
Abstract
In the past, violence and aggression were often seen as an inevitable aspect of a chosen profession [1]. A growing number of countries and jurisdictions are implementing zero tolerance policies to target these attitudes and address concerns about increasing levels of violence within the health sector. Several prominent cases of assault in the New South Wales health-care setting led to the recognition that uniform aggression and violence minimization policy and training were a high priority for the health service. In June 2001 a NSW Health Taskforce on the Prevention and Management of Violence in the Health Workplace was formed. A policy document, titled “Zero tolerance policy and framework guidelines” [2], was a key outcome of this taskforce and was based on the “NHS zero tolerance zone” materials that were developed by the National Health Service in the UK [3]. The key message of the policy is that health services must establish and maintain a zero tolerance to violence culture. This message is being disseminated throughout the health service via posters that include slogans such as “NSW Health is a zero tolerance zone”, “Violence and verbal abuse will not be tolerated” and icons giving visual reminders of a zero tolerance culture such as the palm of a hand in a position indicating ‘stop’.
Although evidence supporting a zero tolerance approach to aggression and violence in mental health services is lacking, such policies have been put forward as a desirable way of dealing with these problems in the health sector. However, the confidence with which zero tolerance initiatives have been implemented has begun to be questioned [4], with attempts to understand the social context of violent and aggressive incidents being explored in the literature [5]. Indeed, several researchers have claimed that zero tolerance campaigns are unlikely to succeed without examining the broader context within which aggression and violence occur [6, 7]. Furthermore, some authors suggest that a zero tolerance approach toward aggression in the health sector may be associated with increases in the use of inappropriately high-intensity interventions in response to aggressive behaviour [8].
Whittington examined the concept of tolerance empirically among 37 mental health staff [9]. The Tolerance Scale [9] was used to examine the extent to which an individual expresses an awareness of the possible reasons that a person may act aggressively. Results of the Whittington study indicated that more experienced mental health staff reported a higher tolerance for aggression, which was also associated with lower staff burnout [9]. Whittington interpreted these findings to suggest a possible counterintuitive, professional wisdom for understanding the function of aggressive behaviour within the context of mental health [9].
During the development of a new aggression minimization training programme for NSW health staff, the recently developed NSW zero tolerance policy [2] was adopted and key elements were included in the new training initiative. This unique situation provided a context for assessing the effect of a zero tolerance approach on staff attitudes to be explored naturalistically, through a comparative study. This study compares a training programme that had been used to train health service staff in aggression minimization just prior to the introduction of the new policy, with the same intervention after the zero tolerance policy was included. Both training interventions included participants from the same participant pool, that is, from the NSW Health Service, and the same trainers trained both groups using similar training materials. Furthermore, trainers were blind to the purpose of the study and as such implemented the training in good faith, that is, the trainers and the training were independent of the research and the researchers.
Method
Training
Data were collected on two aggression minimization training programmes for health staff. Prior to training and at follow up participants completed a series of evaluations. Both training programmes were manualized and were essentially modules 1 and 2 of the statewide programme [10], before and after the zero tolerance content was added. That is, the only difference in content between the two programmes was the new zero tolerance policy information for dealing with aggression and violence in the health workplace, contained in intervention 2. There were six zero tolerance attitudes and behaviours documented in the policy and disseminated in the training manuals. In abbreviated form these key principles were: (i) putting up with violence is not an acceptable part of job; (ii) know your options when confronted with aggression; (iii) management will support you and it is their responsibility; (iv) report it; (v) be aware of violence as an occupational risk; and (vi) be vigilant. These messages emphasize being alert and cautious and focus on attributing responsibility for violence to others. Because training intervention 1 was developed prior to the policy introduction it did not include information on the new zero tolerance approach. Training duration was 2 days and the programmes were identical in terms of trainers and target audience. Training occurred over a period of 6 months in regional areas of NSW and 15–25 participants were trained in each session.
