
Abstract
Psychiatric mother and baby unit (MBU) services are being developed worldwide [1]. These specialist services allow mothers with severe perinatal mental illness to be admitted jointly with their infant, while the mother is treated, to promote the formation of their relationship. An audit of MBU admissions in the UK reported generally positive clinical and parenting outcomes at hospital discharge [2]. However, the audit highlighted concerns about the capacity of women with more severe illness to provide practical care or to be emotionally responsive to their child. Mother–infant interaction deficits have been consistently reported in studies of MBU patients in the UK [3–5] and Australia [6]. Increasingly, the role of MBUs is being extended to include parenting assessments regarding the capacity of women with severe mental illness to care for their children [7].
Snellen et al. called for the development of integrated services following discharge from MBU inpatient treatment [6], but little is known about the later outcomes of children whose mothers have previously been admitted to an MBU. The Hipwell et al. study of MBU mother–infant dyads (excluding mothers with schizophrenia) found that, although few maternal symptoms were detected at 1 year after birth, MBU mothers (n = 25) were less sensitive, less appropriate in play or expectations about the infant, and expressed more negative affect than matched controls [3]. However, rates of attachment insecurity and disorganization (8/19) were comparable with matched controls (7/19). Mothers with unipolar depression were much more likely to have children with insecure or disorganized attachments (7/9) than mothers with bipolar depression (1/10). Cunningham et al. reported that 21 children of 13 mothers who had been admitted to an MBU showed poorer behavioural and emotional functioning than children in the general population, but comparable rates of attachment insecurity [8]. That study, however, relied solely on mother-reported postal questionnaires and the children were of an unusually wide age range for a developmental study (3–12 years). Possible age effects were not examined. Other studies of children of mothers with depression and schizophrenia have produced mixed findings regarding cognitive, behavioural and emotional outcomes [9–11].
We report on whether young children, previously jointly admitted with their mother to a psychiatric MBU following the onset of severe maternal mental illness, showed poorer developmental outcomes than would be expected from comparison and standardized child norms. In part, the study was designed to test the feasibility of recruiting a cohort of mother–child dyads at school age (i.e. several years after discharge) and assessing cognitive, motor, social, sociocognitive (‘theory of mind’) and emotional functioning, and attachment security.
Method
Sample
Ninety-four mothers had been admitted to the psychiatric MBU in Manchester, UK, following their child's birth, whose children (n = 95; one set of twins) were identified as being between 4 years 6 months and 6 years 11 months during the study's recruitment period (8 March 2004–31 August 2005). Extensive efforts were made to obtain the patient's most up-to-date home address and current general practitioner (GP) through MBU admissions information and through two National Health Service Mental Health and Social Care Trust database systems. To be eligible to participate, the Primary Care Trust of the patient had to approve the study, 26 Trusts in total, before GPs could be approached, and GPs had to be willing to confirm the following: the mother and child's health status (i.e. well enough to participate), the mother's current home address at which the child was also registered, which had to be within a 50 mile (60 km) radius of the City of Manchester for home visit purposes. Ethical considerations determined all eligibility criteria except the study area, which was determined for practical reasons. GPs were approached by letter (followed by telephone calls) up to three times to obtain this patient information. The study was approved by the NHS Multisite Research Ethics Board. Eligible mothers were invited by letter for their child and themselves to participate in a follow-up study. To recognize their time and participation, a gift of £20 and a toy worth up to £5 were offered to participants.
Measures
On the McCarthy Scales of Children's Abilities (MSCA), systematic observation of performance on a range of tasks yields a standardized general cognitive index score, which comprises verbal, perceptual and quantitative index scores, and a memory and motor index score [13].
The Manchester Child Attachment Story Task (MCAST) is a validated semi-structured doll play assessment that elicits the child's attachment representations of his/her mother [14]. In each of four test vignettes, the child is prompted to complete a prescribed story, requiring the enactment of an attachment-related issue. The videotaped responses were coded by the first author who was blind to maternal diagnosis.
