
Abstract
Introduction
The organization of the respiratory network has traditionally been described through descending medullary tracks. The diaphragm is innervated by the phrenic nucleus (C4-C6). However, the intercostal muscles are innervated by the intercostal motor nucleus (T1-T11) located at the thoracic spinal cord segments. Therefore, cervical spinal cord injury (SCI) can typically cause respiratory motor system dysfunction. From the literature, ventilation failure within the human lower cervical SCI population typically occurs 4.5 ± 1.2 days after injury, affecting 26.6% of patients. Also, the risk of apnea following low cervical SCI is increased during sleep. However, while intercostal muscles contribute to respiratory recovery post injury the pathways mediating this effect have never been fully elucidated.
Methods
Following complete C7 spinal cord transection in rats, we demonstrated the presence of intercostal-EMG activity synchronized to the inspiratory bursts of the diaphragm. We explored the anatomical, and latent, pathway that enables synchronized activation of the intercostal muscles after complete cord transection. Experimental work, in the form of bilateral dorsal/ventral rhizotomies, unilateral transection of the phrenic nerve and sympathetic chain ganglia and systemic application of salubutamol, suggested that intercostal activities is mediated through the sympathetic chain ganglion by means of connection to the ipsilateral phrenic nerve.
Results
In anesitised and unventilated rats, rhythmic inspiratory activity was present in the intercostal muscles following acute C7 transection and bilateral dorsal/ventral rhizotomies. This activity persisted up to five days following the initial trauma. Unilateral transection of the phrenic nerve and sympathetic chain ganglia eliminated ipsilateral intercostal motor activity. Systemic application of salubutamol (β2-agonist), not only increase intercostal activity but also restored it in transected rats which had not retained this activity following transection.
Conclusions
These data provide the first evidence of sympathetic nerve activity mediating synchronized and robust intercostal inspiratory muscle activity following severe, lower cervical transection. This activity occurs up to 5 days following trauma, an effect which correlates with the induction of ventilation failure and respiratory dysfunction in human patients with SCI. The clinical implications of this finding are provocative. 60% of patients undergo some degree of respiratory distress following acute C5–8 injuries. Using this pathway, it may be possible to modestly stimulate or activate sympathetic activity to further aid intercostal muscle activity and respiratory function following acute SCI. This thus represents a novel target for the treatment of respiratory dysfunction following spinal trauma.
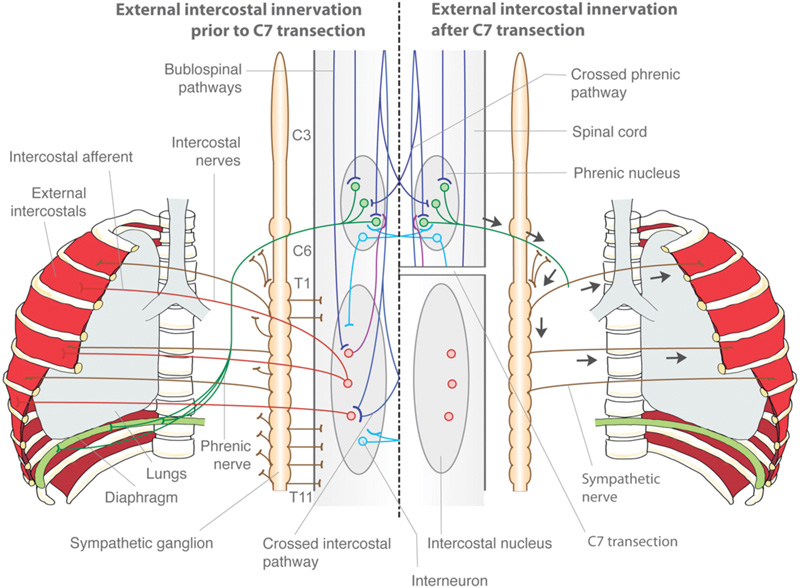
Diagram illustrated the phrenic-intercostal neuronal connections and circuits.