
Abstract
Introduction
The goal of arthrodesis is bone fusion, effected at the craniovertebral junction through onlay of either morselized iliac crest autograft (ICAG), or posterior structural unicortical ICAGbetween posterior elements. As an alternative, facet manipulation (FM) with C1-C2 or C0-C1 facet decortication and “jamming” of bone spacers into the articular space (C1-C2) has been described. We describe a series of 79 cases of surgical fusion of at least 1 component of the CVJ. FM was used in 65 cases requiring arthrodesis. Among these, we describe 14 cases using cages placed in the atlanto-axial joints (Cage assisted facet arthrodesis CAFA). To examine the efficacy of FM, we look specifically at CT documented fusion, and time to fusion using this technique.
Material and Methods
Retrospective review of medical records of 88 patients undergoing posterior arthrodesis of the craniovertebral junction (CVJ) at our unit from May 2004 to December 2013 was performed. 4 patients were excluded in case of early postoperative death (up to 30 days after the surgery). 5 patients had insufficient radiological follow-up data (follow-up < 6 months). Construct length is detailed in Table 1. Fusion – pseudarthrosis. Fusion was considered successful on CT if there was visible bridging trabeculations with or without bony remodeling and callus formation, across at least one of C1/C2 facets, and absence of pseudoarthrosis. Criteria for pseudoarthrosis were construct failure, or bone lucency around the screws. Time to fusion was defined as months between surgery and the earliest radiological assessment confirming solid fusion.
Results
Fusion rate and time to fusion. Sixteen patients were not considered for fusion analysis (N = 6 not grafted), or insufficient follow-up (N = 10). A solid fusion was achieved in 55 (87.3%) patients. Fusion rate was strongly associated with age.
Detailed construct length grouping in analyses
|
Construct length |
N (%) |
Group |
|---|---|---|
|
SA = subaxial. |
||
|
C0 – C1 |
2 (3%) |
C0 – Cx |
|
C0 – C2 |
5 (6%) |
|
|
C0 – CSA |
9 (11%) |
|
|
C1 – C2 |
50 (63%) |
C1 – Cx |
|
C1 – CSA |
3 (4%) |
|
|
C2 Direct |
3 (4%) |
C2 – Cx |
|
C2 – CSA |
7 (9%) |
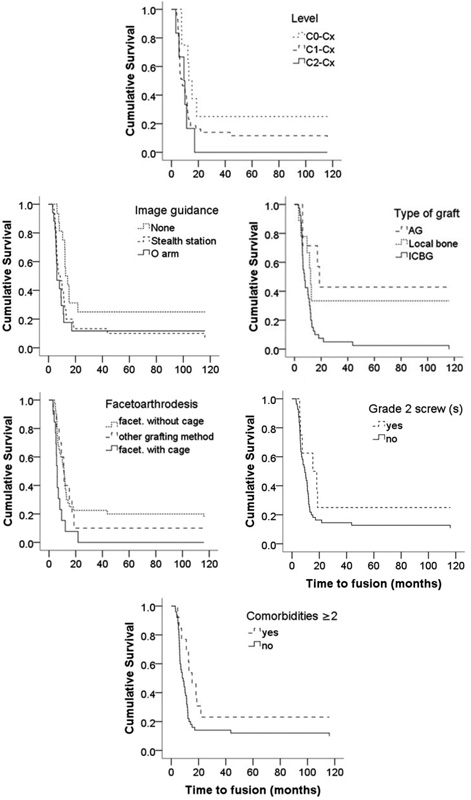
Kaplan-Meier probability of solid fusion in patients with C0-Cx, C1-Cx and C2-Cx surgery (upper), using Stealth station, O arm or without image guidance (2nd left), with allograft (AG), local bone and iliac crest bone grafting (ICBG) (2nd right), Facet manipulation C1-C2 with or without cage (3rd left), with or without grade 2 screw(s) (3rd right), and with or without multiple comorbidities (lower).
Conclusion
Many techniques are used to achieve solid bony fusion in the upper cervical spine. Facet manipulation, first described by Goel should be the ideal fusion bed but has not been widely used. We report our experience using FM as a fusion technique to highlight its usefulness as a primary means of achieving fusion. It exploits the weight bearing part of the spine, the volume of bone graft materiel is very small compared with other techniques, it can be used when there are no posterior elements. Cage assisted facet arthrodesis (CAFA) may accelerate time to fusion, and may enhance fusion rates.