
Abstract
Study Design
Case report.
Objective
Present a case of Foix-Alajouanine syndrome that presented as acute cauda equina syndrome and discuss the pathophysiology and management.
Methods
An adult male patient developed sudden onset of back pain and leg pain with weakness of the lower limbs and bladder/bowel dysfunction typical of cauda equina syndrome. Emergency magnetic resonance imaging revealed no compressive lesion in the spine but showed tortuous flow voids and end-on blood vessels in the peridural region suggesting spinal arteriovenous malformation resulting in Foix-Alajouanine syndrome.
Results
The case was managed by endovascular embolization with excellent results. The pathophysiology, imaging features, management, and literature review of the syndrome is discussed.
Conclusion
The authors conclude that this condition may be an important differential diagnosis for cauda equina syndrome.
Keywords
Introduction
Acute onset of low back pain, bilateral lower limb radiation, and sensory, motor, and reflex changes in the legs along with bladder and bowel dysfunction accompanied by perianal sensory loss are considered characteristics of cauda equina syndrome (CES). 1 Typical differential diagnosis includes compressive spinal lesions like acute central disk prolapse, spinal stenosis, intra- and extradural tumors of the spine, spinal infections, fractures, cystic lesions, hemorrhage and hematoma, arachnoiditis, as well as noncompressive lesions like demyelinating diseases of the cord. 2 , 3 Occasionally Guillain-Barré syndrome or transverse myelitis can present as CES. A variety of rare causes like Susac syndrome and several interventions like epidural and spinal injections have been described in literature as causing acute onset of neurologic changes mimicking CES. 3 , 4 Intradural arteriovenous malformations of the spinal cord are well-described conditions in the neurosurgical literature, and the syndrome of ischemic myelopathy described as Foix-Alajouanine syndrome is a well-known entity. 5 However, the syndrome presenting as cauda equina compression has not been hitherto described to the best of our knowledge.
Case Report
A 42-year-old man presented to the emergency department with sudden onset of severe low back pain, bilateral lower limb radiation, paresthesia, inability to walk due to lower limbs weakness of 3 days’ duration, which rapidly increased from onset. He also complained of urinary incontinence, constipation, and numbness around the perianal region. He had no history of recent trauma, fever, or systemic manifestations of illness or known medical comorbidities. He had been having occasional low back pain for the previous 1 year.
On examination at the time of admission, he appeared to be an obese man with stable vital parameters and had lower limb weakness with the left side worse than the right. The ankle dorsiflexion, toe extension, and flexion on the left were 2/5 (Medical Research Council grade) and the knee was 3/5. On the right side, the toes, ankle, and knee were grade 3/5 in both extension and flexion. He had absent knee and ankle jerks bilaterally and sensory hypesthesia over L5 and S1 dermatomes bilaterally. He also had saddle anesthesia and lax anal tone. His Babinski reflex was flexor on both sides. His upper limbs were neurologically intact.
On admission, the basic blood results are within normal limits including the inflammatory markers, serum folate, and vitamin B12 levels and bone profile. Blood cultures were negative. A clinical diagnosis of CES was made and injection of dexamethasone was started as emergency treatment while the patient was kept fasting in anticipation of surgery for spinal decompression. An urgent X-ray and magnetic resonance imaging (MRI) of the lumbosacral spine were done.
The X-ray of the lumbosacral spine was within limits of normalcy. The MRI of the region was also essentially normal with regard to the disks and spinal canal. However, there was an abnormal ill-defined hyperintensity of the distal spinal cord involving the conus medullaris predominantly from T9 to L2 on the T2-weighted image. Tortuous flow voids and thin vascular channels were noted in the sagittal T2-weighted images within the thecal sac as well as anterior and posterior aspects of the conus and distal cord, which suggested an arteriovenous malformation (AVM) of the spinal cord (Figs. 1 and 2). MRI with contrast also confirmed these findings. The patient also underwent urgent electrophysiologic studies (electromyography study and nerve conduction study), which were considered normal. No cerebrospinal fluid studies were undertaken at this stage.
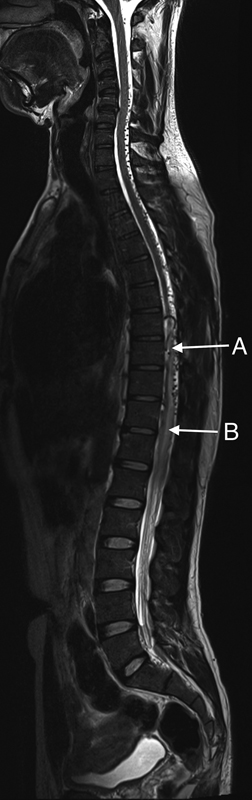
T2-weighted magnetic resonance image illustrating extensive spinal arteriovenous malformations in the cervical, thoracic, and lumbar spinal cord. Arrow A demonstrates the end-on view of the leash of vessels, and arrow B highlights the edema in the conus medullaris.
