Abstract
Introduction
The higher vulnerability of RLN in anterior approach to the cervical spine on the right versus left sides is the subject of ongoing debate. While most cadaveric studies have focused on in situ variations in course and local structural relations of the RLN as a suitable guide, they have mostly been done in preserved (fixed) cadavers or without relevance to the needs of spinal exposure.
Our aim was to perform surgically relevant exposures of the anterior cervical spine with particular attention to observing the potential vulnerabilities of the RLN on right and left side in fresh cadaveric specimens. In addition, we aimed to explore its branches.
Materials and Methods
12 cadavers had extensive layer by layer dissections by 2 surgeons (one with extensive experience as anatomy dissector). The RLNs and its branches were exposed in their entire length and explored for vulnerability. (Each stage was photographed)
Results
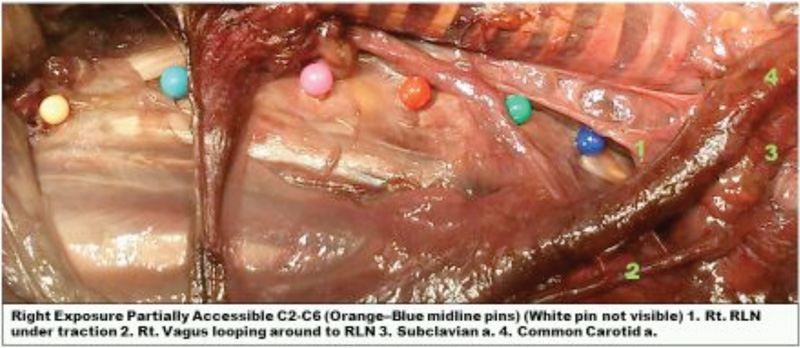
In all specimens, we demonstrated that right sided approach clearly causes undue stretch of the nerve and its branches particularly below C5 (photographed). The left side provided a good exposure without undue traction on the nerve. However, the terminal oesophageal branches of the nerve were especially vulnerable to this stretch or direct pressure on the left side.
Conclusion
Traction neuropraxia of the upper oesophageal branches of the RLN nerve may provide an alternative explanation for the transient post-op dysphagia (upto 60%). The laryngeal supply of the RLN benefits from Galen's anastomotic nerve supply of SLN (Ansa of Galen) and hence the neuropraxia of the nerve is less frequently symptomatic. Below C5, the left sided anterior cervical approach permits a wider access to the entire anterior cervical spine with less risk to the RLN. Neuropraxia induced on the oesophageal branches (directly by retractors or indirectly by traction) could provide a possible explanation for transient post-op dysphagia. We believe that this will help spinal surgeons to refine their surgical technique and thus reduce the incidence of iatrogenic injury.