The Attachment Behaviour Questionnaire (ABQ), was adapted from test statements on the Attachment Behaviour Q-Set (Version 3.0) [15, 16] to obtain maternal ratings on 20 attachment security behaviours on a five-point scale.
The Strengths and Difficulties Questionnaire (SDQ) [17] is a validated brief behavioural screening measure, which asks about 25 attributes, generating scores for conduct problems, inattention–hyperactivity, emotional symptoms, peer problems and prosocial behaviour, the first four summed to create a ‘total difficulties’ measure.
Two ‘theory of mind’ (social mentalizing) tasks assess the ability to understand the beliefs, emotions and desires of toy characters and thus to engage with another person on a mental level. Performance on almost identical tasks at 5 years was found to be associated with earlier attachment security [18]. The tasks are slightly modified versions of the Taylor et al. ‘picture identification task’ [19] and the Harris et al. ‘false belief and emotion’ task [20].
The Beck Depression Inventory (BDI) is a widely used 21-item self-report questionnaire that measures current adult depressive symptoms [21].
Clinical information during MBU admission was obtained through clinical notes and the Marcé clinical audit database [2, 22]. Current clinical and sociodemographic information was obtained through maternal report.
Procedure
During a 2 h home visit, the child was assessed (blind to maternal diagnosis) on the MSCA and, following a break, on the MCAST and social mentalizing tasks. In a separate room, the mother was briefly interviewed to collate sociodemographic and clinical information and given the SDQ, BDI and ABQ. At the mother's request, the child's class teacher completed and returned the SDQ.
Results
Sample characteristics
Fifteen mothers and 16 children (one pair of twins) participated in the study, which constituted 16% of total admissions and 28% of eligible participants (Table 1). At admission to the psychiatric MBU, the mean maternal age was 28.93 years (SD = 5.13) and the mean infant age, 8.27 weeks (SD = 5.80). The mean timing of admission was at 7.53 weeks post-partum (SD = 6.15) and mean duration of admission, 6.80 weeks (SD = 5.47). At discharge, 4/14 mothers (29%) had been rated by clinical staff as having a ‘significant problem’ in the practical care of and/or emotional responsiveness to their child, as recorded in the Marcé clinical database (two depression, one bipolar disorder, one schizophrenia), which is comparable to data from the national MBU cohort (28.57% [22]). At participation, 13 women (87%) were married (all to the father of the index child), nine (60%) had current mental health needs (based on self-report), but only 3/14 (21%) screened positive for current depression on the BDI (one severe, two mild-moderate; one did not feel well enough to complete the BDI). The distribution of socioeconomic status was as follows: six professional/managerial, four skilled/manual, two semi-skilled/unskilled, three never employed and one unclassified. Although 29% of admissions resided in the region covered by the Manchester Primary Care Trusts, only two women (13%) from this region participated, the remainder coming from the surrounding area (i.e. not from the city). Eight boys and eight girls participated in the study, with a mean age of 5.38 years (three children had reached the age of 7 by the time of assessment).