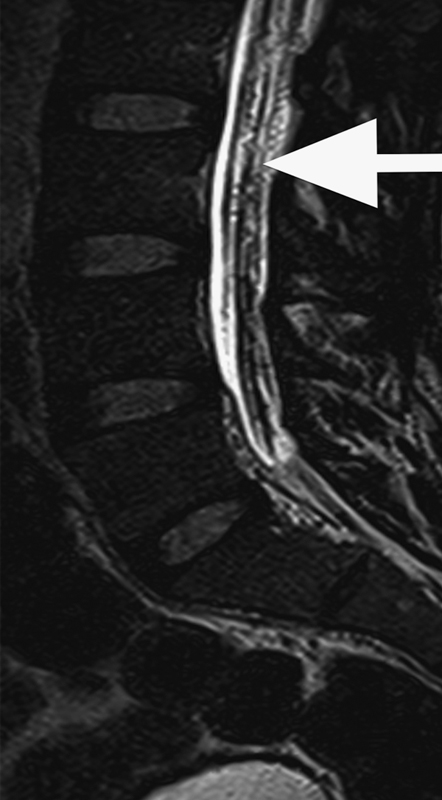
T2-weighted image of the lumbar spine. Please note the absence of bony, disk, or soft tissue compression of the neural tissues. Serpentine flow voids are highlighted by the arrow.
A diagnosis of intradural AVM resulting in venous hypertension and cord edema of the conus medullaris (Foix-Alajouanine syndrome) was made. The patient was maintained on steroids and nonsteroidal anti-inflammatory drugs while he was awaiting angiographic studies and endovascular embolization. He was transferred to a neurosurgical facility in Cairo, Egypt at his request. While under neurosurgical care in his native country, the patient started to complain of progressive tightness in both lower limbs, and examination revealed hyperreflexia and spasticity with increased muscle tone in both lower limbs. His sensory dysesthesias had significantly diminished by then. All the imaging and neurophysiologic studies were repeated (2 to 3 weeks from the original study). The MRI remained essentially the same but the electrophysiology now suggested upper motor neuron lesion of both lower limbs associated with decreased amplitude of the somatosensory evoked potentials—a picture of dorsal myelopathy and epiconus lesion. The H-reflex was normal and there was no evidence of peripheral neuropathy. His bulbocavernosus reflex (S2, 3, 4) was also normal at this stage. Urodynamic study revealed a neurogenic bladder. Spinal angiography was done and confirmed the AVM. During this entire period, the patient was on regular dose of dexamethasone (4 mg thrice daily), neurotropic drugs, nonsteroidal anti-inflammatory drugs, and drugs for urinary incontinence.
A week after the angiographic spinal procedure, the patient improved remarkably and was able to walk and soon returned to his normal daily activities with resolution of most of his symptoms. He returned to his original employment 3 months after onset of symptoms. When last reviewed 3 months after the confirmed diagnosis, he was completely pain-free and had minimal numbness in the legs with normal neurologic examination of the legs. However, he continued to be incontinent with regard to his bladder function and also constipated with some residual saddle anesthesia.
Discussion
Foix-Alajouanine syndrome is a well-known clinical entity in the neurosurgical circuits, 5 , 6 though perhaps less well known to orthopedic spine surgeons. The importance of this condition is that it can present with acute onset of neurologic dysfunction reminiscent of CES due to lumbar disk prolapse. Charles Foix and Théophile A. J. Alajouanine originally described the condition in French literature in 1926, though the pathophysiology was not unraveled until many years later. 5 This syndrome is not a distinct entity but is considered a sequel of spinal AVM that was caused by thrombosis within the abnormal vessels of the spinal cord. The pathophysiology is described as a subacute myelopathy due to venous congestion of the spinal cord in the absence of hemorrhage in a patient with a spinal AVM. 7 , 8 The vascular anatomy of the spinal cord has been reviewed in detail by Takai and Taniguchi. 9 The anterior spinal artery is described as communicating with the radiculomedullary artery, and the corresponding veins also have similar anastomosis, with the venous network being far more extensive and connecting to the extradural and extravertebral veins as well (Fig. 3). Anomalous communication between the radiculomedullary artery and vein results in significant pressure rise in the communicating venous network. The typical pathophysiology of the disease consists of venous congestion in the spinal cord, leading to progressive ischemia and infarction. Thrombosis is also often an accompaniment in this lesion. Rosenblum et al differentiated dural arteriovenous fistulas and intradural AVMs based on their review of 81 patients. 