
Abstract
Study Design
Retrospective cohort.
Objective
To clarify the sensitivity of C3–C2 spinolaminar line test as a screening tool for the stenosis of C1 space available for the cord (SAC).
Methods
Spine clinic records from April 2005 to August 2011 were reviewed. The C1 SAC was measured on lateral radiographs, and the relative positions between a C1 posterior arch and the C3–C2 spinolaminar line were examined and considered “positive” when the C1 ring lay ventral to the line. Computed tomography (CT) scans and magnetic resonance imaging (MRI) were utilized to measure precise diameters of C1 and C2 SAC and to check the existence of spinal cord compression.
Results
Four hundred eighty-seven patients were included in this study. There were 246 men and 241 women, with an average age of 53 years (range: 18 to 86). The mean SAC at C1 on radiographs was 21.2 mm (range: 13.5 to 28.2). Twenty-one patients (4.3%) were positive for the spinolaminar line test; all of these patients had C1 SAC of 19.4 mm or less. Eight patients (1.6%) had C1 SAC smaller than C2 on CT examination; all of these patients had a positive spinolaminar test, with high sensitivity (100%) and specificity (97%). MRI analysis revealed that two of the eight patients with a smaller C1 SAC had spinal cord compression at the C1 level.
Conclusion
Although spinal cord compression at the level of atlas without instability is a rare condition, the spinolaminar line can be used as a screening of C1 stenosis.
Introduction
The sagittal diameter of the cervical spinal canal is important, as a small canal diameter is associated with cervical myelopathy and with a high risk of spinal cord injury after trauma. 1 , 2 , 3 , 4 The majority of the published reports investigate the subaxial spine, and a sagittal canal diameter of 12 mm or less is regarded as stenotic. 2 , 3 , 5
There are few studies regarding stenosis at the level of the atlas, with little data existing to define a critical threshold for stenosis. 6 , 7 , 8 At the level of the atlas, the space available for the cord (SAC) is equal to the sagittal diameter of the atlas minus the dens diameter and ligamentous structures, with Steel's “rule of thirds” dictating that the dens, SAC, and spinal cord account for one third each of the contents of the C1 ring. 8 Atlantoaxial instability decreases the effective SAC and may be associated with myelopathy. In the absence of instability, hypoplasia and other congenital malformations of the atlas have been associated with myelopathy. 9 , 10 , 11 , 12 In most of these cases, this pathology is often associated with other skeletal abnormalities, such as spondyloepiphyseal dysplasia congenita and Down syndrome. 13 , 14 On the other hand, hypoplasia of the atlas causing spinal cord compression in the absence of instability or other skeletal abnormalities is rare, although there have been several case reports. 9 , 10 , 11 , 12 Given the relative rarity of this diagnosis, the diagnosis of stenosis at the level of the atlas may be missed or underdiagnosed.
The purpose of this study was to clarify the relative measurements of the SAC between C1 and C2. First, we investigated the sensitivity of the C3–C2 spinolaminar line as a reliable screening tool for the hypoplasia of C1 SAC on lateral radiographs. Computed tomography (CT) scans were used to analyze the detailed and relative measurements of C1 and C2 SAC, and magnetic resonance imaging (MRI) was used to identify cases of spinal cord compression to test the diagnostic value of the spinolaminar line rule.
Methods
This study was approved by the Institutional Review Board. The records of patients who underwent both CT scans and MRI of cervical spine at a cervical spine clinic of a single attending surgeon between April 2005 and August 2011 were reviewed. The patients presented with various cervical spine complaints, including neck or head pain, cervical spondylotic myelopathy or radiculopathy, disk herniation, and ossification of the posterior longitudinal ligament. Patients with rheumatologic disease (e.g., rheumatoid arthritis), congenital deformities (e.g., Klippel-Feil), and prior surgeries were excluded. Patients with histories of cervical trauma, infection, or tumor were excluded. Patients with instability between C1 and C2 or with congenital defects of the posterior arch of the atlas were also excluded.
The SAC of the atlas was measured on neutral, lateral radiographs using digital radiographs, with a correction for magnification by 10%. The C1 SAC was defined as the distance from the posterior border of the dens to the ventral C1 lamina. Also, the C3–C2 spinolaminar line was drawn, beginning at C3 and extending cranial through C2 to the lamina of C1 (Fig. 1). When the ventral lamina of C1 lay ventral to this line, the spinolaminar test was defined as positive, which indicated the possibility of existence of a relatively narrow SAC of C1. The dimensions of the atlas, dens diameter, atlantodental interval (ADI), and C1 SAC were measured using CT scans. The MRI evaluation included measurements of the spinal cord diameters at C1 and C7 levels on T2-weighted images as well as checking the existence of spinal cord compression. The images investigated were taken in digital imaging formats, and all the measurements were made using the digital data.