Eligibility and recruitment by maternal diagnosis
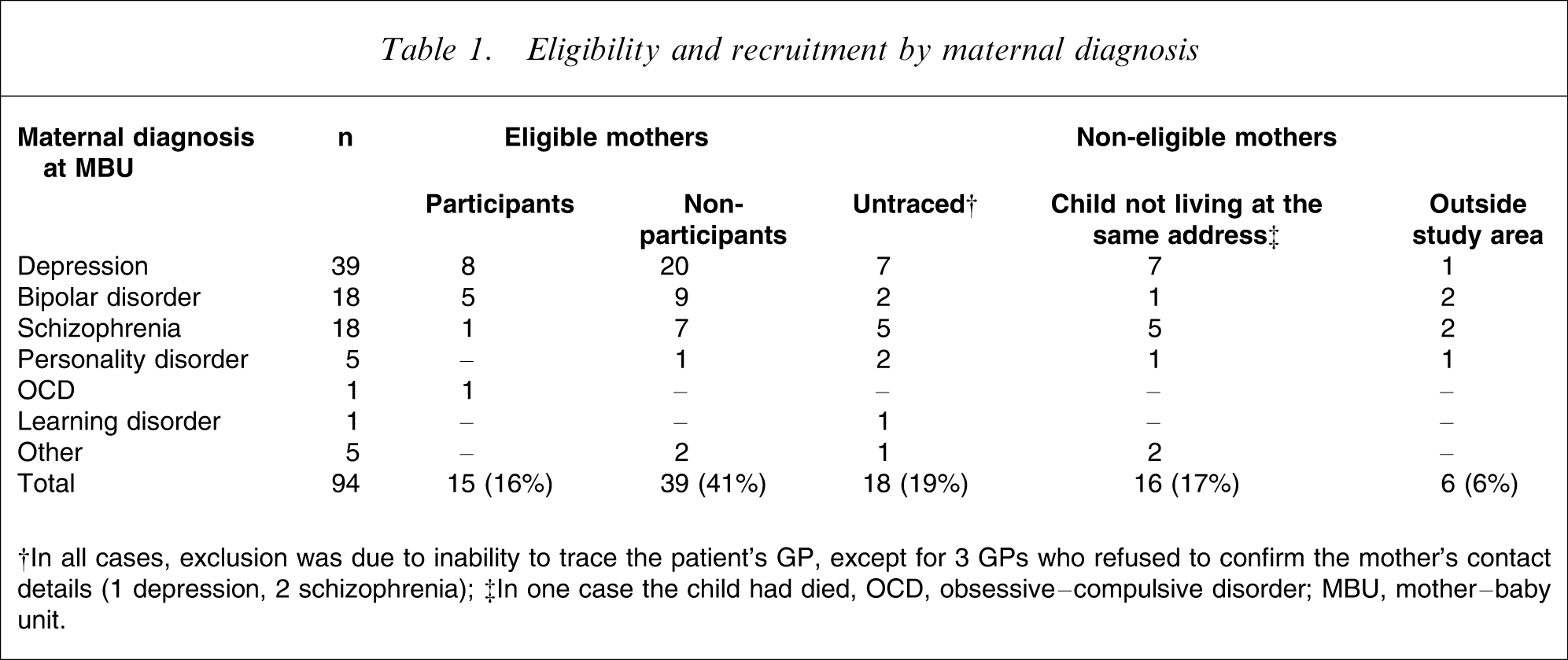
†In all cases, exclusion was due to inability to trace the patient's GP, except for 3 GPs who refused to confirm the mother's contact details (1 depression, 2 schizophrenia); ‡In one case the child had died, OCD, obsessive–compulsive disorder; MBU, mother–baby unit.
Behavioural, emotional and cognitive functioning
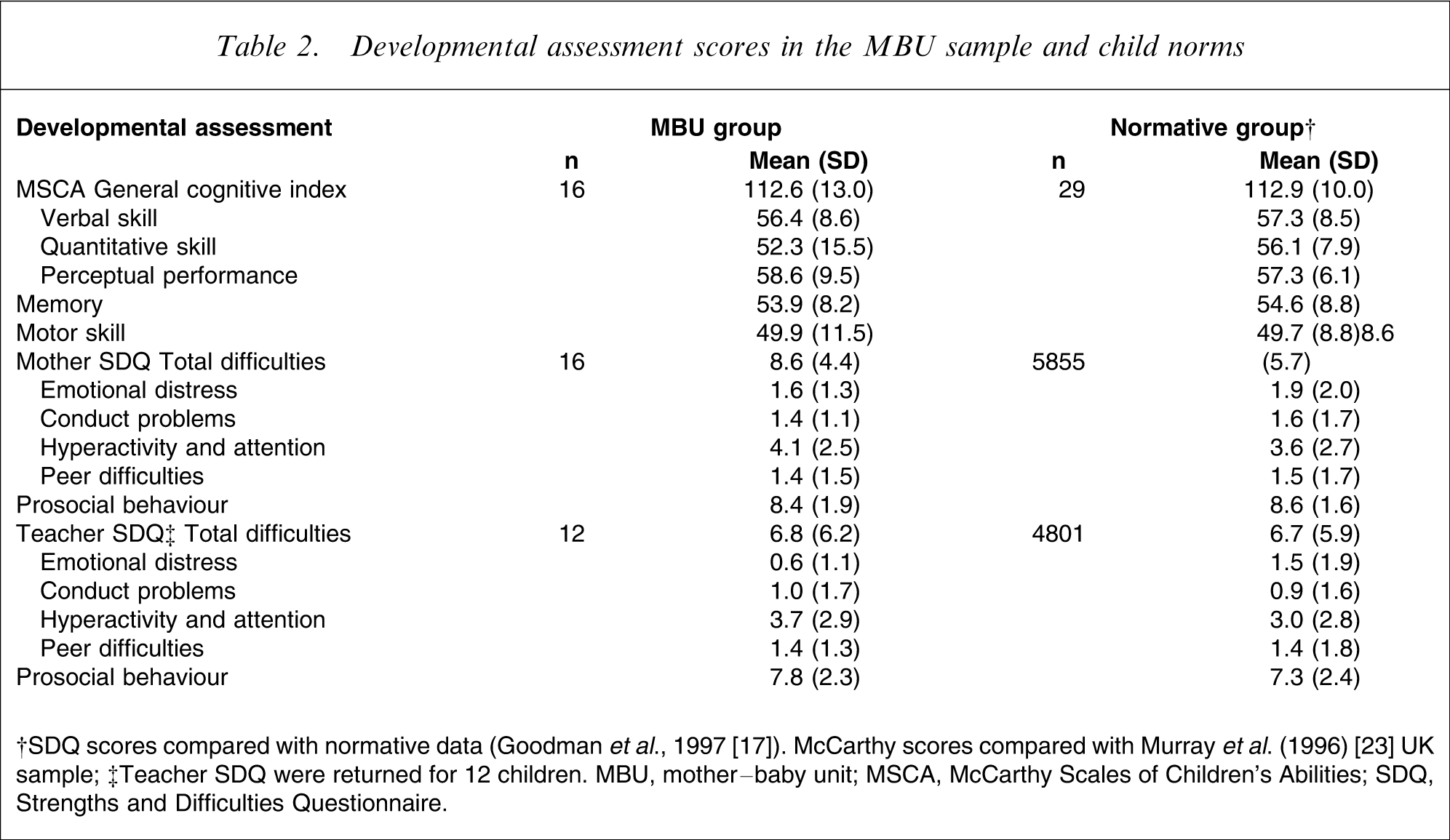
Cognitive and motor performance (MSCA) and mother- and child-reported behavioural and emotional ratings (SDQ) in the MBU group were remarkably similar to standardized normative sample data (Table 2). A lower quantitative mean score was due to one child's refusal to complete most of the number tasks (score = 6). Based on the MCSA classifications [13], no participants performed below average. On the SDQ, slightly higher ‘hyperactivity and attention problems’ and slightly lower ‘emotional distress’ (particularly in the teacher SDQ) were found. Based on the mother SDQ, children scored for ‘caseness’ in the following areas: hyperactivity/inattention, n = 3; peer problems, n = 2; and (poor) prosocial behaviour, n = 1. Based on the teacher SDQ, children scored for ‘caseness’ in: total difficulties, n = 1; conduct problems, n = 2; hyperactivity/inattention, n = 1; and (poor) prosocial behaviour, n = 1. No relationship was found between mother-reported and teacher-reported SDQ total difficulties (total difficulties: r = 0.14; p > 0.05), or SDQ subscales. On the mother SDQ, two of three who were borderline cases on total difficulties (score = 14 and 15) were attributed very low (normal) scores of 2 and 3, respectively, by teachers (the other did not receive a teacher rating). The child who reached ‘caseness’ for total difficulties on the teacher SDQ (scoring 20) was attributed a ‘normal’ score of 11 by the mother.