Participants
A total of 117 health staff completed training evaluations. Fifty-seven staff were trained with intervention 1 and 60 staff were trained with intervention 2. Participants provided written informed consent to allow the training programme data to be used for research evaluation.
Data collection instruments
Four instruments were completed by the participants, and they are listed as follows.
Rigid attitudes toward the management of aggression scale (IPP Rigidity Scale).
Measurements of health staff rigidity toward the management of aggression were obtained before and after training using a specifically designed self-report instrument developed within our Interpersonal Program (IPP) for managing aggression [11]. The scale consists of 10 items (rated on a Likert scale) indicating agreement or disagreement with statements that indicate rigid attitudes toward the management of aggression (e.g. ‘People who are aggressive should not be tolerated’, ‘Patients who are aggressive should not get the support of staff’). All items are scored in the same direction with high scores indicating a rigid approach to managing aggression. Previous pilot data have found the instrument to have high internal consistency with an alpha of 0.82.
Tolerance for aggression
Pre- and post-training measures of health staff tolerance for aggression were obtained using the Tolerance Scale [9]. This scale was derived from the Perceptions of Aggression Scale [12], in particular the subscale that characterizes ‘aggression as a normal reaction’. The tolerance subscale is made up of 12 items (rated on a Likert scale) indicating agreement or disagreement with four items that positively evaluate patient aggression (e.g. ‘Aggression helps to see the person from another point of view’) and eight that indicate an awareness of the possible causes of patient aggression (e.g. ‘Aggression is a form of communication and as such is not destructive’). All items are scored in the same direction with high scores indicating a high tolerance for aggression. This scale has been reported to have a high internal consistency with an alpha of 0.82 [9].
Confidence in dealing with aggression
Pre- and post-training measures of health staff confidence were obtained using the Confidence in Coping with Patient Aggression Instrument [13]. The instrument is a 10-item self-report questionnaire that addresses areas pertaining to ability, preparation, comfort in safety, effectiveness in intervening psychologically and physically with aggressive patients for self-preservation and therapeutic intervention (e.g. ‘How comfortable are you in working with an aggressive person?’ (rated from very uncomfortable to very comfortable)). Participants indicate their degree of confidence using a 10-point Likert scale with higher scores indicating greater confidence. During its development Thackrey [13] found the instrument to have a high degree of internal consistency with an alpha of 0.92.
Skill in dealing with aggression scale (IPP Skill Scale)
Pre- and post-training measures of health staff skill in dealing with aggression were obtained using a specifically designed 10-item self-report instrument [14] that addresses areas pertaining to: identifying high-risk patients, awareness of response options when faced with aggression, use of verbal and physical skills and awareness of legal issues and procedures that should follow an incident. Participants indicate their degree of skill and higher scores indicate greater skill (e.g. ‘How good are your current assessment skills for identifying high-risk aggressive people?’ (rated from very poor to very good)). Inter-item reliability was assessed for this instrument and the questionnaire was found to have a high degree of internal consistency with an alpha of 0.91.
Data analysis
First, independent samples t-tests and χ2 analyses were carried out on the sample to test for any pre-training differences between the groups. Second, t-tests were carried out to examine within-group differences from before to after training on rigidity, tolerance, confidence and skills for each training intervention. Finally, an ANCOVA was carried out to examine post-training differences between the training groups on rigidity, tolerance, confidence and skills, (controlling for pre-training scores). In all analyses, the criterion for statistical significance was set at p < 0.05.
Results
There were no significant differences between the groups with regard to age (38 years vs 41 years; t = − 1.70, p = 0.09), sex (63% vs 68% female; χ2=0.35, p = 0.56) or occupation (54% vs 47% nursing; χ2=0.56, p = 0.46). Half the sample from each group had a nursing background, with the rest consisting of allied and support staff (e.g. psychiatry, allied health, security). Prior to training the two groups did not differ with regard to rigid attitudes toward the management of aggression (n = 117, df = 1, t = 0.02, p = 0.99), tolerance for aggression (n = 117, df = 1, t = 1.17, p = 0.24), confidence in managing aggression (n = 117, df = 1, t = − 1.20, p = 0.23) or skills for dealing with aggression (n = 117, df = 1, t = − 1.10, p = 0.27).