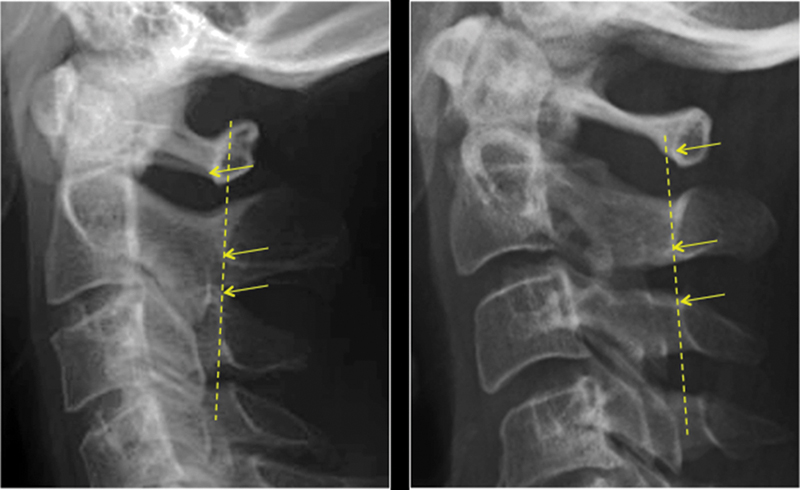
Posterior wall of C1 spinal canal lies ventral (left; top arrow) or dorsal (right; top arrow) to the spinolaminar line (dotted line) from C3 and C2.
The independent samples t test was used to compare the means between the groups. Pearson's correlation coefficient was used to measure the correlation between the continuous variables. Interobserver reliability was evaluated using the kappa coefficient. The sensitivity and specificity of the spinolaminar line rule was calculated using CT measurements as the gold standard for C1 and C2 SAC. The calculations were performed using SPSS 17 software (SPSS, Chicago, Illinois, United States). Statistical significance was defined as p < 0.05.
Results
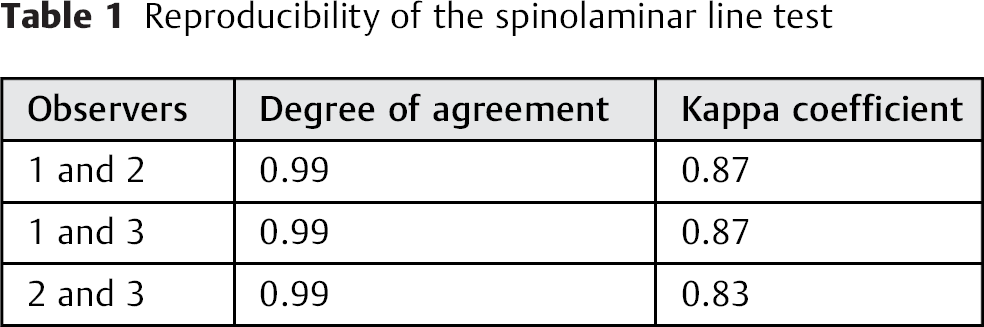
Of the 570 patients identified in the specified period, 487 patients met the inclusion criteria. A sample of this size is appropriate for a population larger than 264 million, assuming a 5% margin of error. 15 There were 246 men and 241 women, with an average age of 53 years (range 18 to 86). The mean SAC of the C1 canal on plain lateral radiographs was 21.2 mm (standard deviation [SD]: 2.2 mm, range: 13.5 to 28.2; Fig. 2). The mean diameter was 21.5 mm (SD: 2.3) in male subjects and was 20.9 mm (SD: 2.0) in female subjects (p = 0.01). Twenty-one patients (4.3%) had a C1 ring ventral to the C3–C2 spinolaminar line (i.e., positive for the spinolaminar line test); all of these patients had C1 SAC of 19.4 mm or less (Fig. 2). The interobserver reliability of this line was considered to be excellent (Table 1).