Developmental assessment scores in the MBU sample and child norms
Age and socioeconomic status distributions were equivalent across gender. Boys were attributed poorer scores than girls on all scales, particularly in general cognition, quantitative skill, memory, and mother- and teacher-reported total behavioural and emotional difficulties (Table 3). Children of mothers with current self-reported mental health problems also achieved poorer scores, particularly in general cognition, verbal skill, quantitative skill, mother-reported total difficulties and teacher-reported prosocial behaviour (Table 3).
Developmental assessment mean scores (SD)
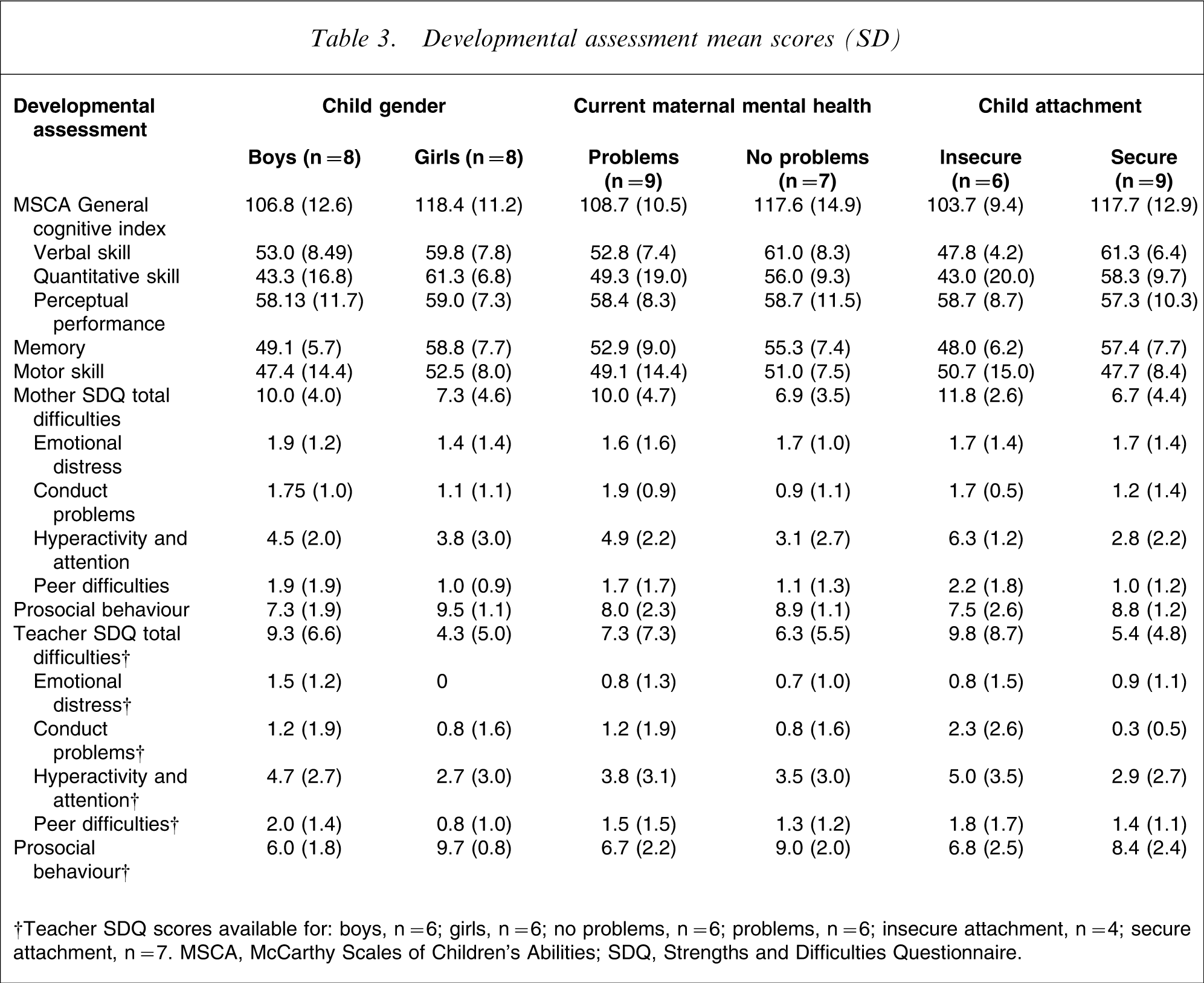
†Teacher SDQ scores available for: boys, n = 6; girls, n = 6; no problems, n = 6; problems, n = 6; insecure attachment, n = 4; secure attachment, n = 7. MSCA, McCarthy Scales of Children's Abilities; SDQ, Strengths and Difficulties Questionnaire.