10 In intradural AVM, 50% present in the acute form, and hemorrhage commonly accompanies clinical deterioration. On the other hand, dural AV fistulas typically cause progressive myelopathy and only 10 to 15% present as acute-onset neurologic deficit. 10 Criscuolo et al also reported the pathologic sequence of venous stasis, congestion, and edema as the essential mechanism before thrombosis sets in. 11 Several classifications have been offered for spinal AVMs, 6 , 12 but all have been subject of debate and disagreement. The Bicetre grouping into the genetic-hereditary, genetic-nonhereditary, and sporadic is one of the more accepted schemas. They have also been grouped according to their location as ventral, dorsal, and lateral. Kim and Spetzler have also made an elaborate classification based on the relationship with the meninges and the location and have added a conus medullaris lesion as a distinct entity. 13
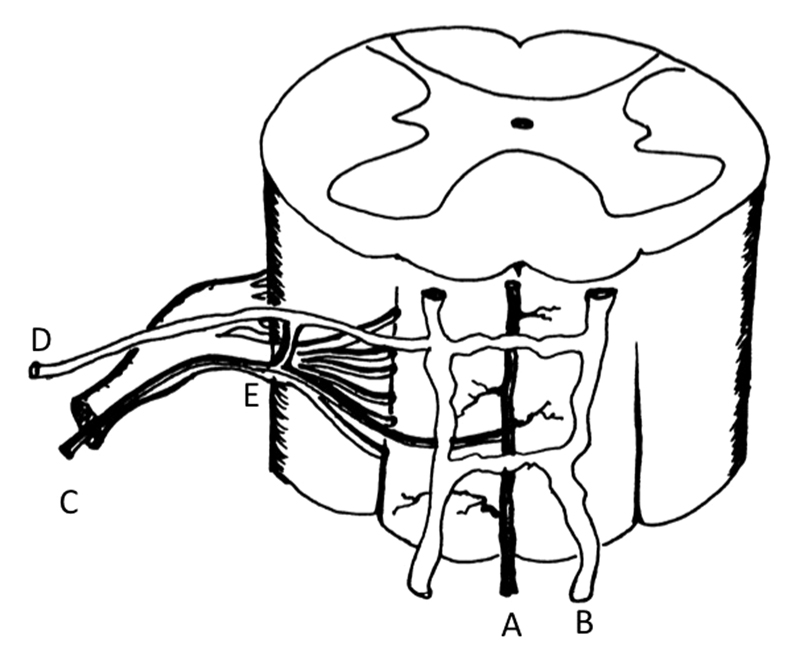
Diagrammatic representation of the arteriovenous network on the spinal cord. (A) Anterior spinal artery. (B) Anterior spinal veins. (C) Radiculomedullary artery. (D) Radiculomedullary vein. (E) Abnormal arteriovenous communication.
Several clinical presentations have been described for spinal AV fistulae, and Muralidharan and coworkers have recently described their experience with 153 patients. 14 About half of their patients presented with leg weakness, 20% had back pain, and 27% had sensory abnormalities. Interestingly, sphincter disturbances were seen only in ∼4% of their cases.
The diagnosis of dural AV fistulas is essentially radiologic and can be made by MRI, which typically shows swelling of medullary conus and slight central spinal enhancement. 15 , 16 Characteristic image alterations include serpentine vessels involving the spinal roots and end-on vessels on the sagittal images. Figs. 1 and 2 show sagittal T2-weighted MRI of the spine demonstrating grossly abnormal and tortuous perimedullary vascular flow voids on the dorsal as well as ventral surface of the spinal cord. Flow voids and vascular channels extend inferiorly in the lumbar subarachnoid space and are seen intermingled with the caudal nerve roots (better appreciated on Fig. 2). The distal spinal cord shows diffuse enlargement with T2 hyperintensity suggestive of cord edema involving the central spinal cord with relative sparing of the periphery and flame-shaped margins superiorly and inferiorly. Absence of intramedullary flow void or nidus excludes type II/III/IV spinal arteriovenous malformation. 15
The emergency management of Foix-Alajouanine syndrome is largely empirical with steroids and supportive measures. The gold standard has been direct occlusion of the fistula by coagulation under visual guidance. However, in recent years, endovascular embolization of the affected vessels in the spinal cord has gained considerable acceptance, and the results are very encouraging. 17 The recommended strategy is to use fluid agents and to block both the arterial end and the venous end of the malformation. In many centers across the world, interventional radiographic procedures are practiced as a procedure of choice because it is less invasive and more cost-effective and has excellent outcomes. Early intervention can result in dramatic reversal of neurologic deficits as has occurred in this patient. It has also been reported that diagnostic angiography itself often results in reversal of clinical symptoms.
Conclusions
The significance of this case report is to raise awareness among spine surgeons that Foix-Alajouanine syndrome is one of the differential diagnoses of acute CES that has been hitherto unpublished. The key to the diagnosis is the characteristic MRI appearance and the absence of compressive lesions in the spinal canal. Treatment is by early endovascular embolization.
Disclosures
None