
Abstract
Study Design
Case report.
Objective
Merkel cell carcinoma is an aggressive neuroendocrine carcinoma with a poor prognosis. Metastatic epidural spinal cord compression (MESCC) is a debilitating disease causing neurologic deficits. The surgical management for MESCC depends on pathology.
Methods
We report a case of Merkel cell carcinoma of the spine and evaluate the treatment paradigms utilized in the prior reports.
Result
A 76-year-old man with a history of Merkel cell carcinoma presented with 2-week history of progressive difficulty ambulating and a solitary T5 epidural mass encasing the spinal cord. The patient underwent a T5 corpectomy with cage placement and T3 to T7 posterior fusion with postoperative neurologic improvement and a return to ambulation. Three weeks postoperatively, the patient re-presented with new-onset weakness and widespread metastatic spinal disease with epidural compression at the T8 level. Six weeks postoperatively, he was placed in hospice care.
Conclusion
Prior reports in the literature demonstrated a poor prognosis for Merkel cell carcinoma metastasis to the spine with survival ranging from 1 to 9 months after diagnosis. Although neurologic decline necessitates a surgical intervention, the assessment of operative benefit should take into account the prognosis associated with the primary tumor subtype.
Introduction
Merkel cell carcinoma (MCC) is a rare neuroendocrine malignancy of the skin, initially named after Friedrich Merkel in 1875. Although Merkel's description of this tumor subtype was based on a description of moles, 1 the true pathologic diagnosis was ultimately defined as a “trabecular carcinoma of the skin” almost 100 years later by Cyril Toker in 1972. 2 The name is derived from the neurosecretory granules in the tumor cells that likely originate from the neural crest, derivative of Merkel cells. 3 After Toker's description, the number of MCC cases reported increased substantially, with an incidence of 44 per 100,000. 4 MCC is more common in Caucasians (∼94%), older populations (average age of ∼72 years), and males (men are two times more likely to be diagnosed than women). 5 , 6 The most common location in tumor diagnosis is the head and neck, followed by the trunk and extremities. Fifty-two percent of the patients have regional lymph node involvement at initial diagnosis, and 34% of this patient population presents with distant metastases. 7 MCC has 5-year relative survival rates for localized, regional, and distant MCC of 75, 59, and 25%, respectively, with a mortality rate of ∼33% (nearly twice that of metastatic melanoma). 5 , 8
There are currently six reports in the literature of MCC causing metastatic epidural spinal cord compression (MESCC) with four reports demonstrating survival of 1 to 4 months after surgical decompression and stabilization with or without chemotherapy and/or radiation. 9 , 10 , 11 , 12 , 13 , 14 Here we review the literature on MCC causing MESCC, and we present the seventh case of MCC metastasis to the spine causing MESCC.
Case Report
Preoperative
A 76-year-old man was diagnosed with MCC after biopsy of a skin lesion on his left upper back over the scapula. He subsequently had a wide excision, and a sentinel lymph node biopsy 2 months later revealed a 2.8-cm tumor and 4/8 lymph nodes were positive. He underwent complete axillary dissection 3 months after the diagnosis, followed by adjuvant external radiation therapy over the left scapula with a total dose of 50 Gy in 200-cGy fractions, which ended 5 months after the diagnosis. He developed a recurrent tumor in the left axilla and the left anterior chest 10 months after the diagnosis. The patient underwent resection of these tumors 11 months after the diagnosis followed by 68 Gy of radiation therapy that was completed 14 months after the diagnosis. Prior to the admission for MESCC, the patient ambulated with a walker at baseline and used an ankle foot orthotic on his left side for residual hemiparesis from a stroke in 1989.