Analysing the groups separately, both interventions were effective in increasing confidence and skills for dealing with aggression (p < 0.05). However, intervention 1 significantly decreased rigid attitudes toward the management of aggression while intervention 2 significantly increased rigid attitudes toward the management of aggression and decreased tolerance for aggression. In order to assess the significance of these findings, an ANCOVA analysis controlling for initial scores was computed between groups. When controlling for initial scores there were significant post-training differences between the groups on confidence (69.89 vs 62.62, n = 117, df = 1, F = 16.48, p = 0.00), skills (76.95 vs 71.55, n = 117, df = 1, F = 8.55, p = 0.00), rigid attitudes (37.28 vs 45.28, n = 117, df = 1, F = 12.81, p = 0.00) and tolerance (59.33 vs 45.13, n = 117, df = 1, F = 19.74, p = 0.00). Overall, after training, group 2 were significantly more rigid, less tolerant, less confident and less skilled than group 1. Figure 1 reports the baseline and post-training means and standard error scores for each group on the four attitude and skill scales.
Pre- and post-training mean scores and standard error bars for each aggression minimization training intervention (group1, pre-zero tolerance training; group 2, zero-tolerance training) on the staff variables of interest (staff rigidity, tolerance, confidence and skill in managing aggression).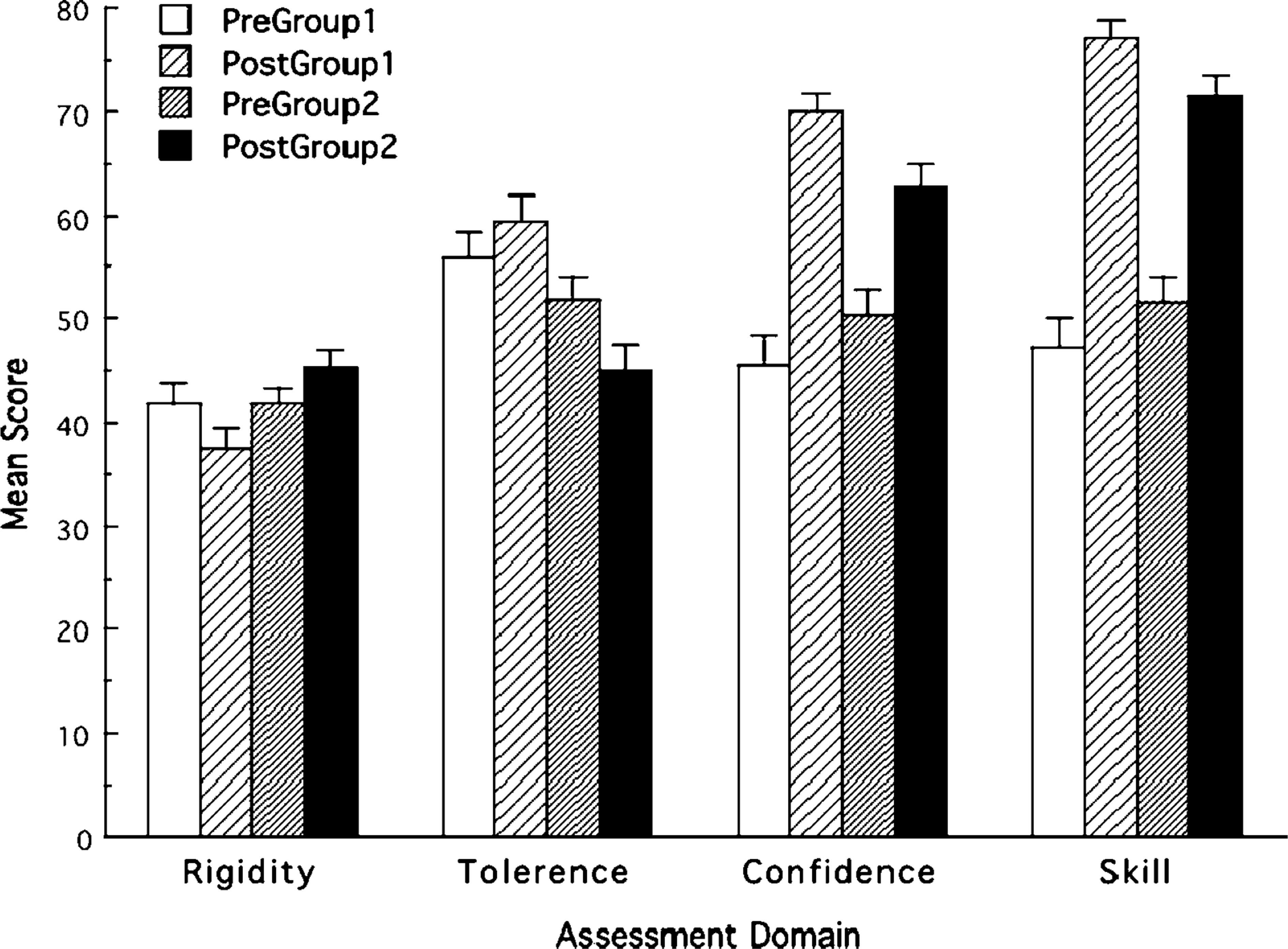
Discussion
This study found that training in zero tolerance had the unintended consequence of increasing rigid or inflexible attitudes toward the management of aggression in the health workplace, while reducing tolerance toward aggression. In light of previous research findings indicating that: (i) health staff with more experience tend to have a more tolerant attitude toward aggression; and (ii) that higher tolerance for aggression is associated with less staff burnout [9], the present results suggest that there are problems with a zero tolerance approach to aggression management training.
It is of interest that intervention 2 did not increase confidence and skills to the same degree as intervention 1. Possibly these variables were affected by the increase in rigid attitudes that intervention 2 appeared to generate. Perhaps being more rigid and less tolerant leads to a perception of lower confidence and skill when responding, that is, there is a reduction in perceived options and confidence in handling violent incidents. Zero tolerance implies that staff should be fearful of all aggression, which might engender a more negative perception of the helpful role.
