
Abstract
Introduction
The patient was a 37-year-old man who was a victim of a motor-vehicle accident. On arrival at the emergency department, the patients’ vital signs were all within normal physiological range. His GCS was 15/15. He had suffered from neck pain. In physical examination, he had upper cervical spine tenderness but there was no abnormal palpable deformity. Other physical examinations were normal. Plain X-ray of the cervical spines was nonconclusive. Cervical-spine CT scan demonstrated an isolated unstable Jefferson fracture associated with Spence's criteria. Cervical CT angiography was normal.
Materials and Methods
The patient was placed in the prone position and the alignment and the position of the atlantoaxial complex was verified by the use of real-time fluoroscopy. The cervical spine was exposed subperiosteally from the occiput to the level of C3-4. The C1-2 articulation was exposed. After the dorsal root ganglion of C2 was retracted inferiorly, the middle of the junction of the posterior arch of C1 and the midpoint of the inferoposterior part of the C1 lateral mass was exposed. The screws were placed via Magerl trans-facet screw technique. Then screws were connected with a rod and nuts to reduce lateral spread of the lateral masses.
Results
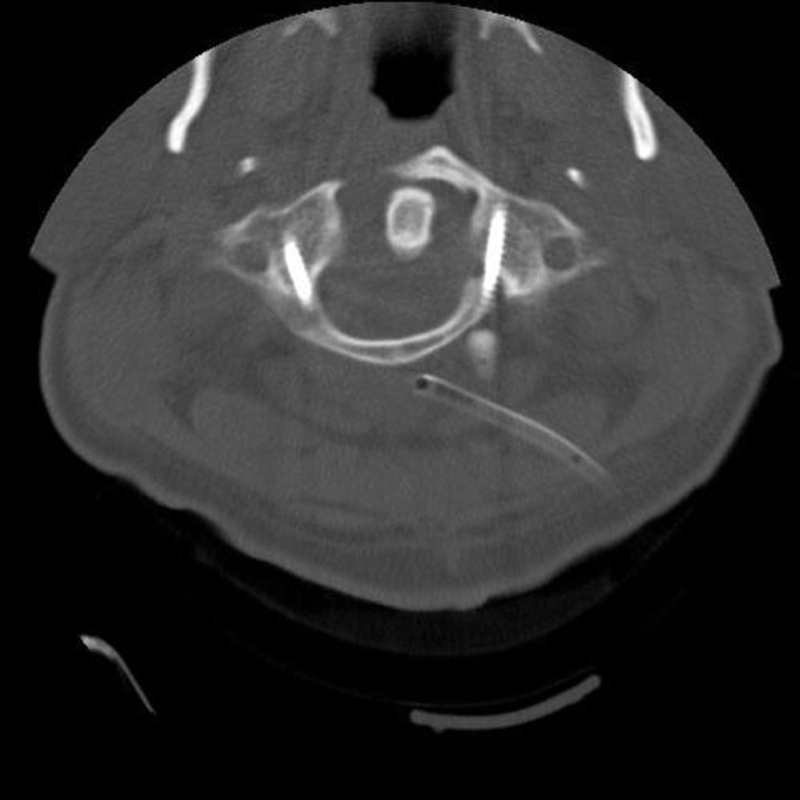
Postoperative cervical CT scan showed that the screws are in favorable position.
Conclusion
The treatment of unstable Jefferson fractures remains controversial. Conservative treatment usually associates with the longtime of immobilization in halo vest, whereas conventional posterior surgical treatments generally eliminate the range of motion of the upper cervical spines. With the posterior intersegmental fusion of unstable atlas fracture, the stabilization of anterior arch of atlas can be achieved while at the same time atlantoaxial rotation is preserved.
None declared