Child attachment
All participants were evaluated with the MCAST; one was omitted from analysis because of problems with the taped clip. Of the remaining 15 participants, nine (60%) were coded as securely attached and six (40%) were insecurely attached (five or 33.3% were insecure-avoidant, and one or 6.7% was insecure-ambivalent). These proportions compare well with the performance of a normative sample of 53 children (mean age = 6.3 years): 33 (62.3%) secure and 18 (34.1%) insecure, four (7.6%) of whom were ambivalent and 14 (26.5%) of whom were avoidant [12]. However, 14 (26.4%) of the normative sample, but none of the MBU group also had (primary) disorganized attachments. Mothers’ reports of child attachment behaviours (on the ABQ) were similar for both MCAST secure and insecure groups (78% vs 76%; the higher the more secure).
Five of the six insecurely attached children had mothers with current self-reported mental health needs compared with 3/9 of the securely attached children. Insecurely attached children had more emotional and behavioural concerns as rated by their mother and, to a lesser extent, as rated by their teacher, particularly in hyperactivity and attentional difficulties (Table 3). Lower general cognition scores were achieved by insecurely attached children than securely attached children, with large between-group differences in verbal skill, quantitative ability and memory (Table 3). The number of insecure child attachments in each maternal diagnostic group was as follows: depression, 2/8; bipolar disorder, 2/4; schizophrenia, 1/1; obsessive–compulsive disorder, 0/1.
Theory of mind
Two children did not complete these tasks. In the picture identification task, nine children were excluded from analysis: five due to negative response bias; one due to positive response bias; and three for incorrect answers to control questions. Of the remaining five, one received a maximum score of 2 and four received a score of 1.
The exclusion rate was very high (64%) and maximum score rate was low (20%) compared with 10/33 (30%) and 16/23 (70%), respectively, in the Meins et al. normative sample of a comparable mean age (5.13 years) [18].
In the false belief and emotion task, one child was excluded due to response bias. Of the remaining 13, five scored a maximum of 4, two scored 3, one scored 2 and five scored 0. The mean number of correct responses (M = 2.15, SD = 1.86) was similar to the Meins et al. normative sample (no total score provided, but secure attachment group, M = 2.25, SD = 1.44; insecure attachment group, M = 1.62; SD = 1.33). The data are consistent with our small secure (M = 2.5, n = 8, SD = 1.69) and insecure group (M = 1.0, n = 4, SD = 2.0).
Discussion
Despite intensive efforts to maximize participant recruitment in our single-session home-visit design, the final sample was small. Participant recruitment was challenging at every stage in the processes of tracing the women to their current address, obtaining cooperation from the patients’ GP concerning participant eligibility, gaining Primary Care Trust approval across a widespread region and recruitment itself. The sensitive nature of this study meant that ethical considerations largely determined the inclusion criteria, which may have resulted in the exclusion of those children at highest risk. For example, two women who had agreed to take part were later reported to be too unwell to participate. Women may not have wanted to take part for fear of being judged as bad mothers, of having their child removed to care, or of being reminded of distressing past experiences surrounding their illness and/or care.