Hospital Course
The patient presented to the emergency room with right lower extremity weakness and difficulty with ambulation resulting in several falls over a 1- to 2-week period 16 months after initial diagnosis. He denied trauma, numbness, tingling, paresthesias, or urinary/bowel dysfunction. On neurologic exam, the patient's left lower extremity motor strength was 1 to 2/5 throughout, and the right lower extremity was 4/5, with upgoing toes and hyperreflexia. An MRI demonstrated a T5 solitary epidural mass encasing and compressing the spinal cord that extended into the paraspinal muscles bilaterally, left greater than right, focused at the T5 vertebral body and extending from the midlevel of T4 with neural foraminal invasion to the middle of the T6 vertebral body (Fig. 1). The patient underwent a T5 transpedicular approach for an intralesional resection through a corpectomy with cage placement and a T3–T7 posterior spinal fusion because the bony destruction involved the entire vertebral body and posterior neural elements encasing the spinal cord (Fig. 2). Postoperatively, the patient's motor exam improved to 3/5 in his left lower extremity (baseline from a previous stroke) and 5/5 strength in the right lower extremity, and he was able to ambulate with a walker again. Pathologic examination demonstrated a metastatic neuroendocrine tumor consistent with his prior diagnosis of MCC.
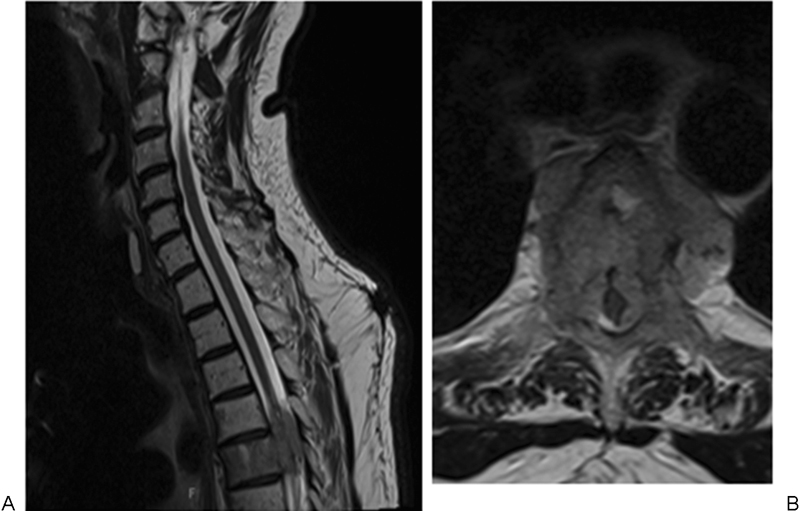
(A) Sagittal and (B) axial magnetic resonance imaging demonstrating a metastatic Merkel cell carcinoma tumor involving the vertebral body and encasing the spinal cord.
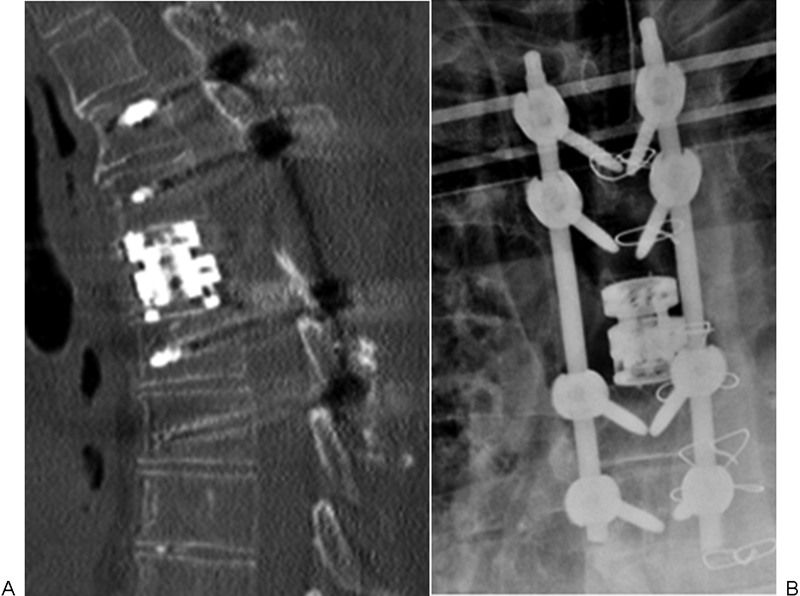
(A) Sagittal computed tomography scan and (B) thoracic spine radiograph demonstrating a T5 corpectomy and cage placement with T3–T7 posterior fusion.