Reproducibility of the spinolaminar line test
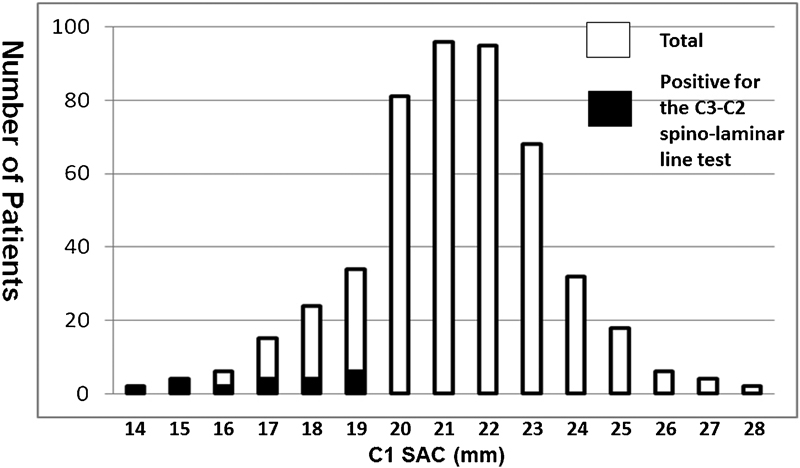
Distribution of C1 space available for the cord (SAC) on lateral X-ray.
The CT scans of all 85 patients (17.5%) with C1 SAC < 19.4 mm or less on plain lateral radiographs were analyzed further. The C1 SAC on the CT scans was ~89% of that on radiographs, with a coefficient of 0.82, which was considered reasonable given that the radiograph was magnified by 10%. Of these, 8 patients (8/487, 1.6%) had C1 SAC smaller than C2 SAC, and all 8 had a positive spinolaminar line screening test. The sensitivity and specificity of the spinolaminar line test to detect a relatively small C1 SAC were 100 and 97%, and the positive and negative predictive values were 38 and 100% (Table 2).
Relationship between the screening by the spinolaminar line on X-rays and C1 stenosis compared with C2 defined by CT
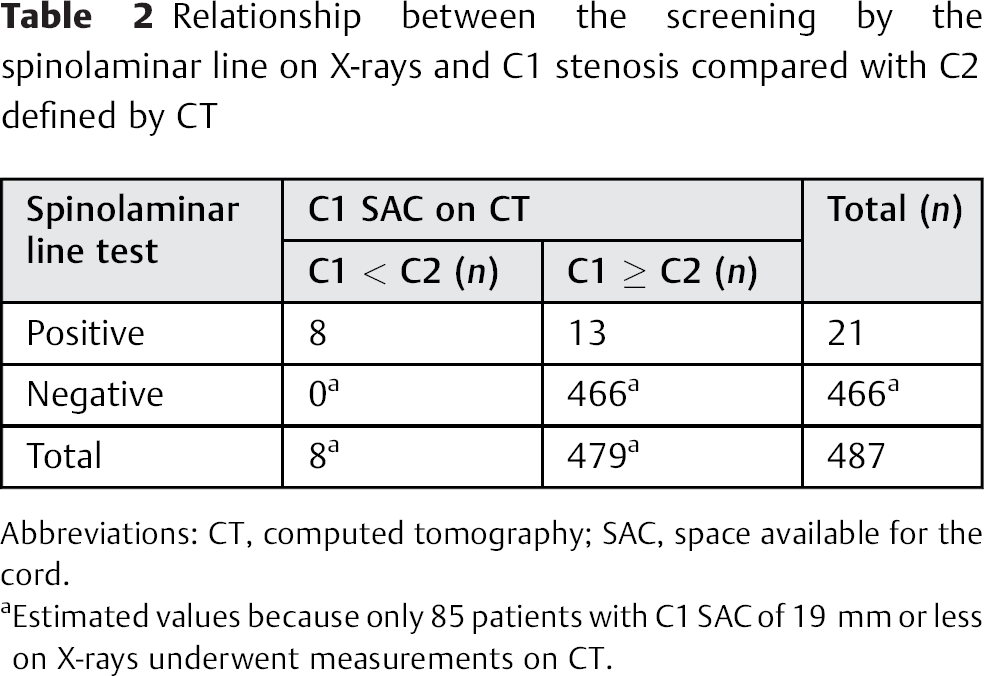
Abbreviations: CT, computed tomography; SAC, space available for the cord.
Estimated values because only 85 patients with C1 SAC of 19 mm or less on X-rays underwent measurements on CT.
MRI analysis revealed a significantly larger spinal cord diameter at C1 (average 7.7 mm, SD 1.2) versus C7 (average 6.2, SD 1.2; p < 0.01). Four of the 8 patients with a smaller C1 SAC had effacement of the subarachnoid space including 2 patients with spinal cord compression at the C1 level; all these patients had C1 SAC smaller than 13.0 mm on CT. In contrast, no patients showed evidence of cord compression or effacement of the subarachnoid space when the C1 SAC was larger than C2.