In spite of the low recruitment rate, we believe that this study provides useful information, particularly because this kind of follow up is rare. We obtained data on whether the index child was living with the mother 4–6 years after MBU discharge. Consistent with care status at discharge, the children of mothers with schizophrenia were least likely to be living with them (31% confirmed out of the broader sample). The proportion of depressed mothers whose index child was not living at the same address was 16%. In the present sample of children whose mothers had been admitted to a psychiatric MBU after their birth and who were currently living with them, we found no evidence of poorer emotional, social or cognitive developmental outcomes using observational, teacher-reported and mother-reported measures compared with comparison and standardized normative data. We did find that overall boys had poorer outcomes than girls, consistent with previous studies in children of depressed mothers [23–25]. Scores were poorest in children of mothers with current illness although we are unable to determine the relationship between timing or duration of maternal illness and child outcomes.
Children of mothers with current illness were more likely to form an insecure attachment which, like the Cunningham et al. study [8], we found to be related to poorer emotional, behavioural and cognitive outcomes, but we used observational and multi-informant assessments. Replication is needed in a larger sample, but the results could be taken to support the notion that a secure child–mother attachment protects against poor behavioural and cognitive outcomes in this group. Current mental illness is likely to significantly reduce the emotional availability and behavioural sensitivity of a mother [3–5], which impacts on the child's developing attachment relationship with her [26]. Other studies have shown that insecure attachment is related to poorer behavioural and cognitive development [27–29], perhaps due to its impact on emotion regulation and social adjustment. Thus, where maternal illness is chronic, the availability of other caregivers such as the father and other relatives is likely to be important not only as a source of social support for the mother [2] but also to protect the long-term developmental outcomes of children.
The findings may suggest that MBU services need to be developed that consider the longer-term consequences for infants of exposure to maternal mental illness. Attention is needed for risk assessment during admission and post-discharge monitoring, possibly through standardized observation [3–6]. Because most mothers are discharged before 1 year post-partum when infant–mother attachment patterns begin to form, MBU facilities may be well placed to provide interventions to prevent the development of insecure attachment relationships, such as by enhancing maternal sensitivity [30].
The sample available for follow up by GP contact, and who responded to a request to take part, represents a small proportion of possible participants. Our findings are limited by this small sample and we were unable to make inferential statistical comparisons or identify predictors of poor developmental outcome. Most women who took part were living with the father of their child, outside the City of Manchester. Mothers with bipolar disorder were most likely to participate and mothers with schizophrenia were least likely to participate. Our findings are consistent with previous reports suggesting that good parenting outcome in mothers from an MBU is associated with having a stable relationship [2]. The present cohort was also stable in the sense of being traceable 5 years following discharge. The tasks we posed for mothers and children were broad ranging and lasted approximately 2 h. Apart from obstacles to recruitment, we found that this type of study was both feasible and acceptable to the women who participated and their children, even in the context of current illness. The only measure with poor completion was the theory of mind tasks, probably because the children were becoming tired and inattentive towards the end of the assessment session. However, low BDI scores (n = 8 scored <4) suggest that women want to be viewed to be well and coping, because most women also reported current mental health problems. The various inconsistent results in the present study suggest that maternal report alone is unreliable and probably compounded by poor current mental health. These inconsistencies highlight the importance of assessing child outcomes through multi-informant and observational measures.
It is our recommendation that developmental follow up should be integrated into an aftercare service. This is in line with recent policy developments in the UK that call for bridge-building between mother and child services [31, 32]. This would require contacting mothers at regular intervals after discharge and would overcome many of the difficulties encountered in the present study. This kind of support in itself might improve child outcomes. Our findings must be considered preliminary and replication of these finding is required. Future research may best be focused on implementing and evaluating interventions that (i) target mothers with chronic mental illness and those with poor social supports (e.g. without a partner); (ii) focus on promoting secure attachment [30]; and (iii) assess whether child outcomes improve when secure attachment is enhanced.
Footnotes
Acknowledgements
The authors would like to thank Professor Jonathan Green for his input and training on the Manchester Child Attachment Story Task, and Dr Angelika Wieck and Margaret Salmon for their cooperation in providing MBU admission information.