Postoperative
Three weeks postoperatively, as the patient was to begin postoperative radiation treatment, he developed new-onset weakness in his bilateral lower extremities. MRI of the thoracic spine revealed new sites of metastatic disease at T2–T3 and T6–T11 with epidural compression at the T8 vertebral body. After discussion with the family, the patient was admitted to hospice care 6 weeks after his surgery.
Discussion
MESCC is found in 5 to 10% of patients diagnosed with spinal column metastases and is associated with progressive disability secondary to the compression of the neural elements. Decompressive surgery combined with radiation is the standard treatment for the tumors that are not highly radiosensitive and is shown to increase the efficacy in preserving neurologic function and to improve ambulation when compared with radiation therapy alone. 15 , 16 The factors associated with a longer survival in patients with MESCC were the ability to walk before and after therapy, 17 , 18 , 19 a single site of epidural cord compression, 20 a radiosensitive tumor histology, 17 , 18 and no visceral or brain metastasis. 21 Here we present a case of MCC metastatic to the thoracic spine that had several factors consistent with a favorable prognosis and prolonged ambulatory status including a single site of epidural cord compression on presentation, radiosensitive tumor histology, and no evidence of visceral or brain metastasis on presentation. Based on prior studies of metastatic disease to the spine, one could predict that the patient presented should have a more prolonged ambulatory status and possibly an improved prognosis; however, despite the favorable factors previously mentioned, the patient developed progressive lower extremity weakness secondary to metastatic progression of his primary tumor.
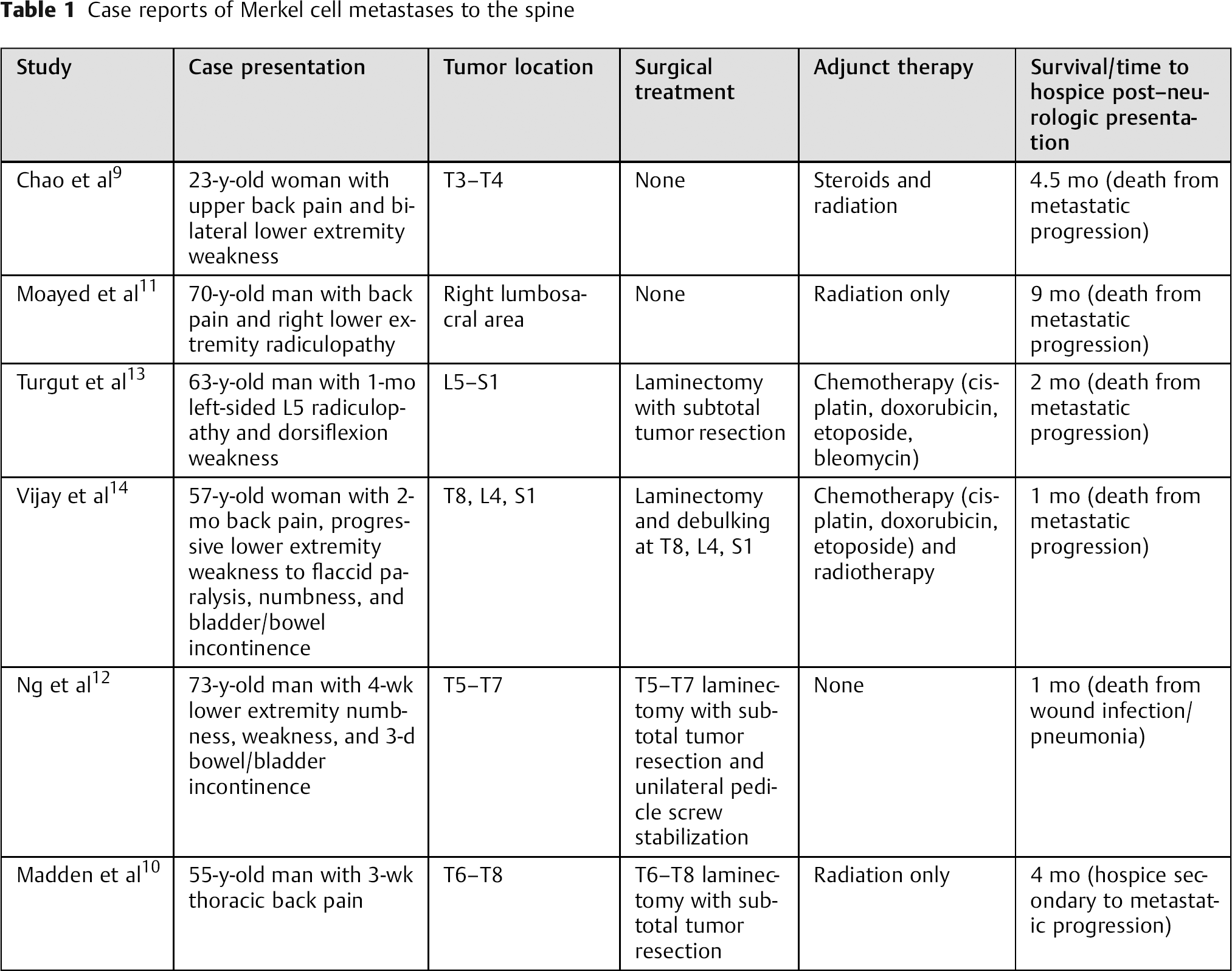
All of the prior cases of MCC metastasis to the spine demonstrated poor survival consistent with the study performed by Allen et al (Table 1). 9 , 10 , 11 , 12 , 13 , 14 , 22 In their review of 251 patients diagnosed with MCC, 14 of whom presented with distant metastasis, Allen et al found that the 2-year survival rate was 11% with a 9-month median survival. 