Discussion
This study was undertaken to examine the value of the spinolaminar line rule at C1–C2 and to investigate the relative diameters of C1 SAC and C2 in relation to spinal cord compression. We found that the spinolaminar line is an effective, simple screening test, with a high sensitivity (100%), specificity (97%), and negative predictive value (100%).
Hinck and Sachdev first described developmental stenosis of the cervical spinal canal on the subaxial levels, which is now familiar among spine surgeons. 1 On the other hand, few case reports have documented small C1 ring as a cause of myelopathy. Therefore, one may overlook this relatively rare condition, especially when the patient has a normal measurement of ADI.
The C3–C2 spinolaminar line test is a simple screening tool that can be performed quickly in the clinic with lateral plain radiographs. In this study, a positive spinolaminar line test excluded all the patients with C1 SAC larger than 19.5 mm as well as those without spinal cord compression at the level of the atlas. Compared with the 4.3% of patients who had a positive C3–C2 spinolaminar line test, only 1.6% had a C1 SAC smaller than C2 on CT. We speculate that the difference may result from inaccuracy of the X-rays. The determination of the posterior wall of the spinal canal may vary, and therefore the spinolaminar line is somewhat subjective. Nevertheless, we believe that the spinolaminar line meets the criterion for a screening test in that it appears to be sensitive. Indeed, all patients with a C1 SAC smaller than C2 were detectable by this simple screening test, including those with spinal cord compression.
There have been few reports as to the relative diameters of C1 SAC. Gupta et al performed a radiographic study of 300 normal Indians and reported that the mean SAC of C1 was 21.43 mm in male and 20.13 mm in female subjects, compared with the mean C2 SAC of 19.66 mm in male and 18.60 mm in female subjects. 16 Although the results were almost similar with those in our study, they did not mention the relative measurements of C1 versus C2 SAC. From our study, the relatively small C1 SAC compared with C2 was seen in only 1.6% of the patients, which indicates the rarity of this condition.
As for cervical spine stenosis below C3, diameters of less than 12 mm are reported to be related to the high incidence of compression myelopathy. 2 Given that the diameter of the spinal cord at C1 level was 1.5 mm larger than that of C7 level, it is reasonable that the C1 canal diameter of 13.0 mm is potentially pathologically narrow. If one considers a normal ADI (2 mm), 17 then the C1 SAC may be even smaller and more likely to be pathologic.
Although we excluded the cases with congenital anomalies and focused on cases without hypoplasia of the atlas, Senoglu et al reported that congenital anomalies of the atlantal arch were found in 2.95% of 1,354 evaluated subjects, most of whom were asymptomatic. 18 Needless to say, we should also pay attention to such rare cases.
There are several limitations in this study. This study suffers from selection bias, as all the patients were evaluated in a cervical spine clinic and underwent CT and MRI scanning for concern of some pathology. As such, our measurements may be smaller than those of asymptomatic individuals. Second, we did not investigate the CT analysis in all the cases but focused on patients screened by plain radiographs. However, the correlation between plain radiographs and CT scans is high, and we do not think we excluded patients suitable for further study. We feel our sample size, 487, is appropriately large to make estimates for the population on the whole.
In conclusion, few patients (1.6%) had a smaller SAC of C1 than that of C2, and all of these patients had a positive spinolaminar line test. Although spinal cord compression at the level of atlas without instability is a rare condition, the spinolaminar line test is a simple screening test for C1 stenosis.
Disclosures
Yasushi Oshima, none
Michael P. Kelly, Grant: Cervical Spine Research Society
Kwang-Sup Song, none
Moon Soo Park, none
Tapanut Chuntarapas, none
Katie D. Vo, none
Jin S. Yeom, Teaching arrangements: Medtronic (honoraria for cadaver workshops)
Katsushi Takeshita, none
K. Daniel Riew, Grant: AOSpine, Cerapedics, Medtronic; Speakers’ bureau: AOSpine, NASS; Royalties: Biomet, Medtronic, Osprey, Medyssey; Stocks: Expanding Orthopedics, Amedica, Benvenue, Nexgen Spine, Osprey, Paradigm Spine, Spinal Kinetics, Spineology, Vertiflex, PSD, Medyssey; Travel expenses: AOSpine, NASS, SRS, Broadwater, Selby Spine; Board membership: CSRS, AOSpine International, Global Spine Journal, Spine Journal, NASS
Footnotes
Note
Research was performed at Washington University School of Medicine. Institutional Review Board (IRB) approval was received for this study.