
Abstract
Homeless people commonly report a history of trauma. Over two-thirds of homeless women in Portland, Oregon reported a lifetime experience of physical abuse [1]. A lifetime experience of rape was reported in New York city by 43% and in St Louis by 20% of homeless women [2,3]. In two cities in New England 89% of homeless women had experienced physical or sexual abuse in their lifetime [4]. A history of trauma among homeless men, although less well documented, is also high. In St Louis 21% of 600 men reported a lifetime episode of assault and 14% ‘a sudden injury or accident’ [3]. Among older homeless people in New York nearly half were robbed and over one-quarter were physically assaulted in the previous year [5]. The prevalence of these trauma among people who are homeless is far greater than for the USA general population [6], assessed using the trauma section of the Composite International Diagnostic Interview (lifetime) 2.0 (CIDI) [7]. There is no published data concerning lifetime trauma in the Australian population.
Differing geographical and cultural factors in the USA compared with Australia are likely to influence the prevalence of physical and sexual assault. An attempt to assess the prevalence of trauma among homeless people in Sydney seems warranted, given the likelihood that experience of trauma will be high. The aim of the present study was to assess the lifetime prevalence of trauma among homeless men and women in inner Sydney.
Method
The present study is part of a larger investigation concerning mental illness in homeless people [8]. We approached 289 people; 79 refused and a further 53 agreed, but were unable to complete the interview because they lost interest, were intoxicated or had cognitive impairment. One hundred and fifty-seven homeless people completed the interview. We adapted the definition of homelessness of Gelberg and Linn [9]: anyone who had spent the previous night in emergency shelter, outdoors, in a space not designed for shelter, at a hotel or motel, with a relative or friend, but was uncertain whether they could stay for at least 60 days, stated that they did not have a permanent house or apartment to which they could go, or had stable accommodation, but required daily support from services for homeless people.
We sampled from the dining halls of the seven largest refuges that cater to homeless single adults in inner Sydney. The chairs in each of the seven refuges were numbered and a random sample of chair numbers was then computer generated for a specific mealtime at each centre using SPSS (SPSS, Chicago, IL, USA). Each person occupying a targeted chair was asked to participate in the study as they left the dining hall. Subjects who agreed were given a comprehensive interview that included the nine-item trauma section of the CIDI. The interviewer introduces this section of the CIDI with the statement ‘now I would like to ask you about extremely upsetting or stressful events that sometimes occur to people.’ The relevant ethical committee granted approval for the study.
Results
One hundred and fifty-seven subjects (119 men and 38 women) were interviewed. Mean age of men was 41 years (± 14.2) and of women 35 years (± 10.7).
The lifetime prevalence of trauma among homeless people in inner Sydney and for the USA general population (percentages rounded) [6] is shown in Table 1.
Prevalence of lifetime trauma among homeless men (n = 119) and women (n = 38) in Sydney and in the USA general population
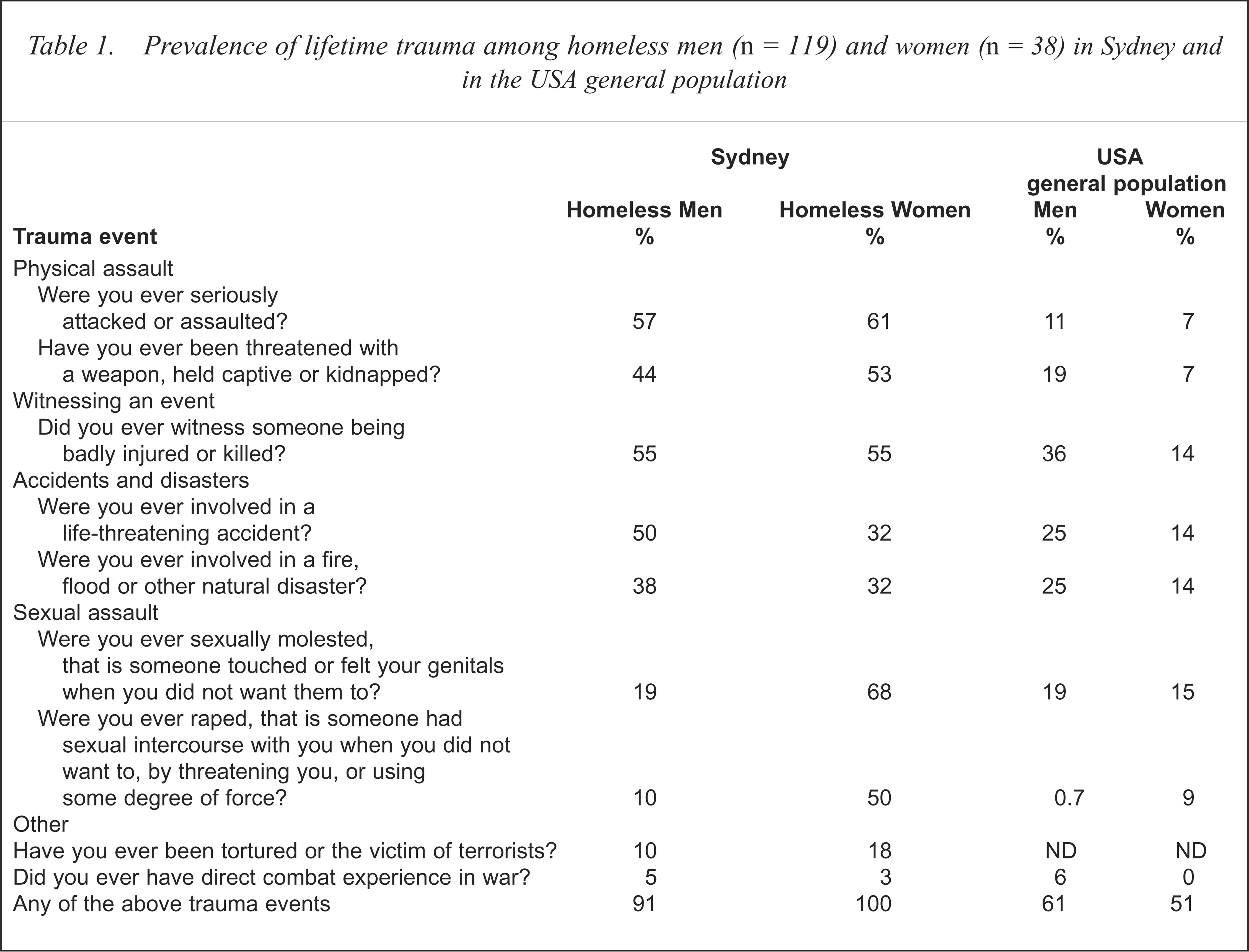
Among the homeless people in Sydney all women and over 90% of men had experienced a trauma event in their lifetime. They frequently reported more than one trauma. Half the women and 10% of men reported they had been raped. For men the experience of rape usually occurred in an institutional setting. Sexual assault (χ2 = 33.0, df = 1, p < 0.001) and rape (χ2 = 28.0, df = 1, p < 0.001) were significantly more frequent among women than men. There were no significant sex differences on any of the other items.
The experience of trauma among the homeless is substantially more frequent when compared with the USA general population [6]. Homeless men were at particular risk for lifetime physical assault and rape; homeless women at particular risk for lifetime physical assault, physical threats, witnessing a trauma event, sexual molestation and rape. Compared with the USA general population, homeless women appear to be at an eightfold risk of lifetime experience of physical threats and assault, while homeless men report a 15-fold increased risk of rape.