The present results support other findings that have identified confusion in the zero tolerance message [15]. Pilot testing of an aggression minimization training programme that was based on the new NSW policy indicated that zero tolerance was interpreted by participants as implying an attitude of withdrawal and punishment toward any individual exhibiting aggressive behaviour, when in fact the intended meaning of the zero tolerance policy was that all instances of aggression and violence should be taken seriously rather than treated simply as part of the job [15]. It seems possible that the salience of the terms ‘zero tolerance’ and ‘elimination of violence’, may confuse the actual definitions put forward in the policy such that the practical interpretation of the policy may be quite different to its intended meaning.
This study was unique in that a rare opportunity provided a naturalistic context for exploring the impact of a zero tolerance policy, in relation to aggression and violence, on health staff attitudes. Despite the methodological advantages of the present study, it is possible that subtle differences in the training interventions could have impacted upon the findings in a way that was difficult to identify. If this was the case there may have been factors other than the zero tolerance policy approach that brought about the attitudinal differences between the training groups. More qualitative work, such as staff and patient interviews, might be helpful to investigate in a more direct way the impact of zero tolerance approaches to aggression and violence, rather than the indirect measurement of self-reported attitudes utilized in the present study.
Whittington and Higgins suggest that government policy that promotes an attitude of zero tolerance may encourage practitioners to assume that any aggressive behaviour by a patient is inappropriate, resulting in the use of immediate, high-intensity interventions that may not match the appropriate level of intensity of the aggressive behaviour [8]. In light of this possibility future work should seek to clarify and expand on the important results found in our study. It is undesirable that the introduction of a zero tolerance policy toward aggression and violence might impact negatively on staff attitudes for dealing with aggression, because this may counteract its original intention of reducing aggression and violence in the health workplace.