Abstract
Introduction
Considerable variations are observed of a “safe zone” for avoiding RLN injury during anterior cervical exposures. Most studies have attempted to accurately measure RLN versus the background of cervical vertebrae level. However all studies so far have not factored-in the unique embryology of RLN following the descent of the aortic arches. Thus, making it a floating structure separate from the bony spine. We aimed to measure the positional variation of this floating complex (RLN, Larynx, Esophagus) in fresh cadavers that are not yet fixed.
Methods
8 fresh cadavers were dissected to measure the point at which RLN on the right and left sides joined the tracheoesophageal groove TEG medially (considered safely protected) thence ascending to enter larynx. This was also measured against backdrop of the cervical level with neck in neutral and extension.
Results
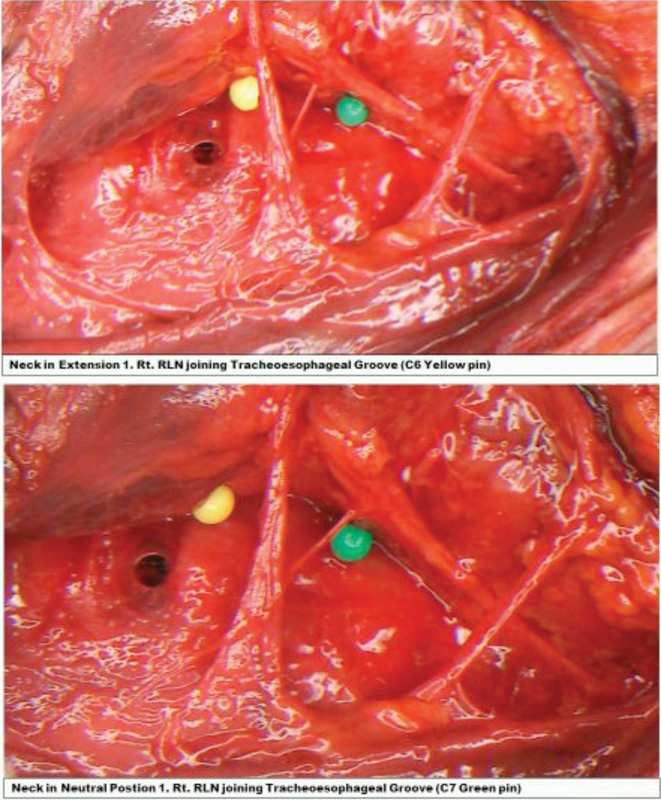
The RLN joins the TEG 4.45 cm vertically inferior to laryngeal prominence on the right and 7.7 cm on the left (Range of +/− 0.5 cm). There were significant variations of this point (RLN joining TEG) measured with neck in neutral and extension by ~1.8 cm (+/− 0.3 cm) (the length of one vertebral level (Photographed).
Conclusion
While the use of vertebral level landmarks may work well for nerve structures exiting or attached to the “fixed” spine, landmarking of a totally free floating nerve, such as the RLN is not practical. This nerve is closely related embryologically to that of the pharyngeal pouches and aortic arches and can undergo positional variation as described. Neck positioning during anterior cervical procedures can produce variations in the location of the recurrent laryngeal nerve. This is due to this structure as a “free floating nerve” and its different embryological origins (to the spine). The RLN joins the TEG ~4.5cm and 8 cm below the laryngeal prominence on the right and left sides respectively.