22 The ability to predict the survival of patients with metastatic disease is critical in determining a management strategy. Certain groups advocate for a greater than 3-month prognosis before recommending operative therapy, 23 although others recommend greater than 6 to 7 months. 24 , 25 Although the “prognosis threshold” varies within the literature, the primary tumor subtype appears to be the most paramount factor in determining the patient prognoses before an operative intervention should be considered. 15 , 25 In the six prior reports of MCC metastasis to the spine, by the time the primary tumor was detected in the spine, the prognosis was 9 months or less with an average survival of 3.5 months (5 of 6 patients died within 4 months; Table 1). 9 , 10 , 11 , 12 , 13 , 14 Given the dismal prognoses associated with rarer tumors such as MCC, further studies are needed to determine the most appropriate cutoff when operative intervention should be considered.
Case reports of Merkel cell metastases to the spine
In conclusion, MESCC caused by MCC is rare with six reported cases in the literature. 12 , 13 , 14 We report the seventh patient with MCC metastases to the spine and the fourth case showing neurologic decline in the setting of MESCC requiring decompressive surgery. This is the first case of MCC that encased the spinal cord causing both anterior and posterior bony destruction that necessitated corpectomy with cage placement and posterior stabilization. In ambulatory patients presenting with spinal metastasis, a metastatic workup with a needle biopsy is the first-line treatment. Acute neurosurgical decompression is the standard of care in patients presenting with a progressive decline in motor strength, ambulatory status, and/or bowel/bladder dysfunction. With such poor survival rates for patients diagnosed with MCC, although neurologic decline warrants aggressive treatment, the risks and benefits of a surgical intervention must be carefully considered. In certain tumor subtypes, the primary end point of ambulatory status may not be as useful in assessing whether surgical intervention is beneficial, and further studies are needed to determine the appropriate management paradigm for patients diagnosed with rarer metastatic primary tumors.
Disclosures
C. Rory Goodwin, none
Ankit I. Mehta, none
Owoicho Adogwa, none
Rachel Sarabia-Estrada, none
Daniel M. Sciubba, none