Discussion
Among the homeless in Sydney a lifetime event of trauma is almost universal. There are several possible reasons for such high rates. First, people who are homeless are frequently raised in a dysfunctional family or by a poorly coping single parent and in such a setting they are likely to witness or experience violence [10]. Second, some of our subjects as children or adolescents reported having been placed in institutions where physical or sexual abuse was experienced. Some possibly spent time in jail. Homeless youth have often spent time in an institution [10]. Third, during adolescence subjects may abscond from home, thereby placing themselves at further risk. In a study in London [10], half the homeless youth reported running away from home, often as a consequence of physical violence or sexual abuse. Adult homeless compared with non-homeless psychiatric patients are significantly more likely to have spent time in foster care or to have run away from home [11]. Fourth, childhood experience of abuse and family fighting are predictive of the experience of trauma in adults [3].
There are also current reasons for the high prevalence of trauma. At least one-quarter of the people who utilise refuges for the homeless have a diagnosis of schizophrenia [8]. Homeless men with schizophrenia, but not women, are vulnerable to trauma [3]. Other factors which are likely to render homeless people vulnerable to physical assault include alcohol and drug intoxication, the seeking-out of illicit substances, cognitive impairment and physical frailty. Finally the rates of trauma among homeless people are high because they spend many more hours than do others in a public space.
Homeless compared with domiciled young people are significantly more likely to have been sexually assaulted [10]. The majority of women and a substantial number of men in our study reported the experience of sexual assault. Childhood sexual assault may be an important early stressor predisposing to adult-onset depression and the greater the abuse the greater the risk [12]. Our female subjects reported sexual assault by parents, step-parents and siblings. These childhood experiences may be part of the explanation for the high rates of depressive disorders among the homeless in Sydney [8].
The prevalence of posttraumatic stress disorder (PTSD) among homeless people is high [13], and is usually present prior to the person becoming homeless [3]. We did not assess PTSD in our subjects, however, factors predisposing to PTSD were present. One is the experience of multiple traumas [14]. Homeless people in St Louis [3] reported multiple traumas, as did our subjects, and given their reports of almost universal experience of at least one trauma, the experience of multiple traumas is likely. Moreover, PTSD is more common in people with other psychiatric disorders [15]. In Sydney three in four homeless people have at least one mental disorder other than PTSD [8], a much higher rate than for the general population. Half the women reported having been raped; PTSD is especially common following rape [3]. Other factors, which are common in homeless people and which predispose to PTSD, include unmarried status, inadequate support systems, low socioeconomic level, recent stressful life changes and a history of childhood trauma [14].
There are limitations to the present study. It is not clear whether our subjects experienced trauma prior or subsequent to homelessness, or indeed whether trauma was the cause for homelessness. Furthermore at least one in four people interviewed were mentally ill; whether these people have a distorted memory of past trauma experiences remains to be established. What is clear is that a lifetime experience of trauma is common among homeless people and that a history of severe or repeated trauma may be relevant to current psychiatric morbidity.
Strategies to minimise these high rates of lifetime trauma need to target people who are at risk of homelessness. These strategies might include the early recognition and support of children who are being raised in a discordant family [16]. Support could be offered to adolescents and young adults who are incarcerated or about to be discharged from institutional care. Current strategies might include the recognition and assessment of trauma through education of health care workers and general practitioners and the establishment of on-site outreach mental health counselling services for people who access facilities for the homeless.