient stay.
Integrating patients into their social networks, and patient care service integration
Many studies have shown the importance of promoting patient integration into the local community [18]. The present study found that only a few acute units in Italy have specific programmes with this aim.
Overall, only half of the acute units reported working actively to involve other health and social services in patient care. Practical matters, such as links with welfare, housing, and employment agencies were little dealt with during inpatient stay. Some reports suggest that the lack of suitable post-discharge accommodation contributes to the pressure on acute psychiatric beds [1]. One exception is represented by 24 h CMHCs, where the admission process is more flexible and less stigmatizing and where an essential treatment component is the link with communities services. The GHPUs that are able to refer patients to 24 h CMHCs may therefore involve a shorter duration of stay and not hinder social integration thereby.
Rules during patient stay
Whereas GHPUs and, to a lesser extent UPCs, seemed more concerned about the risk of patients absconding, 24 h CMHCs appeared to be more integrated in their social contexts by allowing more free exits. These differences in exit policy can be explained by several factors: one is the different case-mix, in that GHPUs, but not UPCs, admit compulsory patients, who may require closer observation and more stringent safety procedures, given the higher risk of absconding and violent behaviour involved [19]. Twenty-four hour CMHCs also admit compulsory patients, but the different rule policy may also represent the effect of less restrictive staff attitudes and more flexible attitudes toward patient treatment [Norico B: unpublished data].
A recent literature review has shown that patient dangerousness still represents one of the most frequent reasons for acute psychiatric admission [20]. Therefore, keeping patients safe is a major task for inpatient facilities. Policies such as locked doors and banning dangerous objects are generally aimed not only at protecting staff and other patients, but also the patients themselves from self-harm [21]. It is important to note, however, that safety cannot be assured exclusively through measures aimed at controlling patient behaviour [20].
We found that specific rules are more common in larger facilities. These facilities host a number of patients exceeding 15, indicated as the optimal number of beds in psychiatric acute inpatients units [6], and may face a higher risk of having to deal with undesirable behaviours.
Some associations emerged for presence of some specific rules and episodes of physical restraint, a finding perhaps indicating that facilities adopting more rules use restraint more frequently. We did not find an association between locked doors and staff provision, which suggests that providing more staff hours per se does not reduce the need for coercive measures; for example, when there are no specific, appropriate policies in place, such as the availability of specific programmes aimed at training staff to deal with violent behaviours.
Limitations
The present study has several limitations. First, information about treatment and intervention were provided by facility head psychiatrists, and it was not possible to verify the accuracy of these replies. The reports were taken at face value, but it was not verified whether all interviewees’ responses reflected the actual facility situations. We also did not assess the appropriateness of the types of intervention that were reported, nor we were able to ascertain how frequently they were used, nor how many patients were involved. A second phase of the present project, in which researchers assessed a random sample of facilities and individually evaluated a representative sample of inpatients, has been recently completed. This second-phase study will soon make available more thorough information about all of these issues. Another limitation lies in the cross-sectional design of the survey, which does not allow for the drawing of causal inferences.
Given that the reliance on manager reports has most probably led to an overestimation of intervention provision, it should be stressed that the current degree of provision of specific forms of evidence-based psychosocial intervention, which are particularly crucial to inpatient care, is limited.
We could not ascertain whether rules were rigidly imposed on all patients, or whether they were used flexibly, based on patient needs and clinical status. More importantly, no outcome data were available to clarify whether there might be an association between rules and recurrence of incidents or negative patient outcomes in the facilities surveyed.
Conclusions
With these limitations in mind, the present study suggests that the provision of psychosocial interventions in Italian public inpatient psychiatric units is limited, and that many of these facilities are poorly linked to community-based services. Specifically designed studies should be performed to provide compelling evidence that outcomes are better in services providing psychotherapy and rehabilitation in addition to pharmacological treatment in the context of integrated community care. Moreover, a large survey of professional and patient opinion may help elucidate both patient needs and the difficulties that professionals face in trying to meet their demands. Such additional work may help identify and introduce the changes in the public health-care system necessary to improve clinical care.
Indeed, acute psychiatry has the complex task of managing patients at the most critical stages of their lives. It is probably time to review acute hospital services with the same determination with which community services were once promoted. Action is needed to introduce treatment procedures of proven effectiveness. All efforts should be made to develop training programmes, working practices, and an effective interface between hospitals and community mental health teams, in order to ensure the continuity of care for patients across services.
Footnotes
Acknowledgements
The study was supported by a grant from the Ministry of Health. Dr Giorgio Bignami provided continuous support throughout the entire National Mental Health Project, during which this study was conceived; Ms. Elena Cuomo has provided valuable bibliographic help throughout project. The PROGRES-Acute was coordinated by the Italian National Institute of Health and the Department of Mental Health of Trieste and includes: National and Regional Coordinators, and scientific consultants: F. Amaddeo, A. Barbato, G. Borgherini, G. Borsetti, R. Bracco, R. Canosa, M. Casacchia, I. Casula, P. Ciliberti, A. Colotto, A. D'Aloise, G. de Girolamo, G. Dell'Acqua, M. De Palma, W. Di Munzio, A. Gaddini, G. Grassi, N. Longhin, M. Miceli, R. Miglio, P. Morosini, M. Nicotera, M. Percudani, B. Norcio, A. Picardi, R. Potzolu, E. Rossi, P. Rucci, G. Santone, S. Schiaffino, F. Scotti, R. Tomasi, G. Turrini, E. Zanalda. Researchers: G. Agostani, F. Basile, F. Basilico, N. Battino, L. Bavero, G. Bazzacco, L. Biscaglia, R. Borio, S. Buttacavoli, B. Caporali, F. Cappelletti, L. Caserta, L. Cifarelli, P. Congia, M. Dazzi, L. Elia, E. Fantini, A. Galli, R. Gangi, A. Ghidoni, P. Ghirardo, L. Giordano, S. Goldoni, S. Marchigiani, G. Morelli, M. Nassisi, E. Paltrinieri, K. Pesaresi, A. Pettolino, L. Pinciaroli, G. Pitzalis, M. Severini, C. Sighinolfi, G. Spinetti, A. Trequattrini, U. Unterfrauner, K. Wolf, L. Zecca.